Thyroid gland
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Gray's Anatomy, Guyton & Hall, Junqueira's Histology, and Robbins Pathology. I have enough to write a thorough, well-illustrated overview. Let me compose the final answer.
The Thyroid Gland
A comprehensive overview drawn from Gray's Anatomy for Students, Guyton & Hall Textbook of Medical Physiology, Junqueira's Basic Histology, and Robbins & Cotran Pathologic Basis of Disease.
1. Anatomy
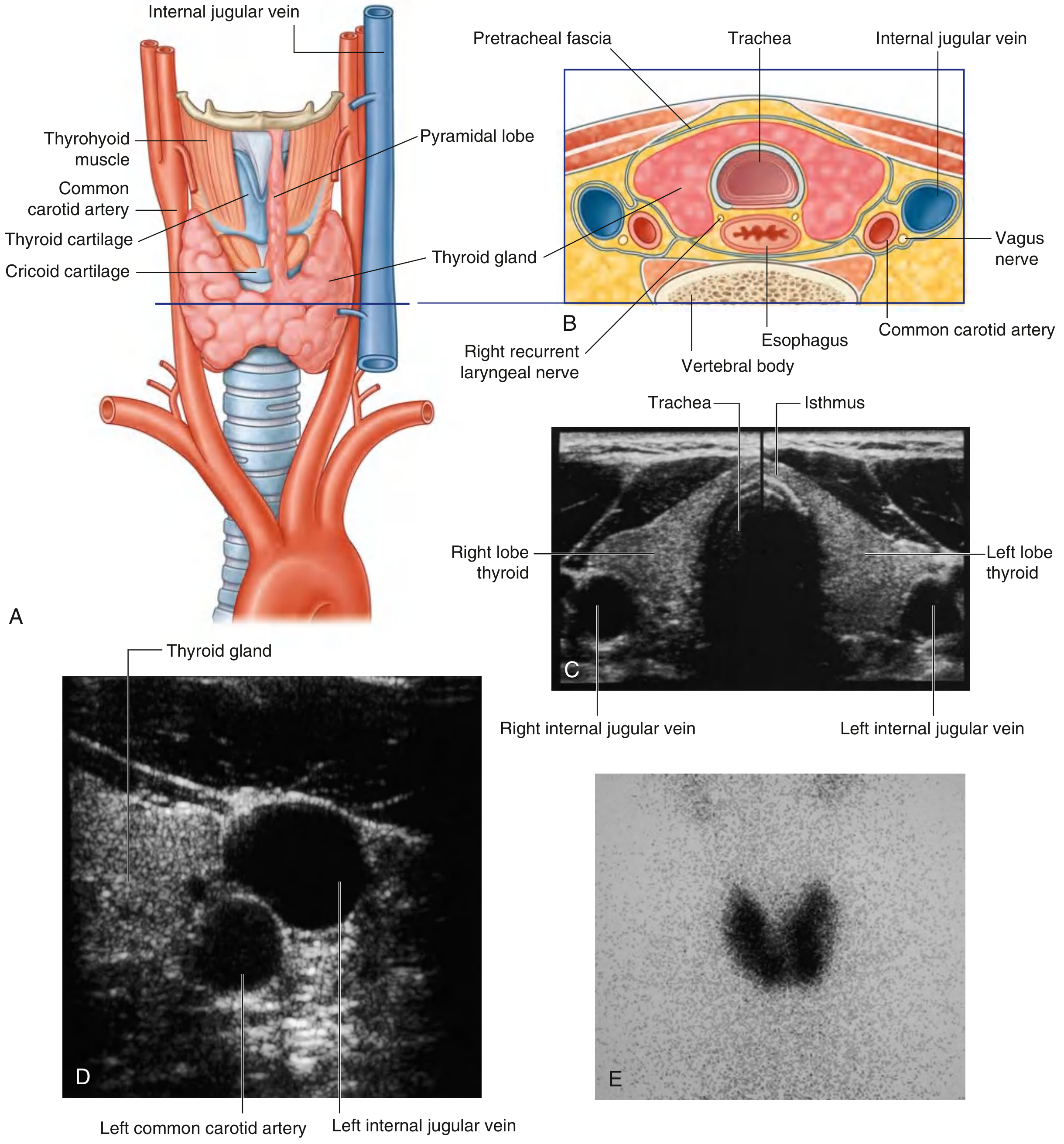
The thyroid gland lies anterior in the neck, below and lateral to the thyroid cartilage. It consists of two lateral lobes joined by an isthmus that crosses the anterior surfaces of the 2nd and 3rd tracheal cartilages. The gland sits within the visceral compartment of the neck (surrounded by the pretracheal fascia), deep to the sternohyoid, sternothyroid, and omohyoid muscles.
Embryology
The gland arises as a median outgrowth (evagination) of the pharyngeal epithelium at the foramen cecum at the base of the tongue. It descends via the thyroglossal duct to its final position in the anterior neck. Remnants may persist as:
- A thyroglossal duct cyst
- A lingual thyroid (ectopic at base of tongue)
- A pyramidal lobe (extending upward from the isthmus)
(Gray's Anatomy for Students, p. 1157)
Blood Supply
Arterial:
- Superior thyroid artery - first branch of the external carotid artery; divides into anterior and posterior glandular branches at the superior pole
- Inferior thyroid artery - branch of the thyrocervical trunk (from the first part of the subclavian artery); supplies the lower pole and the parathyroid glands
- Occasionally, a small thyroid ima artery arises from the brachiocephalic trunk or arch of the aorta
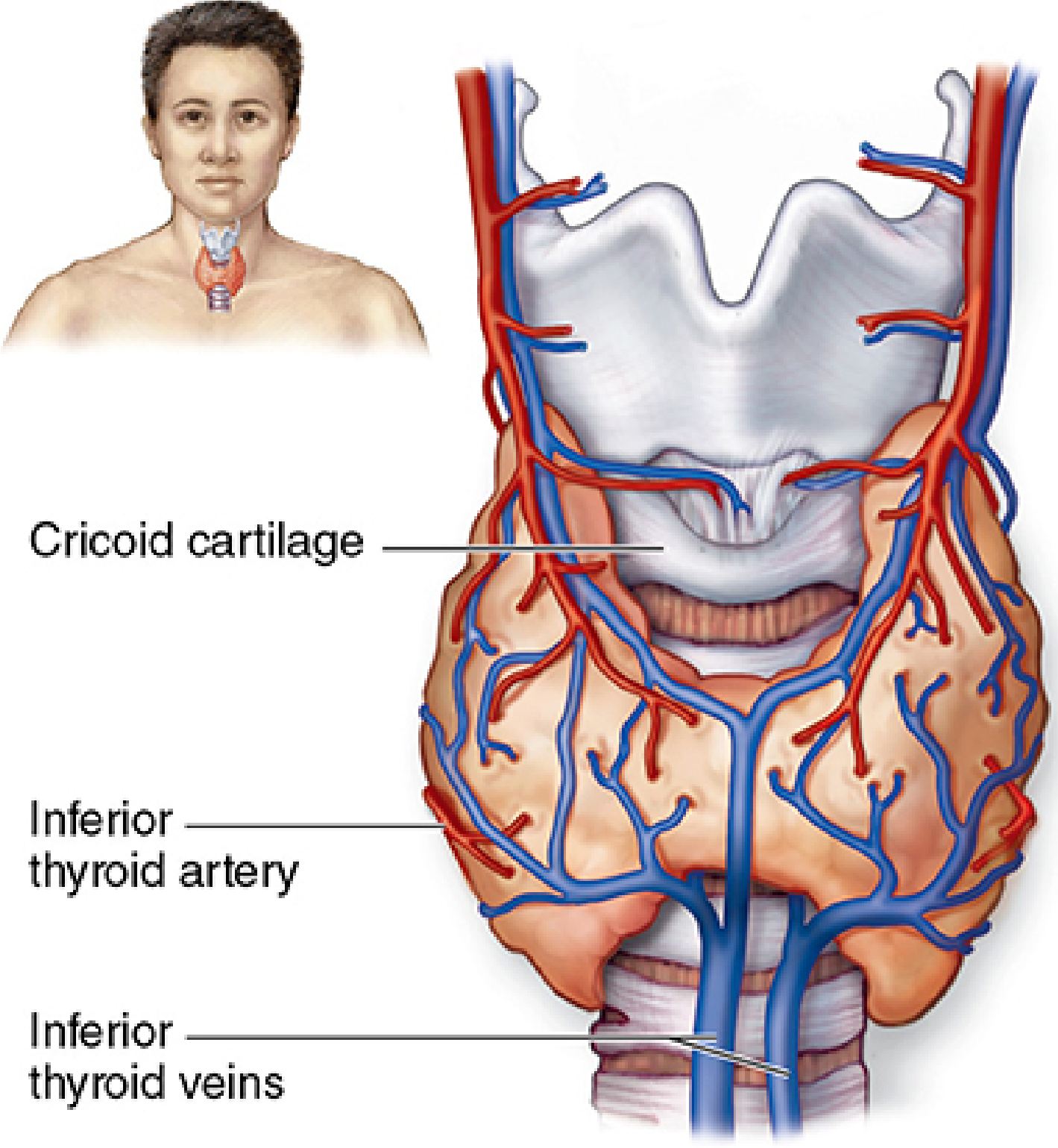
Venous:
- Superior and middle thyroid veins drain into the internal jugular vein
- Inferior thyroid veins drain into the right and left brachiocephalic veins
Lymphatic drainage: To paratracheal nodes and deep cervical nodes along the internal jugular vein.
Recurrent Laryngeal Nerves
The recurrent laryngeal nerves (branches of vagus [CN X]) ascend in the groove between the trachea and esophagus and are closely related to the posterior surface of the thyroid - they are at risk during thyroid surgery. (Gray's Anatomy for Students, p. 1159)
2. Histology
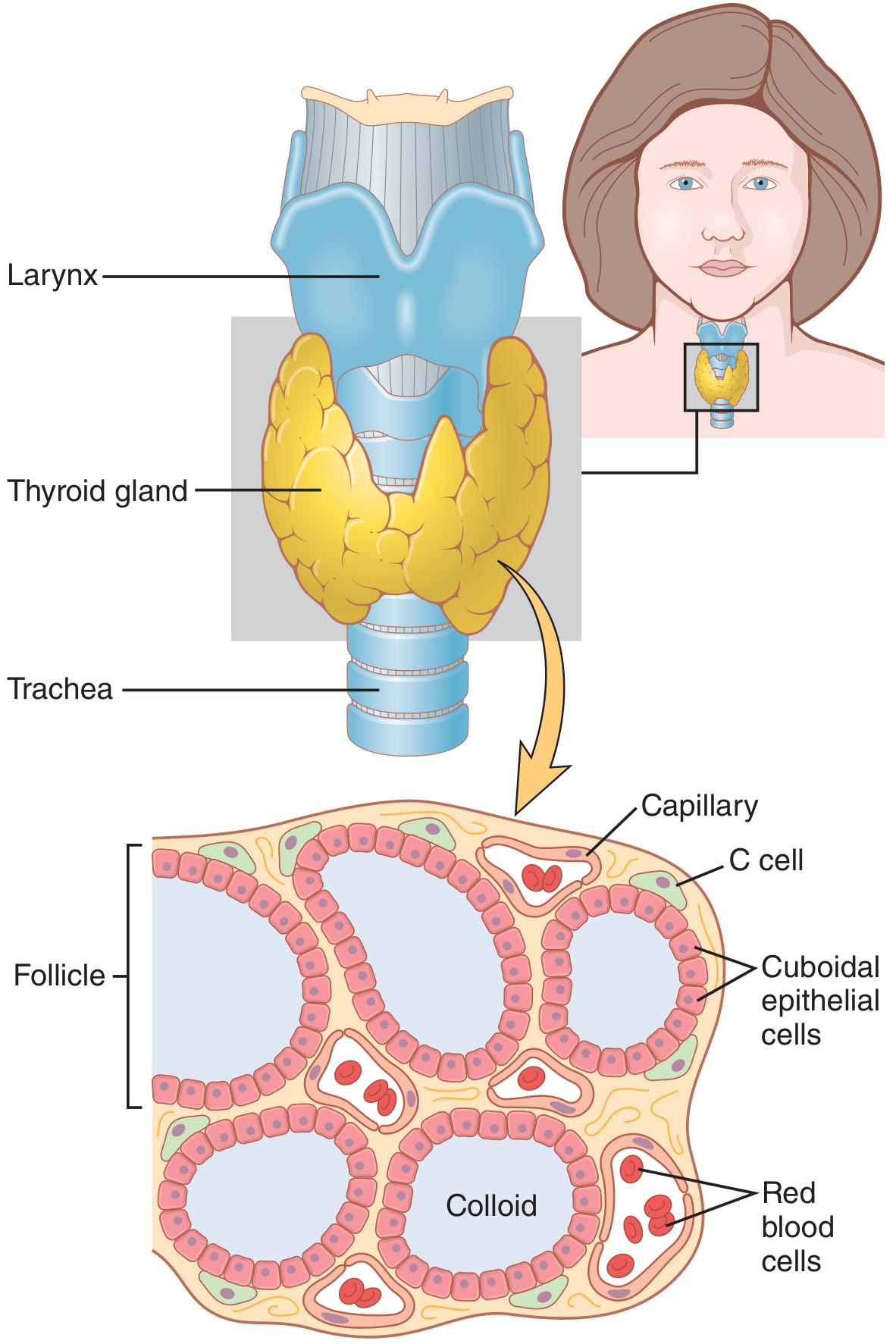
The thyroid parenchyma consists of millions of thyroid follicles - spherical structures lined by simple epithelium (follicular cells / thyrocytes) with a central lumen filled with gelatinous acidophilic colloid.
Key cell types
| Cell | Features | Function |
|---|---|---|
| Follicular cells (thyrocytes) | Cuboidal to low columnar; size varies with activity | Synthesize T3 and T4 |
| Parafollicular cells (C cells) | Larger, pale cells between follicles | Secrete calcitonin |
- Active gland: more follicles with tall columnar epithelium; smaller follicles with less colloid
- Inactive gland: mostly flat/squamous follicular epithelium; large follicles distended with colloid
- The thyroid is the only endocrine gland that stores a large quantity of hormone outside its cells (in the colloid), sufficient for up to 3 months of body supply
- Colloid contains thyroglobulin (660 kDa glycoprotein), the precursor for T3 and T4
- The stroma contains fenestrated capillaries for rapid hormone transfer to blood
(Junqueira's Basic Histology, p. 1034-1035)
3. Hormone Synthesis
The thyroid produces:
- Thyroxine (T4) - tetraiodothyronine
- Triiodothyronine (T3) - more potent (10x greater receptor affinity than T4)
- Calcitonin - from C cells; promotes calcium absorption by skeleton, inhibits osteoclast bone resorption
Iodine Requirement
About 50 mg of iodine per year (or ~1 mg/week) is required for normal T4 production. Common table salt is iodized with ~1 part NaI per 100,000 parts NaCl to prevent deficiency. (Guyton & Hall, p. 930)
Steps of T3/T4 Synthesis
| Step | What Happens |
|---|---|
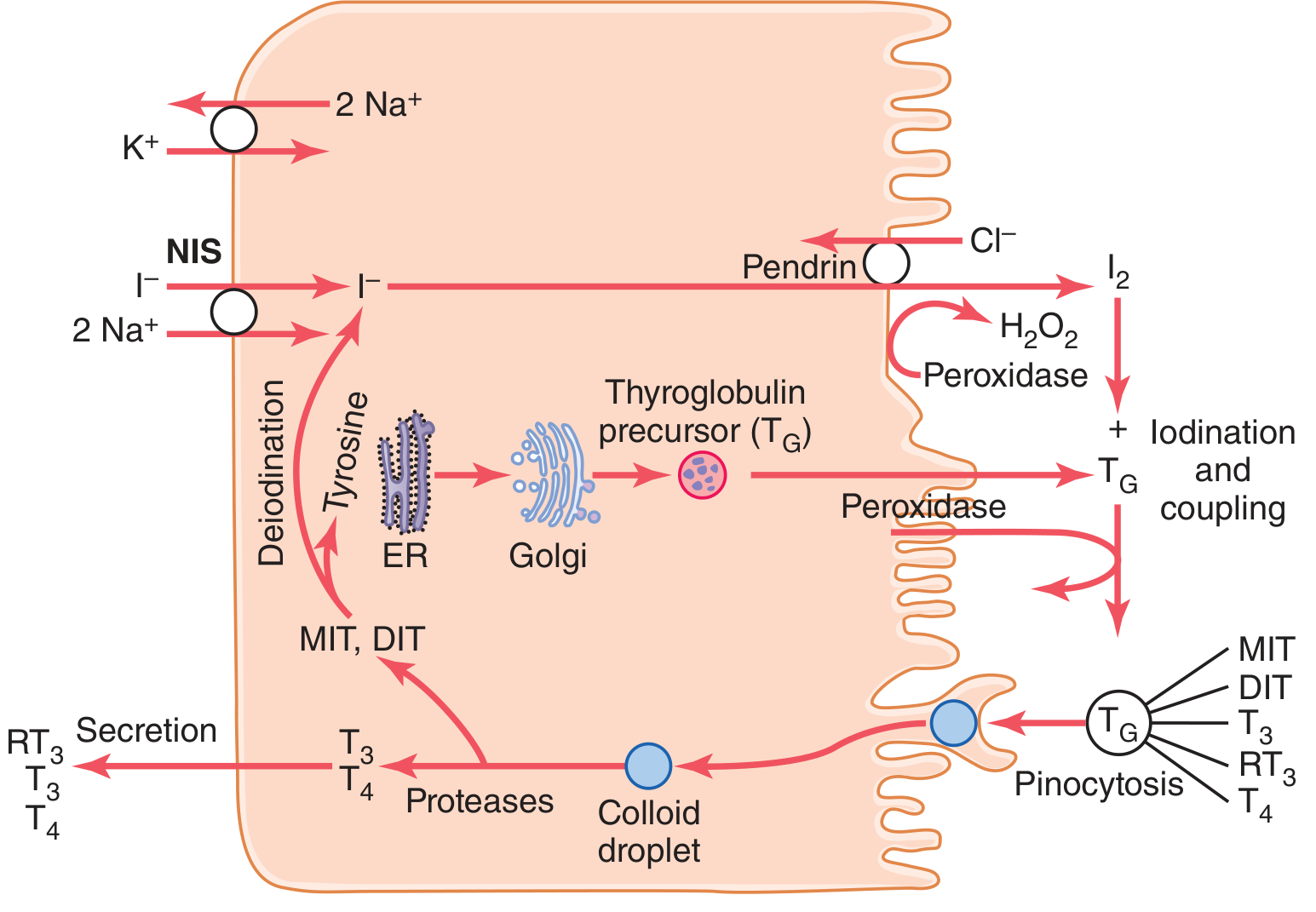
| 1. Iodide trapping | Na-I symporter (NIS) on basolateral membrane co-transports I⁻ with 2 Na⁺ into the cell (driven by Na⁺-K⁺-ATPase). Normal gland concentrates iodide ~30x blood level; hyperactive gland up to 250x |
| 2. Iodide transport to follicle | Iodide crosses the apical membrane via pendrin (chloride-iodide counter-transporter) |
| 3. Oxidation | Thyroid peroxidase (TPO) + H₂O₂ oxidize I⁻ → I₂ (nascent iodine) at the apical membrane |
| 4. Organification | Oxidized iodine binds tyrosine residues on thyroglobulin → monoiodotyrosine (MIT) then diiodotyrosine (DIT) |
| 5. Coupling | DIT + DIT → T4; MIT + DIT → T3 (within thyroglobulin) |
| 6. Storage | Iodinated thyroglobulin stored in colloid |
| 7. Secretion | TSH stimulates pinocytosis of colloid → proteases cleave T3/T4 from thyroglobulin → T3/T4 secreted into blood |
| 8. Deiodination | Uncoupled MIT and DIT are deiodinated; iodide recycled within the cell |
(Guyton & Hall, p. 930-931)
4. Regulation (HPT Axis)
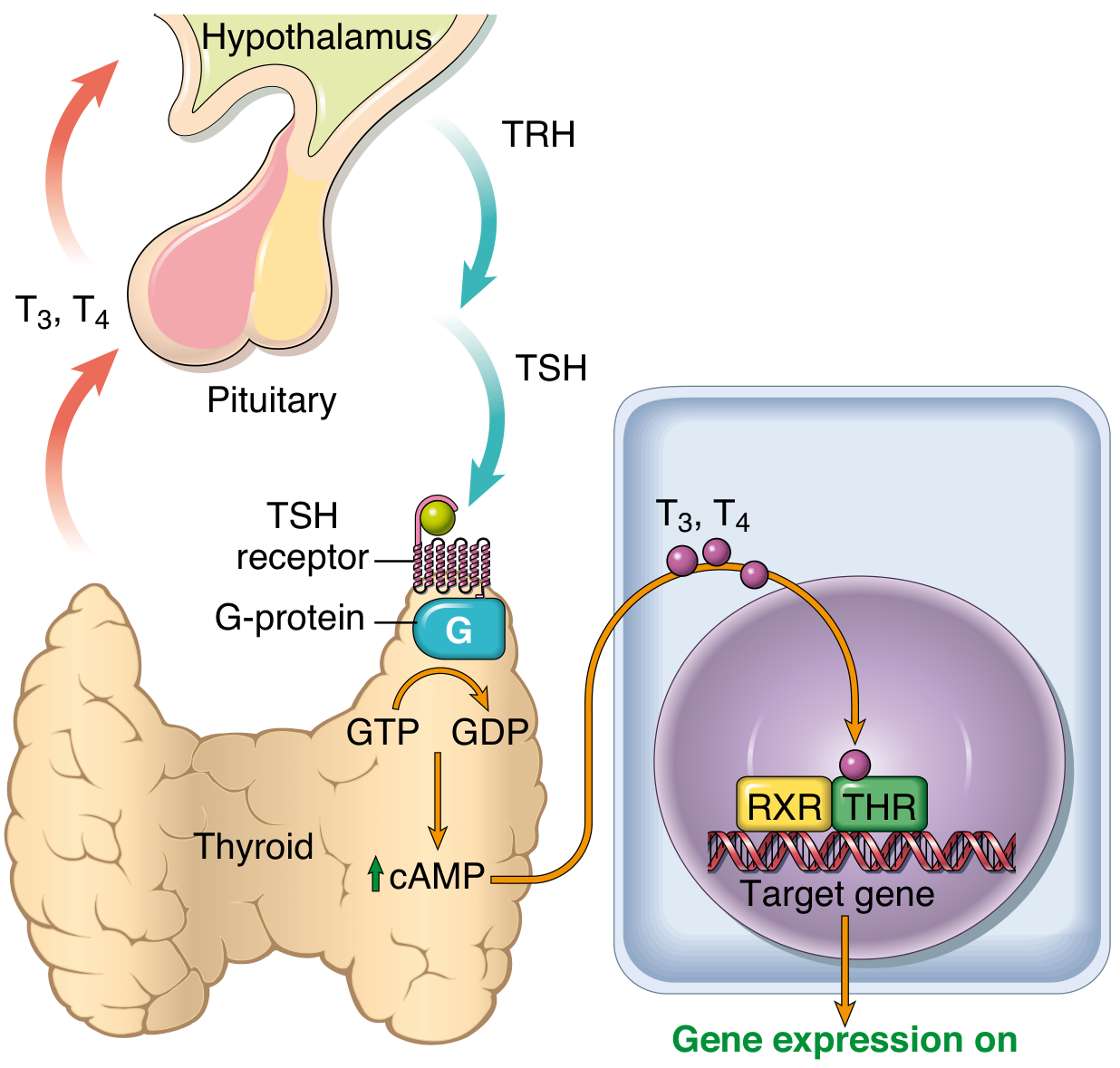
- Hypothalamus releases TRH (thyrotropin-releasing hormone)
- Anterior pituitary releases TSH (thyrotropin)
- TSH binds its receptor on follicular cells → Gs protein → ↑ cAMP → stimulates thyroid hormone synthesis and release
- Elevated T3/T4 negatively feed back to suppress TRH and TSH
In the periphery, T4 is deiodinated to the more active T3. T3 enters the nucleus, binds thyroid hormone receptor (THR), which heterodimerizes with RXR, and activates thyroid response elements on target genes. (Robbins & Cotran, p. 995)
5. Functions of Thyroid Hormones
Thyroid hormones increase transcription of hundreds of genes, producing a generalized increase in metabolic activity throughout the body.
| System | Effect |
|---|---|
| Metabolism | ↑ basal metabolic rate; stimulate carbohydrate and lipid catabolism; ↑ protein synthesis |
| Cardiovascular | ↑ heart rate, cardiac output, and blood flow |
| Nervous system | Critical for fetal and neonatal brain development; deficiency → cretinism |
| Growth | Required for normal skeletal growth and maturation |
| Heat production | Calorigenic effect - increase body temperature |
Onset and duration: T4 has a latent period of 2-3 days before effect is seen, peaking at 10-12 days (half-life ~15 days). T3 acts ~4x faster (onset 6-12 hours, peak 2-3 days). Both are >99% plasma-protein bound (mainly to thyroxine-binding globulin). (Guyton & Hall, p. 930)
6. Goitrogens & Antithyroid Agents
Chemical agents that suppress thyroid hormone synthesis lead to ↑ TSH and compensatory hyperplastic enlargement (goiter):
- Propylthiouracil (PTU) and methimazole - block iodide oxidation (inhibit TPO); PTU also blocks peripheral conversion of T4 → T3
- Large doses of iodide - paradoxically block thyroid hormone release (Wolff-Chaikoff effect)
7. Pathology Overview
(Robbins & Cotran Pathologic Basis of Disease, p. 995-996)
| Category | Examples |
|---|---|
| Hyperthyroidism (Thyrotoxicosis) | Graves disease (~85% of cases), hyperfunctional multinodular goiter, toxic adenoma |
| Hypothyroidism | Hashimoto thyroiditis (autoimmune), iodine deficiency, post-thyroidectomy |
| Thyroiditis | Hashimoto, subacute (De Quervain), Riedel |
| Goiter | Diffuse or multinodular; iodine deficiency or dyshormonogenesis |
| Neoplasms | Papillary, follicular, medullary (from C cells), anaplastic carcinoma |
Graves disease is the most common cause of hyperthyroidism and is mediated by TSH receptor autoantibodies that constitutively activate the receptor. Hypothyroidism is most commonly caused by Hashimoto thyroiditis in iodine-sufficient regions.
Sources:
- Gray's Anatomy for Students, 4th Ed., p. 1157-1159
- Guyton and Hall Textbook of Medical Physiology, p. 930-931
- Junqueira's Basic Histology, 17th Ed., p. 1034-1035
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 995-996
This is a shared conversation. Sign in to Orris to start your own chat.