I now have abundant, high-quality source material from Creasy & Resnik's Maternal-Fetal Medicine. Let me now compose the complete, comprehensive CTG teaching lesson.
📋 CARDIOTOCOGRAPHY (CTG) - A Complete Teaching Guide
Sources: Creasy & Resnik's Maternal-Fetal Medicine (Principles and Practice), Williams Obstetrics, DC Dutta's Textbook of Obstetrics
PART 1: WHAT IS A CTG?
Cardiotocography (CTG) is the simultaneous, continuous electronic recording of two things:
- The Fetal Heart Rate (FHR) - the top channel
- Uterine contractions (tonus/tocometry) - the bottom channel
The word comes from: Cardio (heart) + toco (labour/uterus) + graphy (writing/recording).
The machine that produces it is called an Electronic Fetal Monitor (EFM).
The paper strip it produces is called a CTG trace or cardiotocograph.
Why do we do it?
The fetal heart rate is tightly coupled to the fetal neurological and cardiovascular system. Changes in oxygenation, acid-base status, and autonomic nerve activity all reflect on the fetal heart. As Creasy & Resnik state: "FHR monitoring relies on the unique coupling of fetal neurologic status to cardiovascular reflex responses... it has become part of fetal monitoring of labor and delivery."
In short: the CTG is a window into the fetal brain and cardiovascular system. A well-oxygenated fetus has a specific pattern. A hypoxic fetus shows warning signs. A compromised fetus shows alarming patterns.
PART 2: THE PHYSIOLOGY BEHIND CTG
To read a CTG intelligently, you must understand the physiology first.
The Fetal Autonomic Nervous System
The FHR is controlled by two opposing systems:
- Sympathetic nervous system - speeds the heart up
- Parasympathetic (vagus) nerve - slows the heart down
In a healthy fetus, there is constant interplay between these two systems. This is why the FHR is never a flat line - it wiggles up and down constantly. This wiggling is called variability and it is the most important sign of fetal wellbeing.
Oxygen and the Fetal Brain
The fetus gets its oxygen from the mother via the placenta. The pathway is:
- Uterine artery → Intervillous space → Placenta → Umbilical vein → Fetal circulation
During a uterine contraction, uterine blood flow temporarily decreases. A healthy fetus has enough reserve oxygen to withstand this. A compromised fetus cannot.
When fetal PO₂ falls:
- Peripheral chemoreceptors in the fetus detect hypoxaemia
- A vagal discharge is triggered
- This causes a transient slowing of the heart (deceleration)
- The brain also responds by reducing its oxygen consumption
- Variability decreases as brainstem oxygenation falls
This sequence is the physiological basis of all abnormal CTG patterns.
The "Fetal Reserve" Concept
Think of it as a tank of oxygen. A healthy term fetus has a large reserve. A growth-restricted fetus, or one in a mother with preeclampsia, has a small reserve. Each contraction dips into that reserve. When the reserve runs out, the fetus decompensates.
PART 3: HOW THE MACHINE WORKS
The CTG machine has two transducers:
Transducer 1: For Fetal Heart Rate
There are two methods:
A. External (Doppler ultrasound transducer / cardiotachometer)
- Placed on the maternal abdomen over the fetal back/chest
- Emits a high-frequency ultrasound signal (~2.5 MHz)
- Detects movement of cardiac valves or ventricular walls
- Measures the interval between beats (in milliseconds), divides 60 by that interval to give rate in beats per minute
- Uses autocorrelation technology to improve accuracy
- Advantage: non-invasive, easy to apply
- Disadvantage: can lose signal with maternal movements, obesity, or poor fetal positioning
B. Internal (Fetal Scalp Electrode / FSE)
- A small spiral stainless steel wire screwed into the fetal scalp
- Measures the R-wave of the fetal ECG directly
- Gives true beat-to-beat variability - the most accurate method
- Requires ruptured membranes and cervical dilation
- Indication: when external monitoring is inadequate (e.g., maternal obesity)
Transducer 2: For Uterine Contractions (Tocometry)
A. External (Tocodynamometer / TOCO)
- Placed on the fundus of the uterus
- A pressure-sensitive button detects the hardening of the uterus during contractions
- Shows the timing and frequency of contractions but NOT the actual intrauterine pressure
- Cannot measure contraction strength accurately
B. Internal (Intrauterine Pressure Catheter / IUPC)
- A soft plastic transducer-tipped catheter placed transcervically into the amniotic cavity
- Measures actual intrauterine pressure in mmHg
- Baseline uterine tone: ~8-12 mmHg
- During contractions: typically 50-80 mmHg
- Requires ruptured membranes
- Useful when assessing adequacy of contractions (e.g., in failed induction)
The Paper
The CTG paper moves at a standard speed of 1 cm/min (UK) or 3 cm/min (USA). This is important because patterns look different at different speeds. Most UK hospitals use 1 cm/min. At 1 cm/min, each large square = 1 minute. Know your local paper speed before interpreting.
PART 4: THE CTG TRACE - ANATOMY OF THE STRIP
┌─────────────────────────────────────────────────────┐
│ FHR channel (top) y-axis: 50-210 bpm │
│ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ │
│ (wavy line representing fetal heart rate) │
│ │
│ Uterine activity (bottom) y-axis: 0-100 mmHg │
│ ___/\___/\___/\___ (mountains = contractions) │
└─────────────────────────────────────────────────────┘
The top channel runs from 50 to 210 beats per minute (bpm). Normal range is around 110-160 bpm.
The bottom channel shows uterine contractions as gentle mounds (mountains).
PART 5: THE FIVE FEATURES TO ASSESS ON EVERY CTG
This is the systematic approach. Every time you look at a CTG, assess these five features in order. The mnemonic is DR C BRAVADO or simply remember: BRAVADO
| Feature | What you measure |
|---|
| Baseline rate | The average FHR over 10 minutes |
| Rhythm / Regularity | Is it regular? |
| Accelerations | Are there accelerations? |
| Variability | How much does the FHR wiggle? |
| Absent features | Any decelerations? |
| Decelerations | Type and timing |
| Overall assessment | Category I / II / III |
Let's go through each one in great detail.
FEATURE 1: BASELINE FETAL HEART RATE
Definition
The baseline FHR is the mean FHR rounded to the nearest 5 bpm during a 10-minute segment, excluding accelerations, decelerations, and periods of marked variability.
The 10-minute window must contain at least 2 minutes of interpretable baseline (not necessarily contiguous).
Normal Range
110-160 bpm (NICHD/ACOG/FIGO definitions)
Some texts give 120-160 bpm as the older range. The current accepted normal is 110-160 bpm.
Tachycardia
Defined as a baseline FHR >160 bpm persisting for at least 10 minutes.
Causes of fetal tachycardia:
| Category | Causes |
|---|
| Maternal | Fever, infection (chorioamnionitis), thyrotoxicosis, anaemia, anxiety |
| Drug-induced | Beta-agonists (ritodrine, salbutamol), cocaine, methamphetamine, atropine |
| Fetal | Hypoxia (early warning sign), infection, anaemia, fetal arrhythmia |
| Physiological | Prematurity (baseline naturally higher), fetal activity |
Key teaching point from Creasy & Resnik: "Although fetal tachycardia is potentially associated with fetal hypoxia, particularly when it is accompanied by decelerations of the FHR, the more common association is with maternal fever or fetal infection such as chorioamnionitis."
Do not confuse simple tachycardia with fetal tachyarrhythmia - if the FHR exceeds 240 bpm, that is a true arrhythmia (e.g., supraventricular tachycardia) and needs urgent evaluation.
Bradycardia
Defined as a baseline FHR <110 bpm persisting for at least 10 minutes.
Causes:
| Category | Causes |
|---|
| Normal variant | Some fetuses simply run at 105-110 bpm |
| Cardiac | Congenital heart block (e.g., in maternal SLE/anti-Ro antibodies) |
| Drug-induced | Beta-blockers (e.g., propranolol, labetalol), anaesthetic agents |
| Hypoxic | Prolonged, severe hypoxia leading to vagal over-activity |
| Vasovagal | Maternal vasovagal episode, rapid epidural, aortocaval compression |
Key distinction: A prolonged deceleration that establishes a new, lower rate can look like bradycardia. A true baseline bradycardia is when the low rate is the established baseline BETWEEN decelerations.
FEATURE 2: BASELINE VARIABILITY
This is arguably the most important feature on a CTG.
Definition
Baseline variability refers to the fluctuations in the baseline FHR of 2 cycles per minute or greater. It is measured as the amplitude of the fluctuations (the difference between the highest and lowest points within a 1-minute window, excluding accelerations and decelerations).
Types of Variability (NICHD Classification)
| Classification | Amplitude | Clinical Meaning |
|---|
| Absent | Undetectable (<2 bpm) | Severely worrying |
| Minimal | >0 but ≤5 bpm | Worrying if persistent |
| Moderate (Normal) | 6-25 bpm | Normal, reassuring |
| Marked | >25 bpm | Usually benign (saltatory pattern) |
The golden rule: If variability is moderate (6-25 bpm), regardless of what other patterns are present, the fetal brain is adequately oxygenated and the fetus is NOT experiencing metabolic acidosis. This is the most protective sign on a CTG.
From Creasy & Resnik: "If the FHR variability is normal, regardless of what other FHR patterns may be present, the fetus is not experiencing cerebral tissue hypoxemia because the fetus can centralize the available oxygen and is physiologically compensated."
Physiological Basis of Variability
Variability reflects the integrity of the entire arc from:
- Cerebral cortex
- Midbrain
- Vagus nerve
- Cardiac conduction system
It is essentially proof that the fetal brain is alive, awake, and in control of the heart. Loss of variability = the brain is losing control = hypoxia/acidosis developing.
Non-Hypoxic Causes of Reduced Variability
Before calling a flat trace "hypoxic," always consider:
- Fetal sleep cycle - fetuses sleep in 20-40 minute cycles; during quiet sleep, variability physiologically decreases (minimal). A sleep cycle never exceeds 40-60 minutes.
- Narcotics/opioids - pethidine, morphine, fentanyl all suppress CNS and reduce variability (Fig. 33.3 in Creasy & Resnik shows a flat trace in a mother on magnesium sulfate and narcotics with normal scalp pH 7.28)
- Magnesium sulfate - CNS depressant
- Benzodiazepines (diazepam, lorazepam)
- Prematurity - preterm fetuses naturally have lower variability
- Anencephaly - no cortex, no variability
- Complete heart block - defective cardiac conduction
- Atropine/scopolamine - vagal blockade
Clinical rule: If variability is absent and the fetus has received pethidine in the last 2-4 hours, consider a prolonged monitoring period or fetal scalp pH before acting. If variability is absent with no pharmacological explanation AND there are late decelerations, act urgently.
Saltatory Pattern (Marked Variability >25 bpm)
Excessively large amplitude fluctuations. Usually seen transiently during cord compression. Significance uncertain but persistent saltatory pattern with decelerations is concerning.
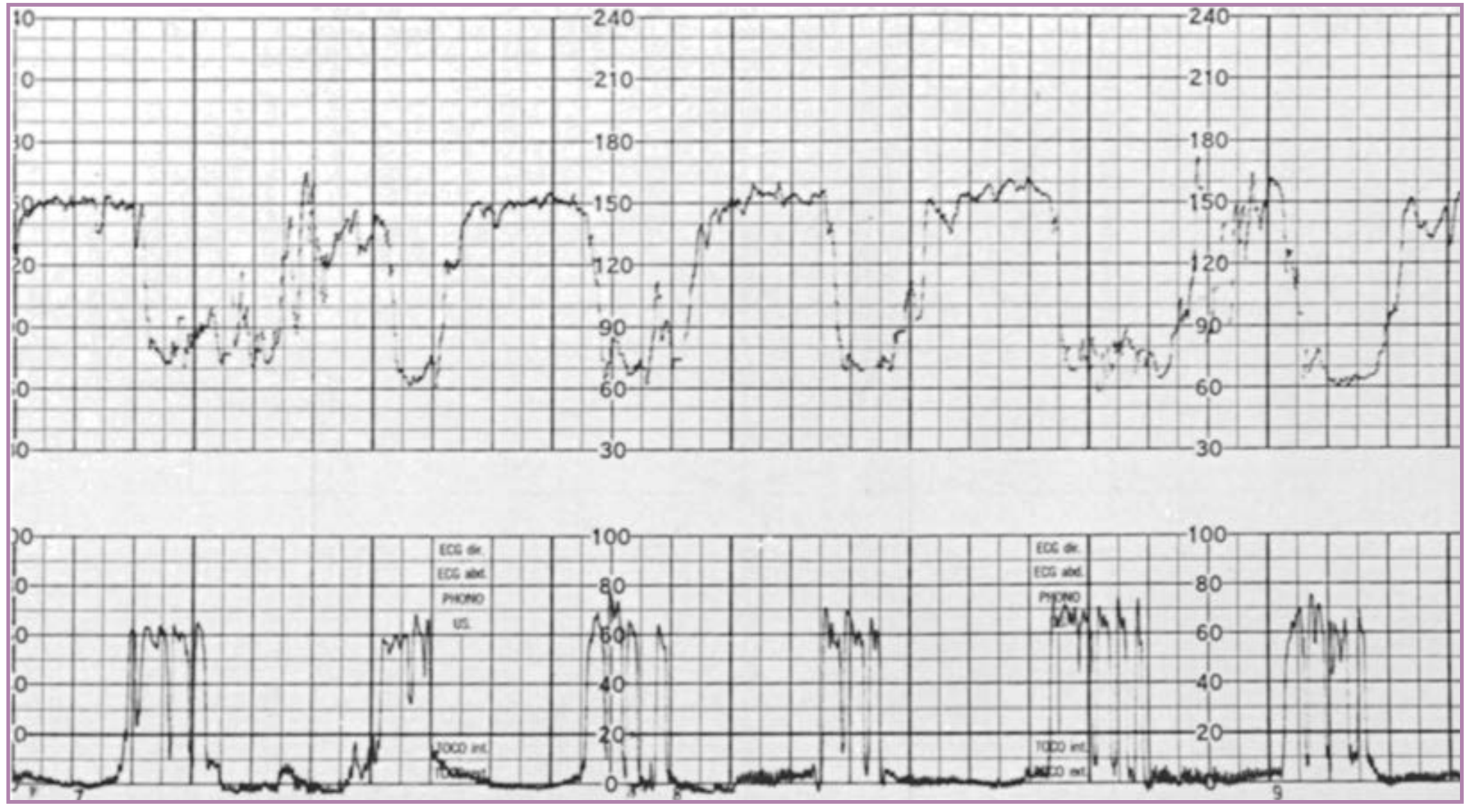
CTG showing variable decelerations with normal baseline variability between decelerations - Creasy & Resnik
FEATURE 3: ACCELERATIONS
Definition
A visually apparent, abrupt increase in FHR above baseline.
For ≥32 weeks gestation:
- Peak ≥ 15 bpm above baseline
- Duration ≥ 15 seconds but < 10 minutes
For < 32 weeks gestation:
- Peak ≥ 10 bpm above baseline
- Duration ≥ 10 seconds
If an acceleration lasts ≥10 minutes, it is classified as a baseline change, not an acceleration.
Significance
Accelerations are the most reliable sign of fetal wellbeing.
They reflect:
- An intact fetal nervous system
- Adequate oxygenation of the CNS
- Fetal movement triggering autonomic activity
The Non-Stress Test (NST) is based entirely on accelerations. A reactive NST = at least 2 accelerations in 20-30 minutes. This is the definition used in the Biophysical Profile.
From Creasy & Resnik: "The classic criteria for a reactive NST are at least two FHR accelerations lasting at least 15 seconds and rising at least 15 beats/min above the established baseline heart rate. Most term fetuses have many of these accelerations in each 20-30 minute period of active sleep."
Absence of Accelerations
When there are NO accelerations on a CTG in labour:
- Does NOT by itself indicate fetal compromise
- However, absence of accelerations alongside other features (reduced variability, decelerations) increases concern
- Requires closer monitoring
Overshoot / Shoulder
A brief acceleration immediately preceding or following a deceleration is called an "overshoot" if it follows a variable deceleration. This is a non-reassuring sign and may indicate hypoxic sympathetic stimulation.
FEATURE 4: DECELERATIONS
A deceleration is a visually apparent decrease in FHR below the baseline. There are four main types. Getting these right is the core clinical skill of CTG interpretation.
Key parameters for any deceleration:
- Onset - abrupt (within <30 seconds) vs. gradual (>30 seconds)?
- Timing - when does the nadir occur relative to the peak of the contraction?
- Duration - seconds
- Depth - nadir below baseline (bpm)
- Variability during/between - does the FHR recover with good variability?
- Uniformity - do they all look the same or are they different each time?
TYPE 1: EARLY DECELERATIONS
Shape: Uniform, smooth, symmetrical U-shape, mirror image of the contraction
Onset: Gradual (>30 sec to nadir)
Timing: Begins WITH the start of the contraction, nadir at the PEAK of contraction, returns to baseline as contraction ends - perfectly in phase
Depth: Usually mild, rarely below 100 bpm
Cause: Fetal head compression against the cervix → vagal stimulation → transient heart rate slowing (Baroreflex)
Clinical significance: BENIGN. Not associated with fetal hypoxia or acidosis. Seen most commonly in active labour with cervical dilation.
Contraction: ___/\___
FHR change: ___\/___ (mirror image = simultaneously occurring)
TYPE 2: LATE DECELERATIONS
This is the most important deceleration type to recognise.
Shape: Uniform, smooth, symmetrical U-shape
Onset: Gradual (>30 sec to nadir)
Timing: Begins AFTER the peak of the contraction, nadir is DELAYED after peak contraction, returns to baseline after the contraction has completely ended
Depth: Can be shallow (even 10-20 bpm below baseline) or deep
Cause: Uteroplacental insufficiency
Contraction: ___/\___
FHR change: ___\/___ (shifted to the right - delayed)
The Physiology of Late Decelerations (in detail from Creasy & Resnik):
There are TWO types of late decelerations:
1. Reflex late decelerations (with GOOD variability)
- Mechanism: Acute drop in uterine blood flow during contraction → placental hypoperfusion → fetal PO₂ drops → fetal chemoreceptors detect hypoxaemia → vagal discharge → heart rate slows
- Timing is late because of the circulation time from placenta to chemoreceptors
- The fetal brain and myocardium still have adequate oxygen (just barely)
- Variability is maintained = brain is still in control = physiologically compensated
- Seen in: acute hypotension, epidural, aortocaval compression, acute blood loss
2. Non-reflex late decelerations (with ABSENT variability)
- Mechanism: The deoxygenated blood from placenta is so profoundly hypoxic that it directly depresses the myocardium + increases vagal activity
- The brain has run out of oxygen too - it can no longer maintain variability
- Variability is absent = fetal decompensation = cerebral and myocardial hypoxia
- Seen in: severe preeclampsia, IUGR, prolonged hypoxia after recurrent late decelerations
From Creasy & Resnik: "Nonreflex late decelerations occur without FHR variability, signifying fetal decompensation - inadequate cerebral and myocardial oxygenation."
Clinical significance: ANY late deceleration is abnormal and requires assessment. Persistent late decelerations, especially with reduced variability, are associated with fetal acidosis and require urgent intervention.
Important: Even shallow late decelerations (only 10-15 bpm) are significant. Depth does not determine pathology - timing does.
TYPE 3: VARIABLE DECELERATIONS
Shape: Variable - each deceleration looks different. Sharp, abrupt, often V-shaped or W-shaped
Onset: Abrupt (< 30 seconds from onset to nadir)
Timing: Variable relationship to contractions - may come before, during, or after
Depth: Variable, can be very deep (down to 60-70 bpm)
Cause: Umbilical cord compression
Typical variable deceleration:
FHR: ____/|\_/|____
Shoulders = brief accelerations before/after deceleration
The Shoulders: Variable decelerations often have brief accelerations immediately before and after them. These "shoulders" are a reassuring sign that the autonomic nervous system is intact.
Physiology:
- Cord compression → increased fetal blood pressure → baroreceptor reflex → vagal activity → heart rate drops
- The abrupt onset reflects the sudden nature of cord occlusion
- Recovery is usually quick once the cord is released
Simple vs. Complicated Variable Decelerations:
| Feature | Simple (Reassuring) | Complicated (Non-reassuring) |
|---|
| Duration | <60 seconds | >60 seconds |
| Depth | <60 bpm nadir | <60 bpm nadir (i.e. drops very deep) |
| Shoulders | Present | Absent |
| Baseline variability | Normal between decelerations | Reduced |
| Recovery | Complete, returns to baseline | Slow, incomplete |
| Post-deceleration overshoot | Absent | Present (prolonged) |
Variable decelerations in 2nd stage: Very common. The fetal head is being compressed and the cord is under intermittent pressure. Brief variable decelerations in 2nd stage with maintained variability are generally acceptable.
TYPE 4: PROLONGED DECELERATIONS
Definition: A fall in FHR of ≥15 bpm lasting ≥2 minutes but <10 minutes
If it lasts ≥10 minutes, it is a baseline change (bradycardia).
Causes:
- Cord prolapse
- Placental abruption
- Maternal hypotension (e.g., post-epidural top-up)
- Uterine hyperstimulation (tachysystole)
- Maternal Valsalva / second-stage pushing
- Vaginal examination stimulating cervical receptors
- Maternal seizure
Clinical significance: Always take a prolonged deceleration seriously. If it lasts >3 minutes with no obvious remediable cause, urgent assessment is needed. If it persists >9 minutes, prepare for immediate delivery.
From Creasy & Resnik: "Among 951 patients who had a terminal deceleration in the study, 98% did not have a neonate with a pH less than 7.10. However, increasing terminal deceleration duration was associated with decreasing umbilical artery pH and increased risk of acidemia."
SINUSOIDAL PATTERN
This is a rare but important pattern.
Definition: A smooth, sine wave-like undulating pattern with a fixed periodicity of 3-5 cycles/minute and an amplitude of 5-15 bpm lasting ≥20 minutes. There are NO accelerations and NO beat-to-beat variability.
Causes:
- Severe fetal anaemia (Rh isoimmunization, fetomaternal haemorrhage, parvovirus B19)
- Fetal hypoxia
- Drug-induced pseudo-sinusoidal: pethidine, butorphanol (this reverses within 30 min)
Key distinction: A TRUE sinusoidal pattern = fetal anaemia until proven otherwise. Requires URGENT evaluation (Kleihauer test, middle cerebral artery Doppler for peak systolic velocity).
PART 6: THE NICHD THREE-TIER CLASSIFICATION SYSTEM (2008)
This is the internationally adopted system by the National Institute of Child Health and Human Development, endorsed by ACOG, for classifying CTG tracings.
CATEGORY I - NORMAL (Reassuring)
ALL of the following:
- Baseline FHR: 110-160 bpm
- Baseline FHR variability: moderate (6-25 bpm)
- Accelerations: present or absent
- Late or variable decelerations: absent
- Early decelerations: present or absent
Meaning: Strongly predictive of normal fetal acid-base status. No action required beyond routine monitoring.
CATEGORY II - INDETERMINATE (Requires Evaluation)
All tracings that are NOT Category I or Category III fall here. Examples include:
- Baseline tachycardia
- Baseline bradycardia (not Category III)
- Minimal variability (without decelerations)
- Absent variability (without recurrent decelerations)
- Marked (saltatory) variability
- Absence of induced accelerations after fetal scalp stimulation
- Recurrent variable decelerations with minimal or moderate variability
- Prolonged deceleration >2 minutes but <10 minutes
- Recurrent late decelerations with moderate variability
- Variable decelerations with other features (slow return, "overshoots," shoulders)
Meaning: Insufficient evidence to classify as normal or abnormal. Requires continued surveillance, evaluation for remediable causes, and possible escalation.
CATEGORY III - ABNORMAL (Requires Prompt Action)
Either of the following:
- Sinusoidal pattern, OR
- Recurrent late decelerations with absent baseline variability, OR
- Recurrent variable decelerations with absent baseline variability, OR
- Bradycardia with absent baseline variability
Meaning: Associated with abnormal fetal acid-base status. Requires PROMPT evaluation and delivery if the pattern cannot be corrected.
THE UK SYSTEM: NICE GUIDELINES (for comparison)
The UK NICE guidelines classify CTG features as:
| Feature | Reassuring | Non-reassuring | Abnormal |
|---|
| Baseline | 110-160 bpm | 100-109 bpm or 161-180 bpm | <100 or >180 bpm; sinusoidal |
| Variability | ≥5 bpm | <5 bpm for 30-90 min | <5 bpm for >90 min |
| Decelerations | None or early | Variable for <90 min OR late for <30 min | Atypical variable or late for >30 min |
| Accelerations | Present | Absent | - |
Then the overall CTG is classified as:
- Normal - all four features reassuring
- Suspicious - one non-reassuring feature
- Pathological - two or more non-reassuring OR one or more abnormal features
PART 7: DECELERATIONS COMPARED - QUICK REFERENCE TABLE
| Feature | Early | Late | Variable | Prolonged |
|---|
| Onset | Gradual | Gradual | Abrupt | Either |
| Timing vs contraction | Simultaneous (mirrors it) | AFTER contraction | Variable/random | >2 min after onset |
| Shape | Uniform, U | Uniform, U | V or W, irregular | Deep, prolonged |
| Duration | = contraction | Outlasts contraction | <2 min usually | 2-10 min |
| Cause | Head compression | Uteroplacental insufficiency | Cord compression | Multiple |
| Significance | Benign | Pathological | Depends on features | Serious |
| Variability | Normal | Normal (reflex) or absent (non-reflex) | Normal between | Depends |
PART 8: FETAL ACID-BASE STATUS - WHAT THE CTG PREDICTS
Understanding the acid-base connection is what makes CTG clinically meaningful.
Fetal Acidaemia Thresholds (Creasy & Resnik)
| Umbilical Artery pH | Clinical Significance |
|---|
| >7.20 | Normal |
| 7.10-7.20 | Mild acidaemia, usually no adverse outcome |
| 7.00-7.10 | Significant acidaemia, increasing risk of neonatal complications |
| <7.00 | Pathological acidaemia - associated with 8% neonatal death, 9.2% seizures |
Note: Mean umbilical artery pH at birth is ~7.27-7.28 (SD ~0.07).
The critical pH threshold for meaningful morbidity is 7.00. Below this, rates of seizures and neonatal death rise significantly (Goldaber et al., 1991).
Base deficit >12 mmol/L = significant metabolic acidosis even if pH is borderline.
Types of Fetal Acidaemia
| Type | pH | PCO₂ | HCO₃⁻ | Cause |
|---|
| Respiratory | ↓ | ↑↑ | Normal | Acute cord compression, short duration |
| Metabolic | ↓ | Normal | ↓↓ | Prolonged hypoxia, anaerobic metabolism |
| Mixed | ↓ | ↑ | ↓ | Both mechanisms together |
Respiratory acidosis is usually acute and reversible. It occurs with sudden cord compression or uterine hyperstimulation.
Metabolic acidosis is the dangerous type. It builds up slowly with prolonged hypoxia. The pH may fall to 7.00 or below, and base deficit rises. This is associated with hypoxic-ischaemic encephalopathy (HIE).
PART 9: CLINICAL MANAGEMENT - WHAT TO DO
For Category I (Normal)
- Continue routine monitoring
- Document regularly (every 30-60 min)
For Category II (Indeterminate)
Step 1 - Correct remediable causes (Intrauterine Resuscitation):
| Problem | Action |
|---|
| Maternal position (aortocaval compression) | Left lateral tilt / full left lateral position |
| Maternal hypotension (post-epidural) | IV fluid bolus, ephedrine/phenylephrine if needed |
| Uterine hyperstimulation | Stop oxytocin, consider tocolysis (terbutaline 0.25 mg SC) |
| Cord prolapse | Emergency delivery |
| Maternal hypoxia | Give supplemental oxygen (though recent evidence shows limited benefit on fetal pH) |
Step 2 - Fetal Scalp Stimulation (FSS) / Allis clamp test:
- Apply pressure or Allis clamp to fetal scalp through the dilated cervix
- A resulting acceleration = pH >7.20 (NPV ~99%)
- No acceleration = indeterminate, may need further assessment
Step 3 - Fetal Scalp Blood Sampling (FBS) - where available:
- Scalp pH >7.25 = normal (repeat in 1 hour if CTG still abnormal)
- Scalp pH 7.20-7.25 = borderline (repeat in 30 min)
- Scalp pH <7.20 = acidaemia → expedite delivery
From Creasy & Resnik: "Fetal scalp blood sampling is no longer an option in most hospitals providing obstetric care" (due to quality assurance issues and procedural challenges).
For Category III (Abnormal)
Immediate actions (all simultaneously):
- Left lateral position
- Stop oxytocin
- IV fluid bolus
- Supplemental oxygen (face mask)
- Call senior obstetrician
- If no improvement in 10-15 min → expedite delivery
- Category 1 (crash) caesarean if immediate danger
- Or assisted vaginal delivery if feasible and rapid
PART 10: SPECIAL SITUATIONS
Prematurity
- Preterm fetuses (<32 weeks) have higher baseline rates and lower variability as a baseline feature
- Accelerations are smaller (10 bpm, 10 seconds qualifies as reactive)
- Late decelerations still carry the same significance
- Interpretation must be modified for gestational age
Multiple Pregnancy
- Two separate CTG traces needed for twins
- Difficult to distinguish the two in external monitoring
- Use FSE on presenting twin if possible
- Variable decelerations are more common in monochorionic twins due to cord entanglement
Second Stage of Labour
- Variable decelerations are very common due to cord compression by the descending head
- The important questions are: Is variability maintained? Are decelerations recovering completely? Is the baseline stable?
- Brief (< 60 seconds), uncomplicated variable decelerations with maintained variability in the second stage are acceptable
- Prolonged variable decelerations or those with loss of variability require action
Post-dates Pregnancy
- Placental reserve declines after 40-42 weeks
- Late decelerations are more significant
- Oligohydramnios (reduced liquor) increases cord compression risk
- CTG alone is insufficient for post-dates surveillance - combine with AFI/BPP
PART 11: SYSTEMATIC APPROACH TO READING A CTG - STEP BY STEP
Every time you pick up a CTG trace, use this approach:
Step 1: Confirm patient details, gestational age, date/time, paper speed
Step 2: Look at the overall picture - do you see a reassuring or worrying trace at a glance?
Step 3: Assess baseline rate - is it 110-160? Is it tachycardic or bradycardic?
Step 4: Assess variability - 6-25 bpm (moderate)? Minimal? Absent?
Step 5: Look for accelerations - present? How many?
Step 6: Identify decelerations - what type? Early, late, variable, prolonged?
- For each deceleration: when does it start relative to contraction? When does it reach nadir? How deep? How long? What is variability doing?
Step 7: Look at uterine activity - how frequent are contractions? Any hyperstimulation (>5 in 10 min)?
Step 8: Classify - Category I, II, or III?
Step 9: Document your interpretation with timestamp and action taken
PART 12: LIMITATIONS OF CTG
CTG is NOT a perfect test. This is important to understand.
From Creasy & Resnik: "Several well-designed randomized clinical studies from different clinical centers involving almost 40,000 women in labor have demonstrated that intrapartum EFM does not result in any measurable improvement in outcomes compared with intermittent auscultation."
Key limitations:
- High false positive rate - many abnormal CTGs are in non-acidotic fetuses
- Poor interobserver agreement - two clinicians may classify the same trace differently
- The only proven benefit is reduction in neonatal seizures (not long-term neurological outcomes)
- The rate of caesarean section increased dramatically after CTG was introduced
- EFM does NOT significantly reduce perinatal death, cerebral palsy, or HIE
- Only 0.19% of children with abnormal FHR findings developed cerebral palsy (Creasy & Resnik)
Why still use CTG then?
- It remains the best available tool for continuous intrapartum surveillance
- It has high sensitivity (few missed hypoxic events)
- Combined with fetal scalp stimulation, it has good NPV
- Practical and non-invasive
- Alternative (intermittent auscultation) is labour-intensive and not feasible in high-risk cases
PART 13: CTG IN ANTENATAL PERIOD - THE NON-STRESS TEST (NST)
CTG is not just for labour. In the antenatal period, it is used as the NST.
Reactive NST
- 2 accelerations in 20-30 min (each ≥15 bpm, ≥15 sec at term; or ≥10 bpm, ≥10 sec before 32 weeks)
- Falsely reassuring (false negative) rate: ~1.9 per 1000 fetuses per week (excellent)
Non-reactive NST
- Does not meet criteria after 40 minutes
- Proceed to biophysical profile (BPP) or contraction stress test (CST)
- About 10-12% of third trimester fetuses are non-reactive at 30 min (usually due to sleep cycle)
Contraction Stress Test (CST)
- Nipple stimulation or oxytocin infusion to produce at least 3 contractions in 10 minutes
- Negative (normal): No late decelerations
- Positive (abnormal): Late decelerations with ≥50% of contractions
- Suspicious: Intermittent late decelerations
- A positive CST indicates uteroplacental insufficiency
SUMMARY MEMORY AID
NORMAL CTG (Category I):
- Baseline: 110-160 bpm
- Variability: 6-25 bpm (moderate)
- Accelerations: present
- Decelerations: none (or only early)
- "All is well"
WARNING SIGNS (look for):
- Rising baseline (early hypoxia → tachycardia)
- Falling variability (brain struggling)
- Loss of accelerations
- Late decelerations (uteroplacental failure)
- Deep/prolonged variable decelerations
- Sinusoidal pattern (anaemia)
THE SINGLE MOST IMPORTANT FEATURE:
→ VARIABILITY. Good variability protects everything else.
→ Even with late decelerations: if variability is good = reflex = brain compensated.
→ Absent variability + ANY decelerations = decompensated = emergency.
References
- Creasy RK, Resnik R et al. Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, 9th Edition. Elsevier. Chapters 32 & 33: Fetal Heart Rate Monitoring, Acid-Base Assessment.
- Williams Obstetrics (Cunningham et al.) - Electronic Fetal Monitoring chapter
- DC Dutta. Textbook of Obstetrics, 10th Edition - Fetal Surveillance chapter
- NICHD Workshop Report (2008) - Three-tier FHR classification system (ACOG)
- NICE Guideline CG190 - Intrapartum Care for Healthy Women and Babies (UK)
- Goldaber KG et al. Pathologic fetal acidemia. Obstet Gynecol. 1991;78:1103.
That is the complete CTG teaching guide. If you want, I can drill down deeper into any specific section - for example, practice trace interpretation, the biophysical profile scoring system, the STAN (fetal ECG ST analysis) adjunct, or management algorithms for specific clinical scenarios. Just say the word.