Prepare ischiorectul fossa for RUHS MBBS exam of anatomy with book reference Vishram Singh with colorful diagram.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Generating Image
Now I have all the material needed. Let me compile the complete, exam-focused notes.
Ischiorectal (Ischioanal) Fossa - RUHS MBBS Anatomy
Reference: Vishram Singh - Textbook of Anatomy (Abdomen & Lower Limb, Vol. 2); supplemented by Thieme Atlas of Anatomy & Color Atlas of Human Anatomy (Sobotta)
Generated Diagram
Anatomical Images from Textbook
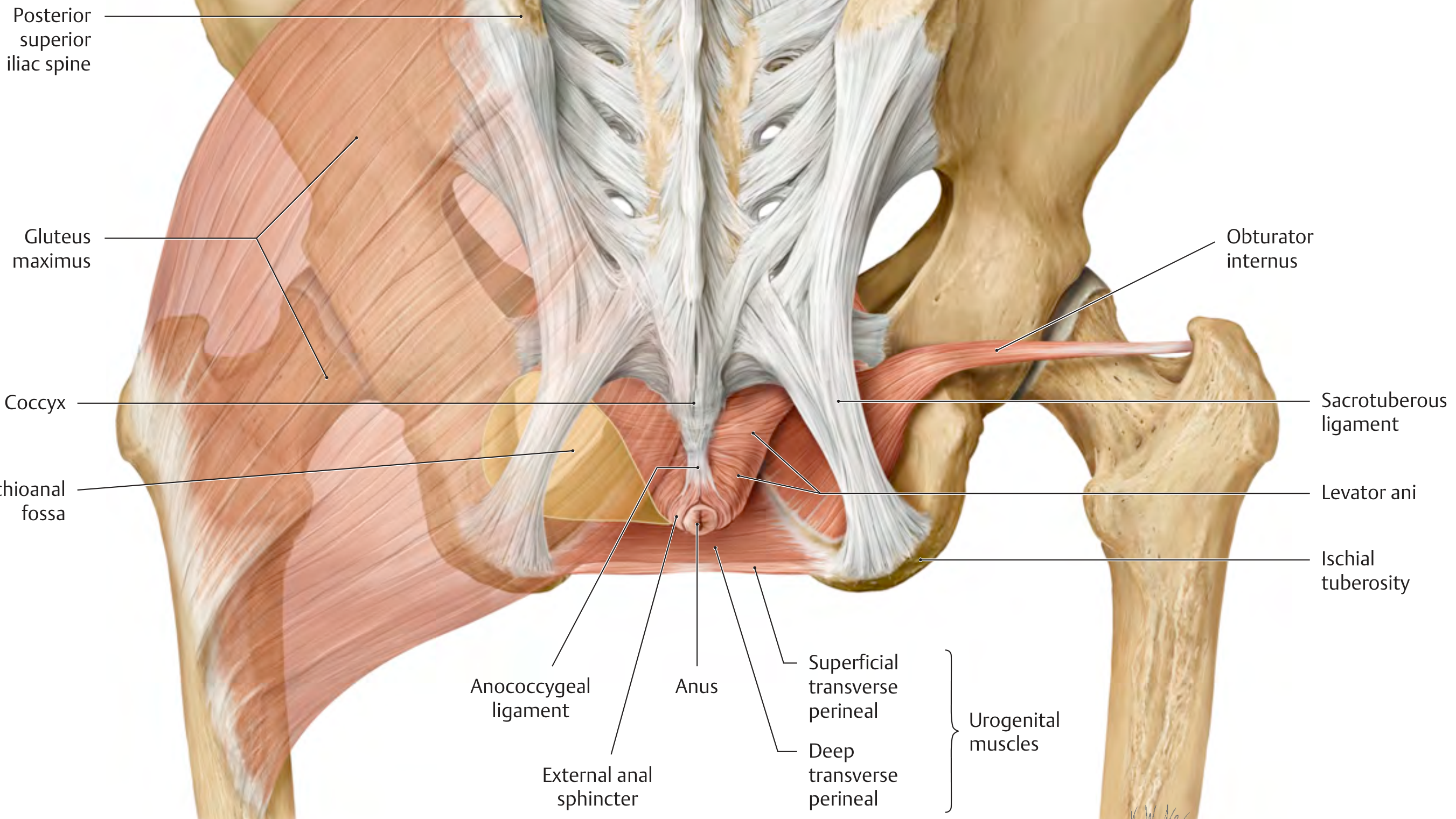
Posterior view - Muscular boundaries:
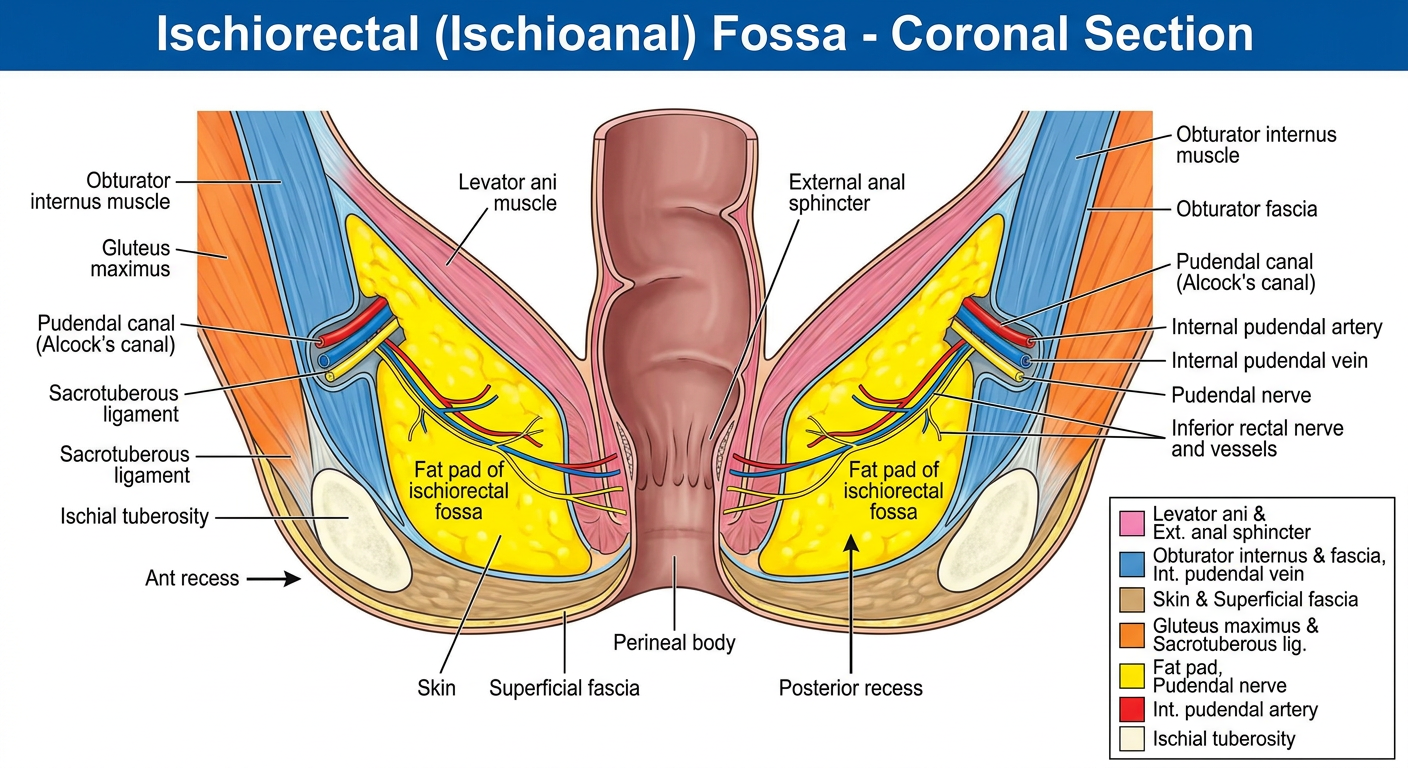
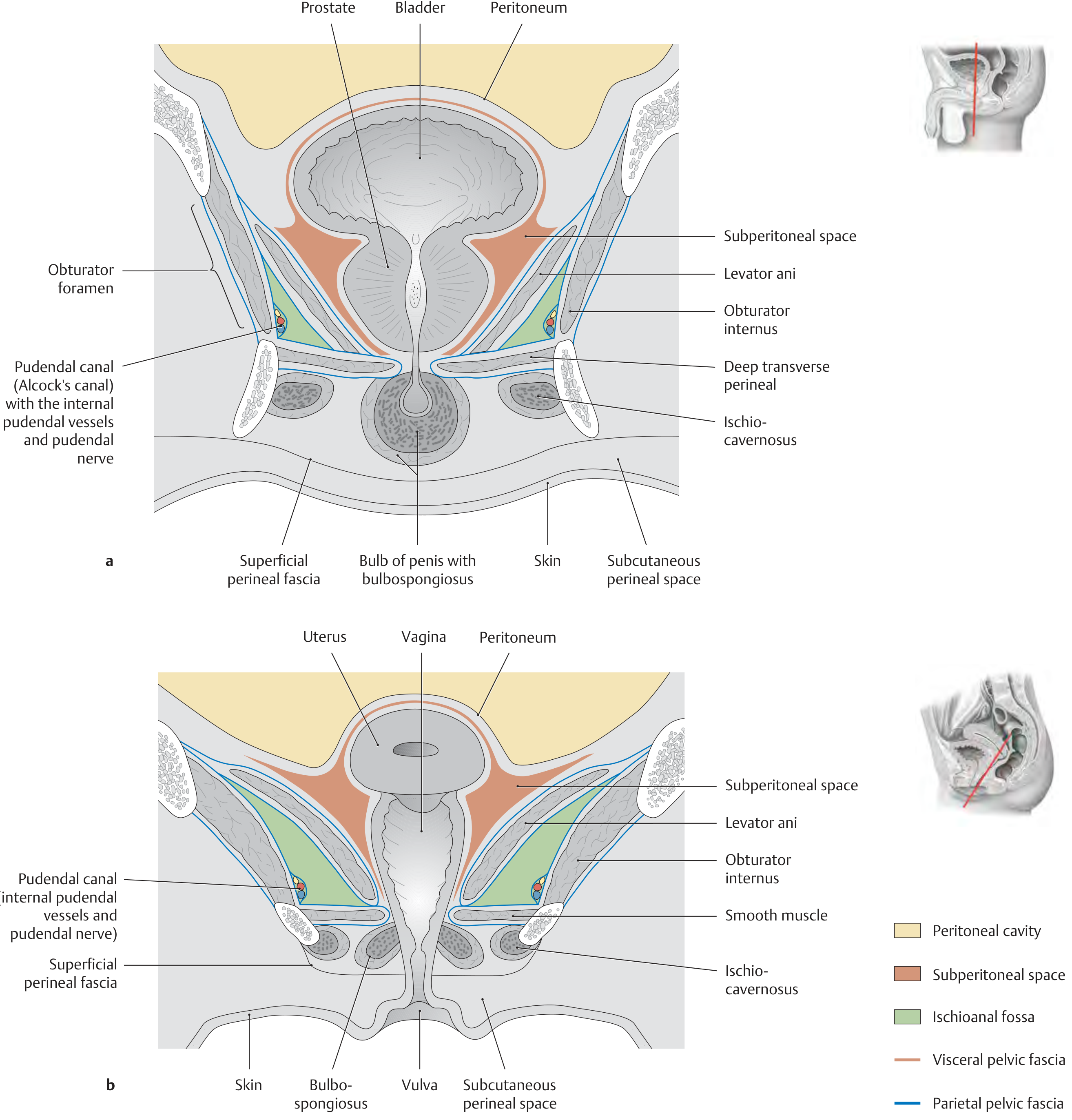
Coronal section - Male and Female pelvis:
1. Introduction
The ischiorectal fossa (now officially called the ischioanal fossa) is a wedge/pyramid-shaped space filled with fatty tissue, located on each side of the anal canal, outside the pelvic floor.
- It is one of the paired bilateral spaces of the perineum
- It communicates across the midline via the posterior recess (behind the anal canal), forming a potential "horseshoe" space
- The fat pad filling the fossa acts as a mobile cushion that slides during defecation and parturition
2. Shape
The fossa is pyramidal with:
| Feature | Detail |
|---|---|
| Apex | Upward - at the junction of levator ani and obturator internus |
| Base | Downward - perineal skin (floor) |
| Tip | Points anteriorly toward the pubic symphysis |
| Posterior opening | Wide - faces the gluteal region |
3. Boundaries (RUHS Exam Favourite!)
| Wall | Boundary |
|---|---|
| Medial wall | Levator ani muscle + its inferior fascia (pelvic diaphragm) + external anal sphincter |
| Lateral wall | Obturator internus muscle covered by obturator fascia (contains pudendal canal!) |
| Floor / Base | Perineal skin + superficial perineal fascia |
| Apex | Meets at the union of levator ani and obturator internus (fascia splits here) |
| Posterior boundary | Gluteus maximus muscle + sacrotuberous ligament |
| Anterior boundary | Posterior border of the urogenital diaphragm (deep perineal pouch) |
Lateral wall bony landmark: Ischial tuberosity is on the lateral wall
4. Contents
A. Fat Body of the Ischioanal Fossa
- Fills the entire fossa
- Function: mobile, compressible pad allowing distension of anal canal during defecation
- Can be removed surgically without major consequence (important in abscess drainage)
B. Inferior Rectal (Hemorrhoidal) Vessels & Nerve
- Branch from the internal pudendal vessels and pudendal nerve (S2, S3, S4)
- Cross the fossa medially from the lateral wall
- Supply the external anal sphincter and perianal skin
C. Perineal Branch of S4 (Cutaneous)
- Runs across the fossa to supply the perineum
D. Scrotal/Labial Posterior Branches
- Posterior scrotal / posterior labial nerves and vessels cross the anterior part of the fossa
5. Pudendal Canal (Alcock's Canal) - HIGH YIELD
- A fascial sheath on the lateral wall of the fossa (within the obturator fascia)
- Contains:
- Internal pudendal artery
- Internal pudendal vein
- Pudendal nerve (S2, S3, S4)
- Structures enter the canal by passing around the ischial spine and sacrospinous ligament
- Clinically important for pudendal nerve block in obstetrics
6. Recesses of the Fossa
| Recess | Location | Significance |
|---|---|---|
| Anterior recess | Extends forward above urogenital diaphragm (between levator ani and obturator internus) | Can be site of abscess extension |
| Posterior recess | Extends behind anal canal, between gluteus maximus and external sphincter | Bilateral fossae communicate here → horseshoe abscess |
7. Communications
- The two fossae communicate posteriorly behind the anal canal
- This explains the horseshoe abscess - infection can spread from one side to the other without crossing the anal canal
8. Nerve Supply Summary
| Nerve | Origin | Area Supplied |
|---|---|---|
| Inferior rectal nerve | Pudendal nerve (S2,S3,S4) | External anal sphincter, perianal skin |
| Perineal branch of S4 | S4 nerve root | Skin of perineum |
| Perineal nerve | Pudendal nerve | Scrotum/labia, perineal muscles |
9. Blood Supply
- Arterial: Inferior rectal artery (branch of internal pudendal artery) - main supply to the fossa contents
- Venous: Inferior rectal vein -> internal pudendal vein -> internal iliac vein
10. Clinical Correlates (RUHS Exam!)
A. Ischiorectal Abscess
- Most common abscess of the perineum
- Arises from infected anal glands (cryptoglandular origin)
- Presents as: severe throbbing pain, tender swelling lateral to anus, fever
- Because the two fossae communicate posteriorly, can form a horseshoe abscess spreading to both sides
- Treatment: incision and drainage through perineal skin
B. Pudendal Nerve Block
- Needle passed through the lateral wall of the fossa to reach the pudendal canal
- Used in obstetric analgesia and anorectal surgery
- Landmark: ischial spine (felt transvaginally)
C. Spread of Perineal Infections
- Infections in the fossa can track:
- Anteriorly into the anterior recess above urogenital diaphragm
- Posteriorly to communicate with the opposite fossa
- Superiorly into supralevator space (supraelevator abscess)
D. Relevance in Episiotomy and Perineal Tears
- The fat pad absorbs forces during delivery
- Deep tears can violate the fossa boundaries
11. Quick Memory Table - RUHS Format
| Feature | Key Point |
|---|---|
| Shape | Pyramid / wedge |
| Medial wall | Levator ani + external anal sphincter |
| Lateral wall | Obturator internus + pudendal canal |
| Floor | Perineal skin |
| Contents | Fat, inferior rectal NVB, S4 branch |
| Special structure in lateral wall | Alcock's canal (pudendal nerve, internal pudendal A & V) |
| Posterior communication | Horseshoe abscess pathophysiology |
| Clinical importance | Ischiorectal abscess, pudendal nerve block |
12. Vishram Singh Key Points (Vol. 2 Pelvis & Perineum)
In Vishram Singh Textbook of Anatomy - Abdomen & Lower Limb (Vol. 2), the ischiorectal fossa is covered under the Perineum chapter with these high-yield points:
- Described as a "pair of wedge-shaped spaces" filled with fatty areolar tissue
- Boundaries taught with a "MILD GAS" mnemonic (Medially: levator ani; Inferiorly: skin; Laterally: obturator internus with obturator fascia; Dorsal/Posterior: gluteus maximus and sacrotuberous ligament)
- The anterior recess extends forward above the posterior border of the perineal membrane (urogenital diaphragm)
- Emphasized clinically for ischiorectal abscess and pudendal nerve block
- The pudendal canal (Alcock's canal) in the lateral wall is a consistent exam question
Source references:
- Vishram Singh, Textbook of Anatomy Abdomen & Lower Limb, Vol. 2 - Chapter on Perineum (Ischiorectal Fossa)
- Thieme Atlas of Anatomy: General Anatomy and Musculoskeletal System, Section 5.7 - The Ischioanal Fossa, p. 581-582
- Color Atlas of Human Anatomy Vol. 2, Internal Organs - Section 7.12, Ischioanal Fossa, p. 476-477
This is a shared conversation. Sign in to Orris to start your own chat.