Details about PDA
Reading File
Finding Sources
Finding Sources
Searching PubMed
"patent ductus arteriosus"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full, detailed answer:
Patent Ductus Arteriosus (PDA)
Definition & Anatomy
The ductus arteriosus is a fetal vascular channel derived from the sixth aortic arch. It connects the main (or left) pulmonary artery to the upper descending thoracic aorta, just distal to the origin of the left subclavian artery. In fetal life, it carries about 60% of combined ventricular output, directing blood from the pulmonary artery to the aorta, bypassing the unexpanded, high-resistance lungs.
A PDA occurs when this channel fails to close after birth. The ductal lumen may range from 2-8 mm in length and 4-12 mm in diameter.
- Schwartz's Principles of Surgery, 11th Ed. - SCHWARTZ'S PRINCIPLES OF SURGERY 2-volume Set 11th Edition
- Robbins & Kumar Basic Pathology - Robbins & Kumar Basic Pathology
Normal Ductal Closure
After birth, several mechanisms drive closure:
| Factor | Role |
|---|---|
| Rising arterial O2 tension | Primary stimulus for smooth muscle contraction |
| Decreased PGE2 / PGI2 | Placenta (major source) is removed; increased pulmonary blood flow metabolizes these prostaglandins |
| Histamines, catecholamines, bradykinin, acetylcholine | Promote ductal contraction |
Functional closure occurs within 10-15 hours postnatally. Complete anatomic obliteration by fibrosis produces the ligamentum arteriosum within the first few months.
Why PDA Persists - Pathogenesis
| Cause | Mechanism |
|---|---|
| Prematurity | Ductal smooth muscle immaturity; low O2 levels |
| Hypoxia / high altitude | Decreased oxygen tension prevents contraction |
| Respiratory distress syndrome | Surfactant deficiency → hypoxia → PDA |
| Maternal rubella infection | Teratogenic damage to ductal tissue |
| Chromosomal anomalies | Associated with complex CHD |
| TGF-β failure (proposed) | Failure of post-birth TGF-β induction |
Incidence: ~1 in 2000 births overall. In premature infants, up to 75% of infants born at 28-30 weeks have PDA. Female predominance: 2:1 ratio.
Virtually all preterm neonates ≤28 weeks with birth weight <1750 g have PDA in the first 24 hours of life.
- The Developing Human - Clinically Oriented Embryology
Pathophysiology & Hemodynamics
Since aortic pressure exceeds pulmonary artery pressure after birth, blood flows left-to-right (aorta → pulmonary artery) continuously throughout the cardiac cycle.
Consequences depend on ductus size:
| PDA Size | Hemodynamic Effect | Clinical Result |
|---|---|---|
| Small | Minimal shunt, no LV dilation | Asymptomatic; murmur only; risk of endarteritis ~0.45%/year |
| Moderate/Large (restrictive) | Significant L→R shunt; LV/LA dilation; variable PH | Dyspnea, palpitations, exercise intolerance by 2nd-3rd decade |
| Large (non-restrictive) | Massive L→R; pulmonary hypertension develops | May progress to Eisenmenger syndrome |
The diastolic runoff lowers aortic diastolic pressure → widened pulse pressure and bounding pulses. Left ventricular volume overload leads to tachycardia, tachypnea, and ventricular hypertrophy. By the 4th decade, mortality rises to 3-4%/year, with two-thirds of patients dying by age 60 if untreated.
Eisenmenger syndrome (reversal to right-to-left shunt) develops in ~5% of isolated PDA cases. When this occurs, deoxygenated blood from the pulmonary artery enters the descending aorta, causing differential cyanosis and clubbing - more prominent in the toes than the fingers.
- Goldman-Cecil Medicine, International Edition
Clinical Features
Symptoms
- Small PDA: asymptomatic
- Large PDA: dyspnea, palpitations, exercise intolerance, respiratory infections, CHF
Signs
- Widened pulse pressure, bounding peripheral pulses
- Hyperactive/hyperdynamic precordium
- Classic "machinery murmur" (continuous, systolic + diastolic) heard best at the 1st-2nd left intercostal space below the left clavicle
- As pulmonary pressure rises, the diastolic component shortens; in Eisenmenger physiology, the murmur may disappear entirely
Investigations
| Test | Findings |
|---|---|
| CXR | Increased pulmonary vascularity, cardiomegaly (see image below) |
| ECG | LV strain, left atrial enlargement, possible RV hypertrophy |
| Echocardiography | Gold standard - demonstrates ductal patency and estimates shunt size with color Doppler |
| Cardiac catheterization | Reserved for cases with suspected pulmonary hypertension |
| CMR | Useful in older patients to visualize and quantify shunt |
Chest X-ray - Before and After PDA Ligation:
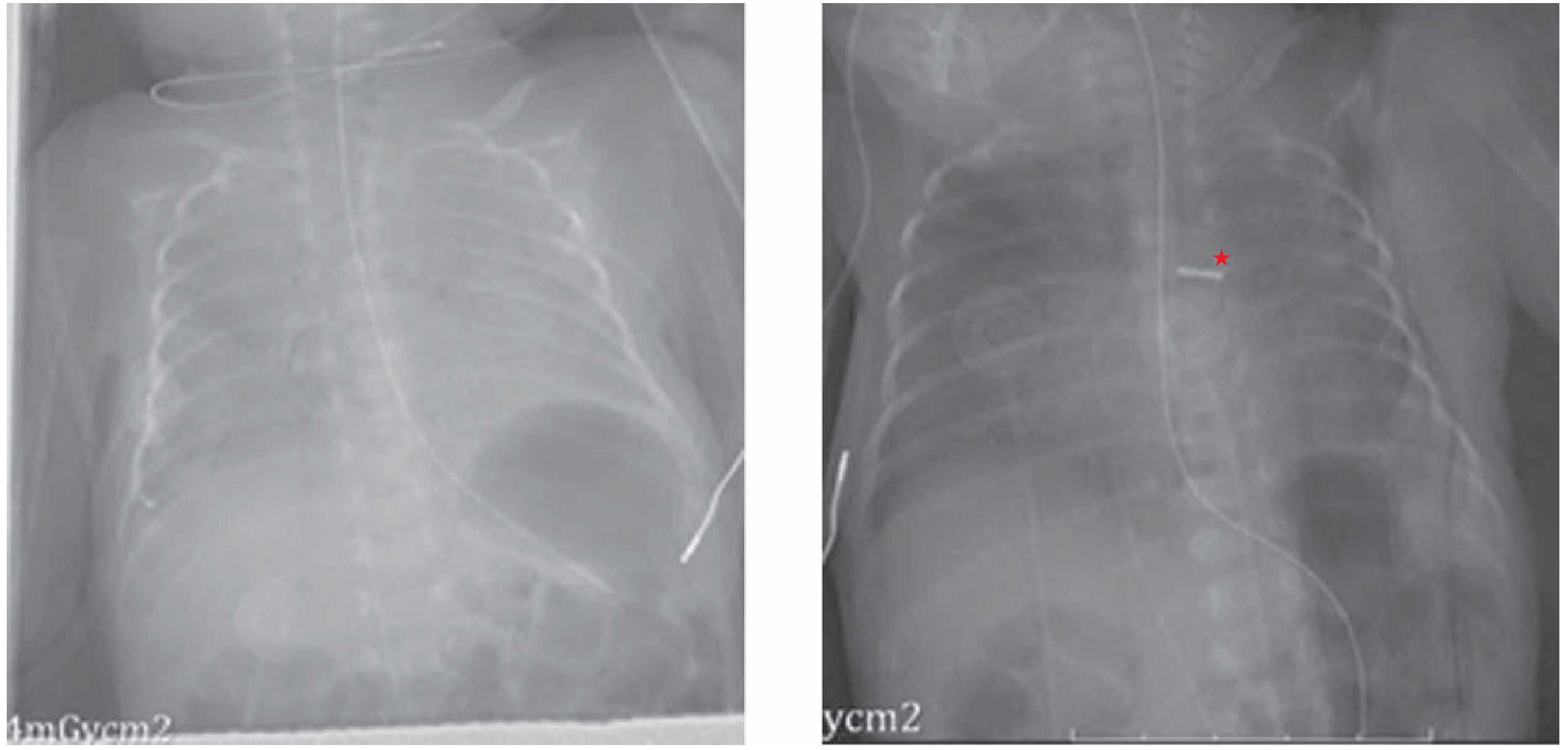
Left: Pre-ligation with increased pulmonary vascularity. Right: Post-ligation showing the surgical clip (★) and clearing of lung fields.
Treatment
The presence of a persistent PDA is sufficient indication for closure due to increased mortality and endocarditis risk (except in Eisenmenger physiology where closure does not help and carries higher mortality).
1. Pharmacological (Premature infants)
- Indomethacin or Ibuprofen (COX inhibitors → decrease PGE2 → promote ductal constriction)
- Indicated in premature infants
- Contraindications: necrotizing enterocolitis, renal insufficiency
- Term infants are generally unresponsive to pharmacological therapy
2. Catheter-Based (Transcatheter) Closure
- Devices: Rashkind double-umbrella, Gianturco coils, or Amplatzer-type occluders
- Widely used; suitable for older patients (>5 years) and smaller ducts (<3 mm)
- Complications: thromboembolism, incomplete occlusion, vascular injury, endocarditis, hemorrhage
- May not be applicable in very young/small infants (inadequate vascular access)
3. Surgical Closure
Approaches:
- Muscle-sparing posterolateral thoracotomy (3rd or 4th intercostal space, left side) - standard approach
- Median sternotomy - if additional cardiac lesions require simultaneous repair
- Video-assisted thoracoscopic (VATS) clipping - also described
Techniques:
- Simple ligation with surgical clip or permanent suture (neonates)
- Division between vascular clamps with oversewing of both ends (for short, broad ductus)
- CPB may be needed in extreme cases
- Recurrent laryngeal nerve must be carefully protected - it courses around the PDA
Preterm newborns and children do well with surgery; older patients and those with ducts <3 mm generally do well with coil occlusion.
Natural History & Prognosis
- Estimated 30% death rate for untreated isolated PDA
- Leading cause of death: congestive heart failure; secondary cause: respiratory infection
- Small PDA: risk of infectious endarteritis ~0.45%/year after the 2nd decade
- Large PDA: mortality rises to 3-4%/year by the 4th decade
- Two-thirds of patients die by age 60 if untreated with a moderate-large duct
Summary Table
| Feature | Detail |
|---|---|
| Origin | Left 6th aortic arch |
| Connects | Left pulmonary artery → descending aorta (distal to left subclavian) |
| Incidence | 1/2000 births; 7% of all CHD |
| Sex | Female > Male (2:1) |
| Shunt direction | Left-to-right (aorta → pulmonary artery) |
| Key murmur | Continuous "machinery" murmur, left 1st-2nd ICS |
| Pharmacotherapy | Indomethacin/Ibuprofen (premature only) |
| Definitive treatment | Catheter-based closure or surgical ligation |
| Closure mechanism | Ligamentum arteriosum (fibrous remnant) |
Sources: Schwartz's Principles of Surgery (11th Ed.) | Goldman-Cecil Medicine | Robbins & Kumar Basic Pathology | The Developing Human - Clinically Oriented Embryology | Grainger & Allison's Diagnostic Radiology
For a neonatal presentation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
"patent ductus arteriosus"[MeSH Terms] AND "infant, premature"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive neonatal-specific data from multiple authoritative sources. Here is the focused neonatal presentation:
PDA - Neonatal Presentation
Why PDAs Are So Common in Neonates
The neonatal PDA is a fundamentally different clinical entity from PDA in older children or adults. The key driver is prematurity:
| Gestational Age | PDA Incidence |
|---|---|
| Term infants | 0.3-0.8% (1 in ~2000) |
| Premature infants (all) | >20% |
| ≤28 weeks, birth weight <1750 g | ~100% within first 24 hours |
| 28-30 weeks gestation | Up to 75% |
Why prematurity causes PDA: The ductal smooth muscle is immature, meaning it has impaired sensitivity to the rising oxygen tension that normally drives constriction. As the fetus approaches term, the ductus becomes progressively less sensitive to prostaglandins and more sensitive to oxygen. Preterm infants lack this maturation.
Additional neonatal-specific risk factors:
- Respiratory distress syndrome (RDS): Surfactant deficiency → hypoxia → PDA persists. Low oxygen tension is a potent vasodilator of ductal smooth muscle.
- Maternal rubella infection (teratogenic damage to ductal tissue)
- High altitude births (chronic hypoxia)
- Indomethacin used as tocolytic in preterm labor - can cause paradoxical premature ductal constriction in utero, complicating postnatal physiology
Normal ductal closure in a healthy term neonate: functional closure within 10-15 hours, complete anatomic obliteration within weeks.
- Mulholland and Greenfield's Surgery, 7e | The Developing Human - Clinically Oriented Embryology
Definition in the Neonate (Harriet Lane)
Failure of the ductus arteriosus to close within the first 72 hours of life, or reopening after functional closure.
Neonatal Pathophysiology
At birth, pulmonary vascular resistance (PVR) drops dramatically and continues to fall over the first weeks. This means:
- Any ductal patency → left-to-right shunt (aorta → pulmonary artery)
- The shunt increases as PVR falls over weeks
- If PVR remains high (as in severe RDS or persistent pulmonary hypertension), shunting may be right-to-left → causing hypoxemia
Consequence of a significant L→R shunt in a neonate:
- Pulmonary overcirculation → pulmonary edema, impaired gas exchange, worsening respiratory failure
- Left heart volume overload → LV dilation, CHF
- Systemic steal ("ductal steal") → decreased diastolic perfusion of vital organs - brain, gut, kidneys
- Worsens and prolongs the need for mechanical ventilation
Clinical Presentation in the Neonate
Symptoms
| Finding | Mechanism |
|---|---|
| Tachypnea, respiratory distress | Pulmonary overcirculation + edema |
| Poor feeding, fatigue | Reduced cardiac output |
| Failure to thrive | Increased metabolic demand, poor feeding |
| Difficulty weaning from ventilator | PDA worsens lung disease of prematurity |
| Apnea | Seen with significant shunting in premature neonates |
Signs on Examination
| Sign | Detail |
|---|---|
| Murmur | Initially systolic; may become continuous ("machinery") with L→R flow - heard best at left upper sternal border / left infraclavicular area |
| Bounding/palmar pulses | Wide pulse pressure from diastolic runoff |
| Hyperactive precordium | Volume overload of LV |
| Widened pulse pressure | Diastolic BP falls as blood is shunted into pulmonary circulation |
| Tachycardia | Sympathetic activation |
Important: In premature neonates with high PVR (e.g., severe RDS), the murmur may be absent or only systolic early on - clinical suspicion must remain high even without a classical murmur.
Investigations
| Test | Neonatal Findings |
|---|---|
| Echocardiogram (Echo) | Gold standard - directly visualizes the ductus, color Doppler confirms L→R flow, assesses shunt size, LV dimensions, pulmonary pressure |
| CXR | Cardiomegaly, increased pulmonary vascular markings (may be hard to distinguish from RDS infiltrates in preterm lungs) |
| ECG | Normal to moderate LVH in small-moderate PDA; biventricular hypertrophy in large PDA |
| SpO2 monitoring | If right-to-left shunting: lower saturation in lower extremities vs. right hand (pre-ductal) |
Echocardiogram of PDA - color Doppler confirms flow from aorta (AO) into pulmonary artery (PA):

Treatment in the Neonate
Key principle: In premature neonates, pharmacological therapy works. In term neonates, it generally does not (ductal smooth muscle is already mature and unresponsive to PG inhibition).
Step 1 - Conservative / Watchful Waiting
- Fluid restriction, diuretics
- Some PDAs in premature infants close spontaneously - indications for treatment and timing remain controversial
- Harriet Lane Handbook, 23rd Ed.
Step 2 - Pharmacological Closure (Premature infants only)
| Drug | Mechanism | Notes |
|---|---|---|
| Ibuprofen | COX inhibitor → ↓ PGE2 → ductal constriction | Drug of choice - fewer renal side effects than indomethacin, no increased NEC risk |
| Indomethacin | COX inhibitor | Effective but more side effects (renal, GI perforations) |
| Acetaminophen | Emerging alternative (inhibits prostaglandin peroxidase) | Similar efficacy to oral ibuprofen; fewer effects on kidneys and platelets; evidence still evolving |
Efficacy: Pharmacologic closure is effective in ~65% of premature infants
Contraindications to NSAIDs (indomethacin/ibuprofen):
- Necrotizing enterocolitis (NEC)
- Renal insufficiency / oliguria
- Intracranial hemorrhage
- Bleeding disorders / thrombocytopenia
- Sepsis
Complications of NSAIDs in neonates:
- Renal: Transient ↓ GFR, oliguria
- GI: Transient GI bleeding; spontaneous intestinal perforations (SIPs) with indomethacin (worse with concomitant hydrocortisone)
- Haematological: Prolonged bleeding time, impaired platelet function for 7-9 days (not dose-related)
After 3 complete courses of ibuprofen without closure → refer for endovascular or surgical closure.
Step 3 - Transcatheter (Endovascular) Closure
- Amplatzer Piccolo Occluder (Abbott): FDA-approved for infants <2 kg
- Procedural mortality: ~3%
- Complete ductal closure: >90%
- Other devices: Rashkind double-umbrella, Gianturco coils
- Now the treatment of choice for most PDAs
Step 4 - Surgical Ligation
Approach in premature neonates:
- Left posterolateral thoracotomy via 3rd intercostal space
- Single surgical clip applied to the ductus (ductal tissue is extremely friable in premature infants - direct manipulation is minimized)
- Commonly performed at the bedside in the NICU to avoid the hazards of patient transfer
Surgical complications to watch for:
- Recurrent laryngeal nerve injury (nerve loops around the ductus)
- Phrenic nerve injury
- Pneumothorax
- Chylothorax (thoracic duct injury)
Note: The ductus may be the largest vascular structure visible in a premature infant - it must not be confused with the aorta.
Surgical closure is now reserved for large-diameter or very short PDAs not amenable to device closure. Periprocedural mortality approaches zero in modern centres.
- Mulholland and Greenfield's Surgery, 7e | Harriet Lane Handbook, 23rd Ed. (Johns Hopkins)
Special Scenario - PDA as a Life-Saving Connection
In certain complex CHDs, ductal patency is essential to maintain perfusion until definitive repair:
| Defect | Role of PDA |
|---|---|
| Pulmonary atresia / critical PS | PDA provides the only source of pulmonary blood flow |
| Severe coarctation / interrupted aortic arch | PDA provides systemic perfusion to the lower body |
| Hypoplastic left heart syndrome (HLHS) | PDA essential for systemic output |
Treatment: IV Prostaglandin E1 (alprostadil/PGE1) is infused to maintain/reopen the ductus in these duct-dependent lesions until surgical palliation (e.g., Norwood procedure) or balloon intervention.
Neonatal PDA - Management Summary
Premature neonate with suspected PDA
↓
Echo confirmation
↓
Haemodynamically significant?
YES NO
↓ ↓
Check contraindications Watchful waiting
to NSAIDs
↓
Ibuprofen (drug of choice) x 3 courses
OR Indomethacin / Acetaminophen
↓
Closed (~65%)? Still open?
↓ ↓
Monitor Transcatheter closure
(Piccolo Occluder if <2kg)
↓
Still open / not suitable?
↓
Surgical ligation (NICU bedside)
Sources: Mulholland and Greenfield's Surgery (7e) | Harriet Lane Handbook (23rd Ed., Johns Hopkins) | Schwartz's Principles of Surgery (11th Ed.) | The Developing Human - Clinically Oriented Embryology
This is a shared conversation. Sign in to Orris to start your own chat.