Elbow joint approaches ms ortho 20 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the information needed from Campbell's Operative Orthopaedics 15th Ed to write a comprehensive 20-mark MS Ortho answer on elbow joint approaches.
Surgical Approaches to the Elbow Joint
Source: Campbell's Operative Orthopaedics, 15th Ed. 2026
INTRODUCTION
The elbow is a complex joint comprised of three articulations: the ulnohumeral (hinge), radiocapitellar (pivot), and proximal radioulnar joints. Surgical approaches must account for three major nerves at risk - the ulnar nerve (medial), the radial nerve and its posterior interosseous branch (lateral), and the median nerve (anterior). Selection of approach depends on the pathology, extent of exposure required, and the need for ligament/tendon preservation.
The main approaches are classified as:
- Posterior approaches
- Lateral approaches
- Medial approach
- Combined (Global) approach
- Anterior approach
I. POSTERIOR APPROACHES
A. Campbell's Posterolateral Approach (Technique 1.107)
Indications: Old posterior dislocations, fractures of distal humerus involving the joint, arthroplasties.
Position: Prone or lateral.
Incision: Begins 10 cm proximal to the elbow on the posterolateral aspect, continues distally for 13 cm.
Steps:
- Deepen dissection through fascia, expose the triceps aponeurosis down to its olecranon insertion.
- Free the aponeurosis in a tongue-shaped flap, reflecting it distally; incise remaining muscle fibers to bone in the midline.
- Subperiosteal dissection exposes the joint. The ulnar nerve is identified and protected throughout.
Key structures at risk: Ulnar nerve (identified and protected in its groove).
B. Extensile Posterolateral Approach - Wadsworth (Technique 1.108)
Indications: Wide exposure of posterior elbow and proximal radioulnar joint.
Position: Prone, elbow flexed 90 degrees, forearm dependent.
Incision: Curved, from posterior surface of arm at proximal limit of triceps tendon, distally to the posterior aspect of the lateral epicondyle, then 4 cm distal to olecranon tip.
Steps:
- Reflect skin flaps; isolate ulnar nerve proximally, release arcuate ligament, retract with rubber sling.
- Fashion a distally based tongue of triceps tendon (leaving peripheral tendinous rim for repair), separating anconeus from extensor carpi ulnaris.
- Reflect the triceps flap distally, divide posterior capsule.
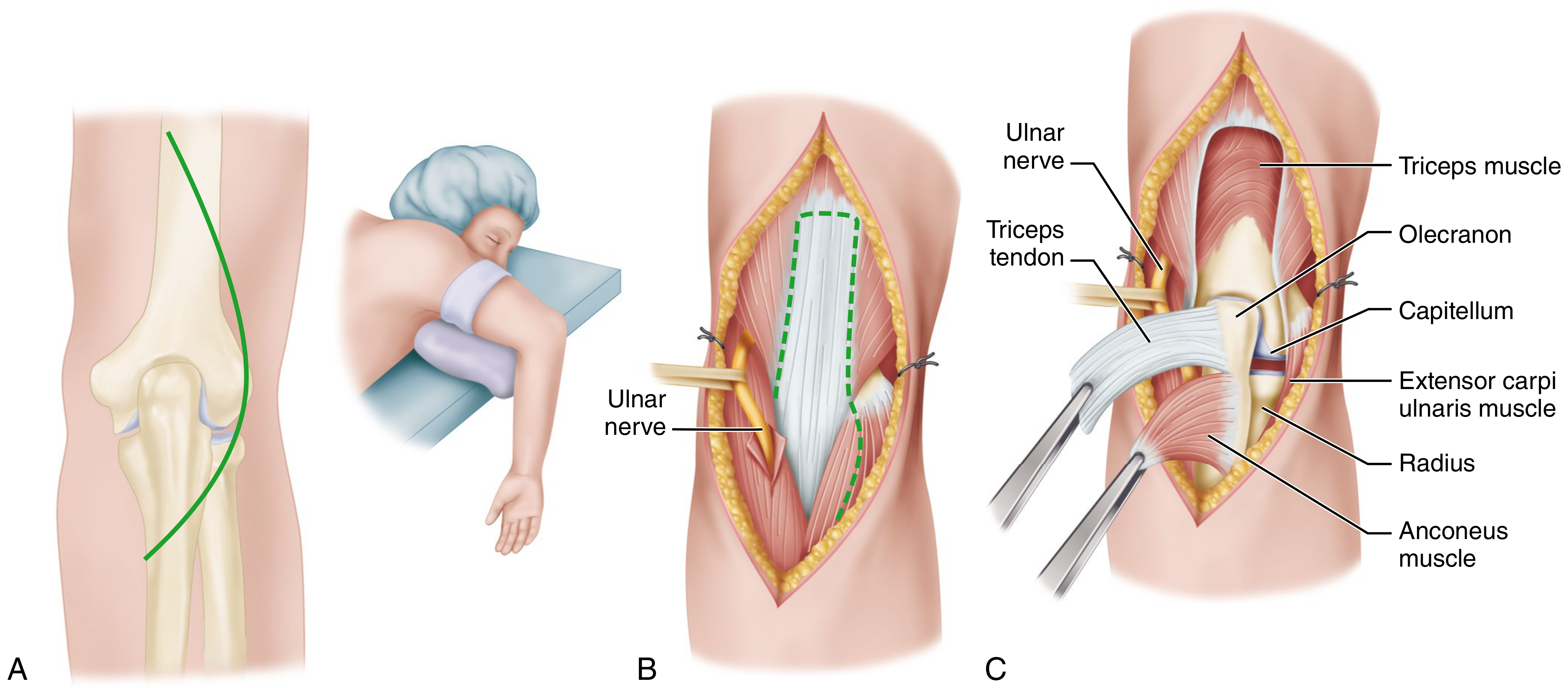
Figure: Wadsworth extensile posterolateral approach - note distally-based triceps tongue and protected ulnar nerve
C. Posterior Approach by Olecranon Osteotomy - MacAusland and Muller (Technique 1.109)
Indications: Fractures of distal humerus (most extensile posterior approach; provides the maximum articular surface exposure).
Key anatomical point: Wilkinson and Stanley showed that olecranon osteotomy exposes significantly more articular surface of the distal humerus than a triceps-reflecting approach.
Steps:
- Straight posterior incision - 5 cm distal to olecranon tip, proximally medial to midline for 10-12 cm above olecranon.
- Isolate ulnar nerve; retract with Penrose drain.
- Pre-drill fixation hole (6.5 mm cancellous screw) before osteotomy.
- Identify the bare zone of the olecranon. Mark a chevron osteotomy (~60 degrees, apex distal) at this bare zone.
- Divide 3/4 of olecranon depth with thin oscillating saw; fracture the last 1/4 with an osteotome (to avoid cutting through articular surface).
- Reflect olecranon with attached triceps proximally - excellent exposure of posterior distal humerus achieved.
- Closure: Reduce and fix with lag screw + tension band wire.
D. Bryan and Morrey Extensile Posterior Approach (Technique 1.110)
Indications: Total elbow arthroplasty - preserves continuity of triceps mechanism, allowing easy repair and rapid rehabilitation.
Position: Lateral decubitus (or 45-60 degrees tilted), limb across chest.
Incision: Straight posterior midline, from 7 cm distal to olecranon tip to 9 cm proximal.
Steps:
- Identify ulnar nerve at medial border of medial triceps head; dissect free to first motor branch. In TJA, transpose anteriorly into subcutaneous tissue.
- Elevate medial aspect of triceps from humerus along intermuscular septum to the posterior capsule.
- Incise superficial forearm fascia distally ~6 cm to periosteum of medial olecranon.
- Reflect periosteum and fascia as a single unit medially to laterally. The medial junction between triceps insertion and forearm fascia/ulnar periosteum is the weakest point - careful sharp dissection with elbow extended 20-30 degrees.
- To expose the radial head, reflect anconeus subperiosteally from proximal ulna - entire joint is now widely exposed.
- Closure: Return triceps to anatomic position; suture through drill holes in proximal ulna. Suture periosteum to superficial forearm fascia.
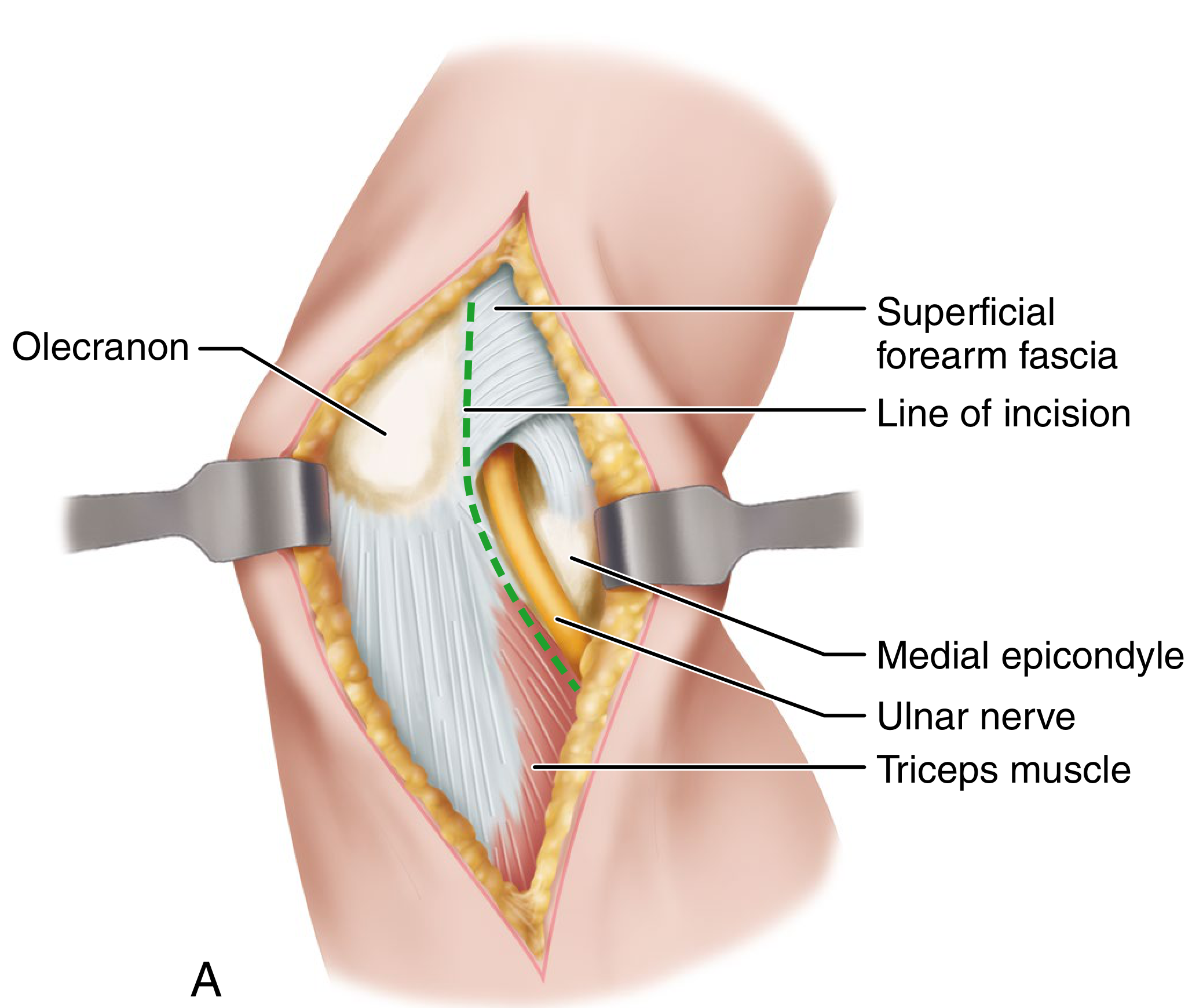
Figure: Bryan-Morrey approach - ulnar nerve dissected and medial fascia/periosteal reflection
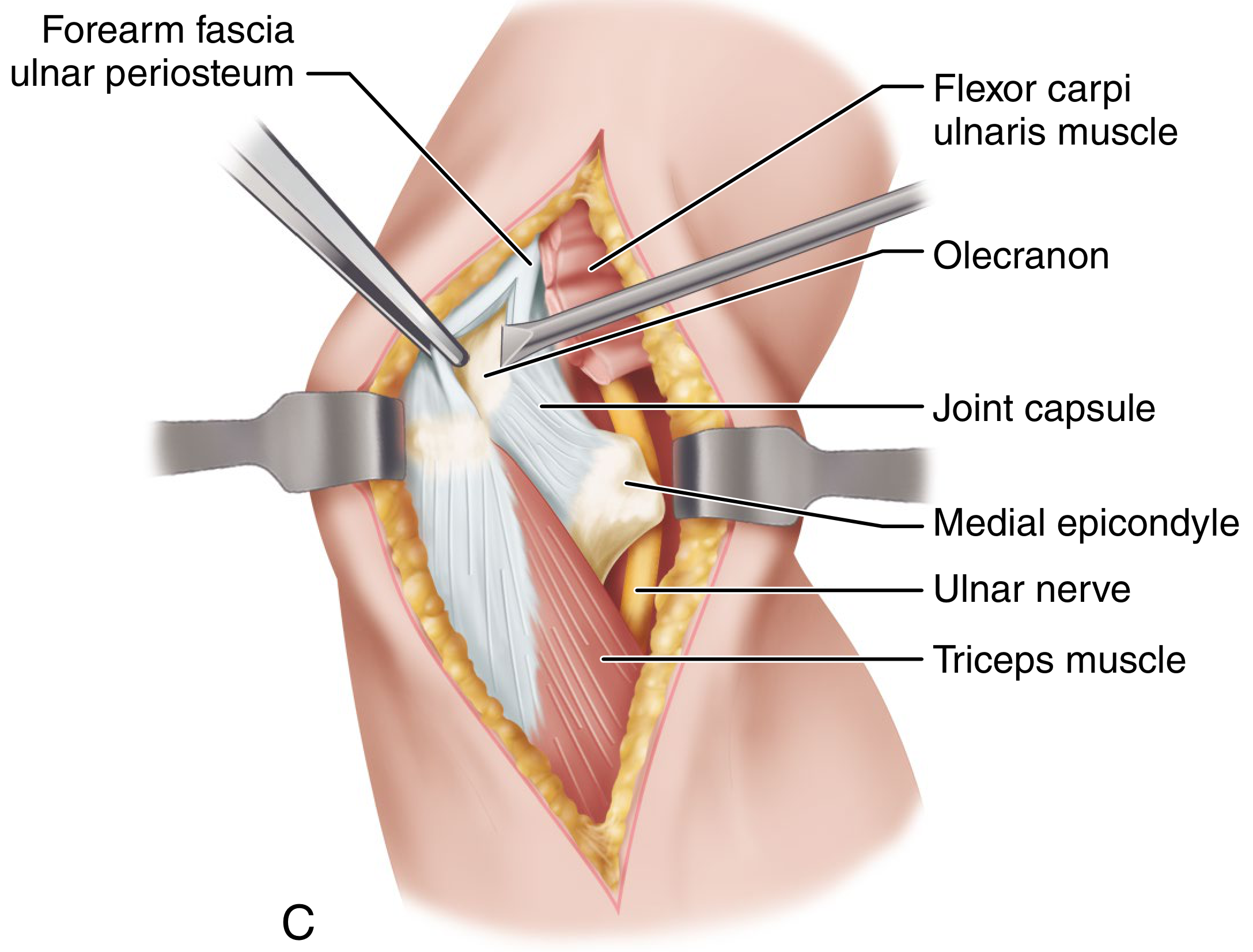
Figure: Bryan-Morrey approach - complete exposure with the triceps mechanism reflected as a single unit
II. LATERAL APPROACHES
A. Kaplan Lateral Approach (Technique 1.111)
Indications: Fracture of lateral condyle - the common extensor origin remains attached to the condylar fragment and need not be disturbed. Also used for radial head excision, capitellum fractures.
Interval: Between triceps (posterior) and extensor carpi radialis longus/brachioradialis (anterior).
Incision: ~5 cm proximal to lateral epicondyle, distally along lateral epicondyle, then ~5 cm onto anterolateral forearm.
Steps:
- Develop the interval between triceps posteriorly and ECRL/brachioradialis anteriorly to expose the lateral border of the humerus.
- Important: In the proximal angle, avoid the radial nerve which passes between brachioradialis and brachialis.
- Continue distally onto the condyle and proximal forearm.
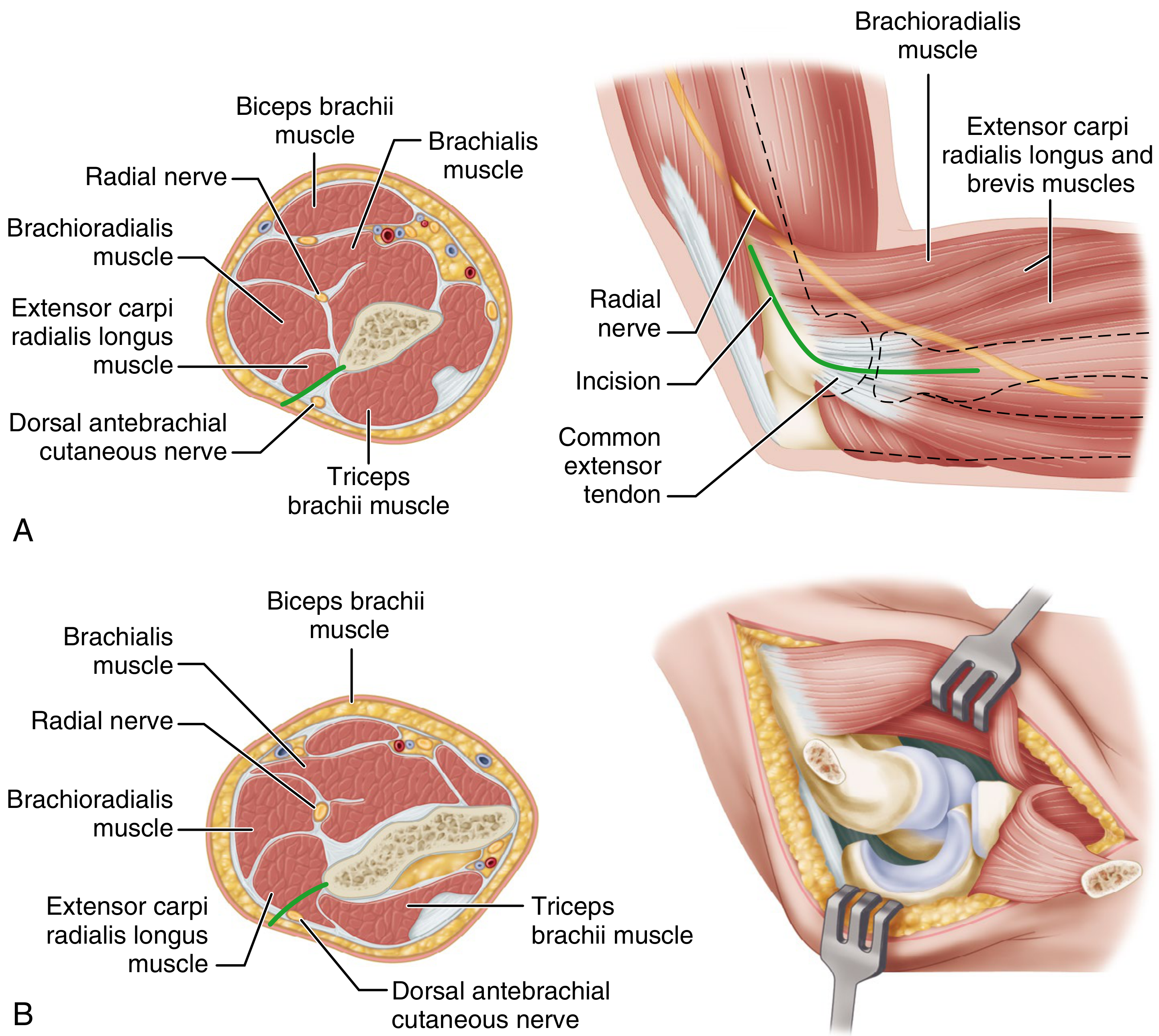
Figure: Kaplan lateral approach - cross-sections showing plane and radial nerve relation
B. Kocher Lateral "J" Approach (Technique 1.112)
Indications: Exposure of lateral condyle, radial head, and lateral structures. Used for lateral ligament repair, radial head fractures.
Internervous interval: Between anconeus (radial nerve) and extensor carpi ulnaris (posterior interosseous nerve - a branch of the radial nerve). This is the Kocher interval.
Incision: "J"-shaped - begins 5 cm proximal to elbow over lateral supracondylar ridge, extends distally to radial head and curves medially and posteriorly to posterior border of ulna.
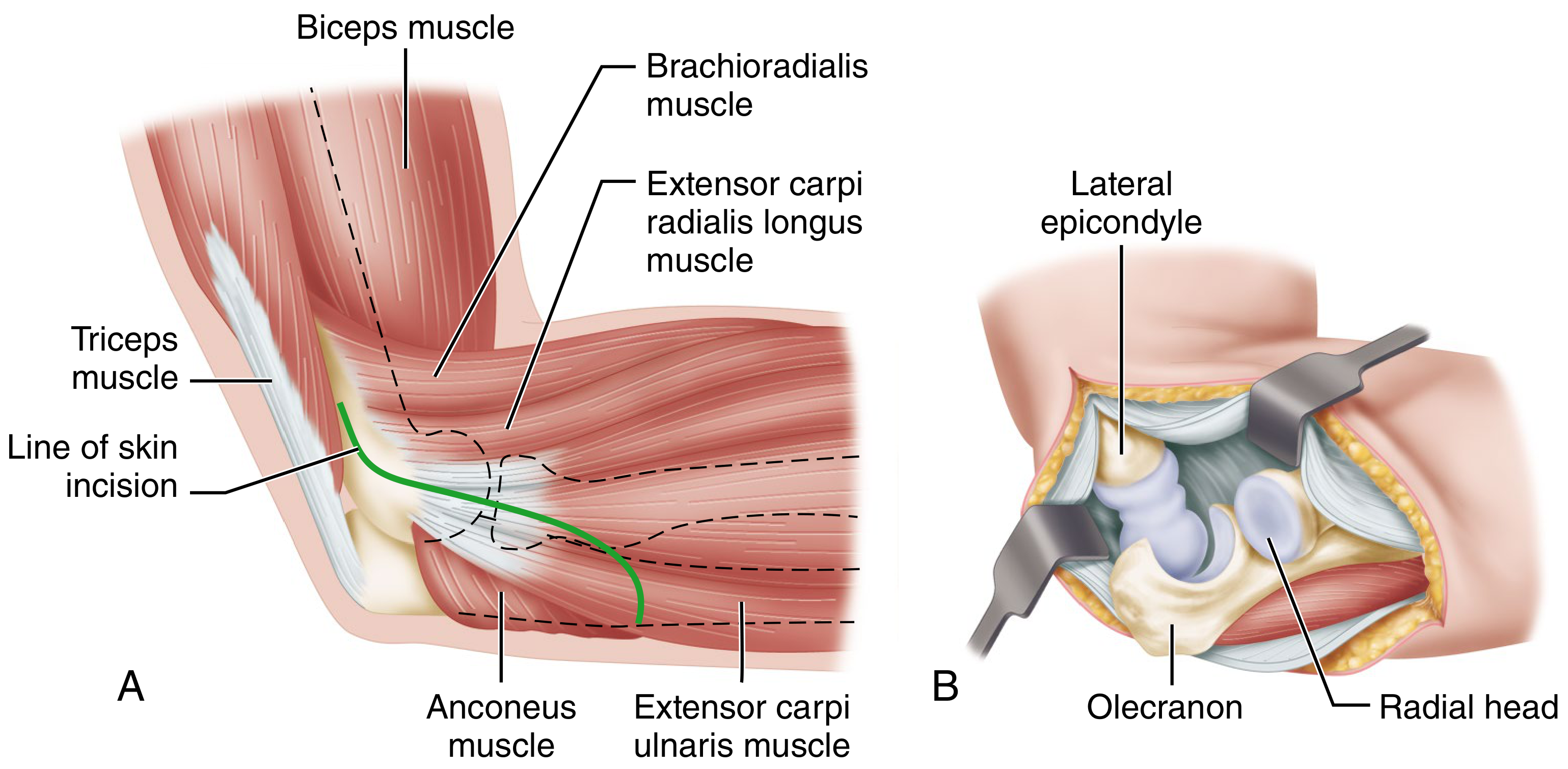
Figure: Kocher lateral J approach - skin incision (A) and completed exposure with joint dislocated (B)
Key point: The Kocher approach uses the safest internervous interval for the lateral elbow, as both anconeus and ECU are supplied by the radial nerve and its branches - there is no true internervous plane, but injury risk is minimized. The posterior interosseous nerve is at risk distally.
III. MEDIAL APPROACH
Campbell's Medial Approach with Osteotomy of the Medial Epicondyle - Molesworth and Campbell (Technique 1.113)
Indications: Incarcerated medial epicondyle fragment, medial collateral ligament reconstruction, exposure of medial joint.
Incision: Medial, over the tip of the medial epicondyle, from 5 cm distal to 5 cm proximal to the joint.
Steps:
- Isolate ulnar nerve in its groove posterior to the epicondyle; free it and retract posteriorly.
- Dissect all soft tissues from epicondyle except the common flexor origin; detach the epicondyle with an osteotome and reflect it distally with its attached flexor muscles.
- Protect branches of median nerve supplying these muscles (entering along lateral margins).
- Free the medial coronoid process; incise capsule; strip periosteum and capsule anteriorly and posteriorly.
- Avoid injuring the median nerve passing anterior to the joint.
- Dislocate the joint with the lateral capsule acting as a hinge - all articular surfaces can now be inspected.
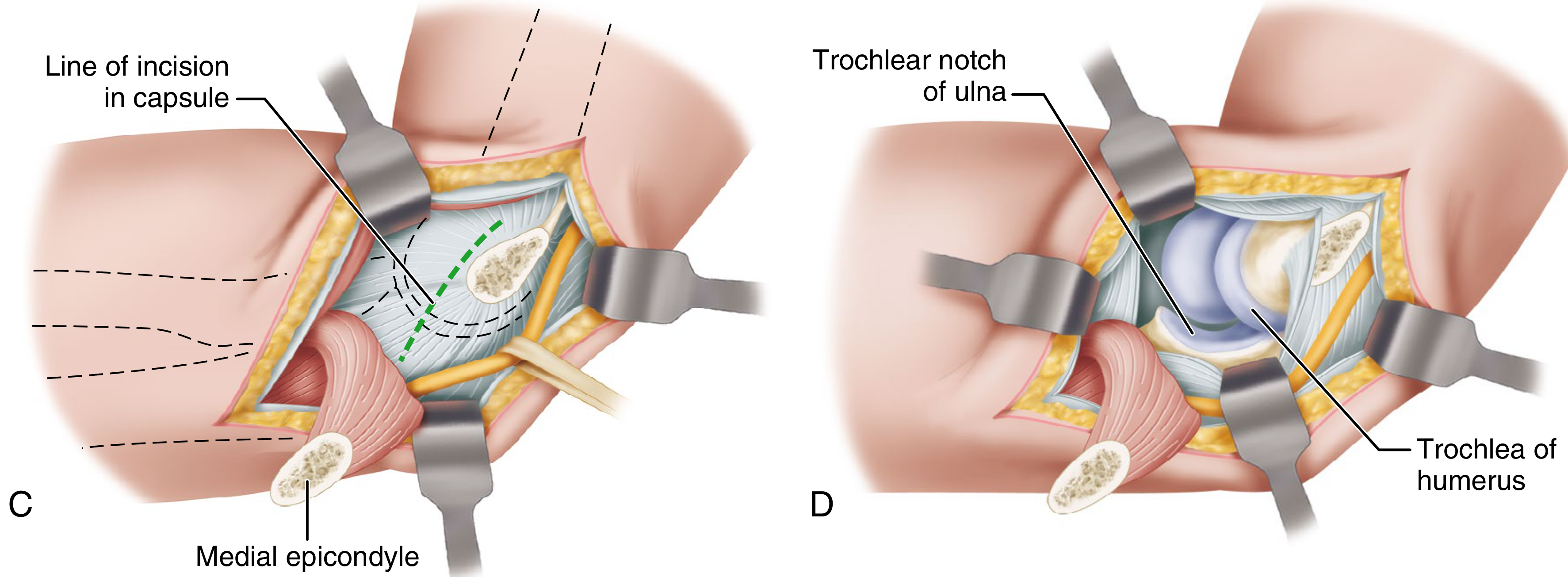
Figure: Medial approach showing capsule line of incision and full joint exposure with trochlea and trochlear notch of ulna visible after dislocation
IV. MEDIAL AND LATERAL (COMBINED) APPROACH (Technique 1.114)
Indications: When extensive exposure is not needed but bilateral access is required (e.g. simple contracture release, loose body removal).
Technique: Incisions of 5-7 cm made on either or both sides of the joint, just anterior to the condyles, parallel with the epicondylar ridges. Capsule is incised from proximal to distal on each side.
Note: On the medial side, carefully avoid the ulnar nerve.
V. GLOBAL APPROACH - Patterson, Bain and Mehta (Technique 1.115)
Indications: Circumferential exposure needed (complex fracture-dislocations, terrible triad injuries, access to coronoid process + anterior capsule + both collateral ligaments).
Incision: Straight posterior midline.
Steps:
- Dissect through deep fascia to triceps tendon and subcutaneous border of ulna.
- Isolate ulnar nerve, open cubital tunnel, transpose anteriorly (protected with Penrose drain throughout).
- Develop full-thickness medial or lateral fasciocutaneous flaps.
Posterolateral component:
- Develop Kocher interval (anconeus - ECU) to expose capsule and lateral epicondyle.
- Reflect anconeus and triceps medially for olecranon fossa exposure.
- Elevate common extensor origin anteriorly for radial head exposure.
- Arthrotomy along anterior border of lateral ulnar collateral ligament, dividing annular ligament.
- If more radial head exposure needed: chevron osteotomy of lateral epicondyle.
- Forearm pronated to translate the posterior interosseous nerve anteriorly and protect it.
Posteromedial component:
- Release flexor carpi ulnaris and flexor digitorum profundus subperiosteally from ulnar origins.
- Retract anteriorly to expose coronoid process, anterior bundle of medial ligament complex, and anterior joint capsule.
VI. ANTERIOR APPROACH
Indications: Anterior compartment loose bodies, anterior capsule release, biceps tendon reattachment, brachialis repairs.
Internervous plane: Between brachioradialis (radial nerve) and brachialis (musculocutaneous nerve).
Key structures at risk: Median nerve, brachial artery (immediately medial to biceps tendon).
SUMMARY TABLE
| Approach | Eponym | Key Interval / Technique | Structures at Risk | Main Indications |
|---|---|---|---|---|
| Posterolateral | Campbell | Triceps tongue flap | Ulnar nerve | Old dislocations, arthroplasty |
| Extensile posterolateral | Wadsworth | Distally-based triceps tongue | Ulnar nerve, PIN | Arthroplasty, complex fractures |
| Posterior (olecranon osteotomy) | MacAusland/Muller | Chevron osteotomy, bare zone | Ulnar nerve | Distal humerus fractures (best exposure) |
| Extensile posterior | Bryan-Morrey | Medial-to-lateral periosteal/fascial peel | Ulnar nerve | Total elbow arthroplasty |
| Lateral | Kaplan | Triceps / ECRL-brachioradialis | Radial nerve proximally | Lateral condyle fractures |
| Lateral J | Kocher | Anconeus / ECU (Kocher interval) | PIN distally | Radial head, lateral ligaments |
| Medial (epicondyle osteotomy) | Molesworth/Campbell | Osteotomy of medial epicondyle | Ulnar nerve, median nerve | Medial epicondyle, MCL |
| Medial + lateral | - | Bilateral limited | Ulnar nerve | Contracture release |
| Global | Patterson-Bain-Mehta | Combined posterior + Kocher + medial peel | Ulnar nerve, PIN | Terrible triad, complex instability |
| Anterior | - | Brachioradialis / brachialis | Median nerve, brachial artery | Anterior loose bodies, capsule release |
NERVE-AT-RISK SUMMARY
- Ulnar nerve: At risk in ALL posterior and medial approaches. Always identify proximally first, protect with Penrose drain or rubber sling. Transpose anteriorly in arthroplasty.
- Radial nerve (main trunk): At risk proximally in lateral (Kaplan) approach.
- Posterior interosseous nerve (PIN): At risk in Kocher approach distally and in the global approach. Forearm pronation displaces PIN anteriorly, away from the operative field - a key protective maneuver.
- Median nerve: At risk in medial and anterior approaches - it crosses anterior to the joint.
Source: Campbell's Operative Orthopaedics, 15th Ed. 2026 - Chapters on Elbow Approaches (Techniques 1.107-1.115)
Acid fast bacilli ms ortho 20 marks answer
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write a detailed 20-mark MS Ortho answer on Acid Fast Bacilli. Let me compile it.
Acid Fast Bacilli (AFB) - MS Ortho 20 Marks Answer
Sources: Harrison's Principles of Internal Medicine 22E (2025), Jawetz Medical Microbiology 28E, Murray & Nadel's Respiratory Medicine, Firestein & Kelley's Rheumatology, Fishman's Pulmonary Diseases
DEFINITION
Acid Fast Bacilli (AFB) are organisms that, once stained with carbol fuchsin (or fluorochrome dyes), resist decolorization by acid-alcohol. This property - acid fastness - distinguishes them from other bacteria and is used as the basis for their laboratory identification.
The term AFB is synonymous with Mycobacterium tuberculosis in the clinical context, though other species also display the property.
I. ORGANISM
Mycobacterium tuberculosis belongs to the family Mycobacteriaceae, order Actinomycetales.
Morphology:
- Rod-shaped, non-spore-forming, thin, obligate aerobe
- Measures 0.5 μm × 3 μm
- Neutral on Gram staining (appear as "ghost" or "Gram-invisible" organisms)
- High lipid content in cell wall - mycolic acids, arabinogalactan, peptidoglycan form a waxy coat
- This lipid-rich cell wall makes them:
- Resistant to desiccation
- Resistant to most antibiotics
- Responsible for acid fastness
- Slow growing (doubling time ~20 hours; culture takes 4-8 weeks)
Genome: 4.4 million base pairs; high G+C content (65.6%), reflecting aerobic lifestyle.
II. BASIS OF ACID FASTNESS
Acid fastness is due mainly to the organisms' high content of mycolic acids - long-chain, cross-linked fatty acids in the cell wall. These lipids:
- Bind the carbol fuchsin dye tightly
- Form a hydrophobic barrier that resists decolorization with acid-alcohol (3% HCl in 95% ethanol)
Other organisms showing acid fastness:
- Nocardia (partially acid-fast with modified stain)
- Rhodococcus, Gordonia, Tsukamurella
- Legionella micdadei
- Protozoa: Cryptosporidium, Isospora (Cystoisospora)
- M. leprae (AFB causing leprosy)
III. STAINING METHODS FOR AFB
A. Ziehl-Neelsen (ZN) Stain - Classic Method
Principle: Heat-facilitated penetration of carbol fuchsin through waxy cell wall, followed by resistance to acid-alcohol decolorization.
Steps:
- Flood smear with carbol fuchsin; heat gently to steam (3-5 min) - drives dye through lipid-rich wall
- Decolorize with 3% acid-alcohol (HCl in 95% ethanol) - washes out dye from non-AFB
- Counterstain with methylene blue or malachite green
Result: AFB appear as bright red/pink rods against a blue background
B. Kinyoun Cold Stain (Modified ZN)
- Modification that excludes heating
- Uses higher concentration of carbol fuchsin to compensate
- Easier and safer to perform
C. Auramine-Rhodamine Fluorochrome Stain (Preferred Method)
- AFB fluoresce orange-yellow against a dark background
- More sensitive than ZN stain for screening
- Easier to scan under low magnification
- Requires fluorescence microscope (or LED microscope - now available in resource-limited settings)
- Most laboratories use this as the preferred initial stain for clinical specimens
- Positive fluorochrome smears are confirmed with ZN stain
Sensitivity Comparison:
- AFB smear sensitivity: 50-65%
- Culture sensitivity: 80-85%
- A positive smear indicates presence of mycobacteria but does not confirm species as M. tuberculosis
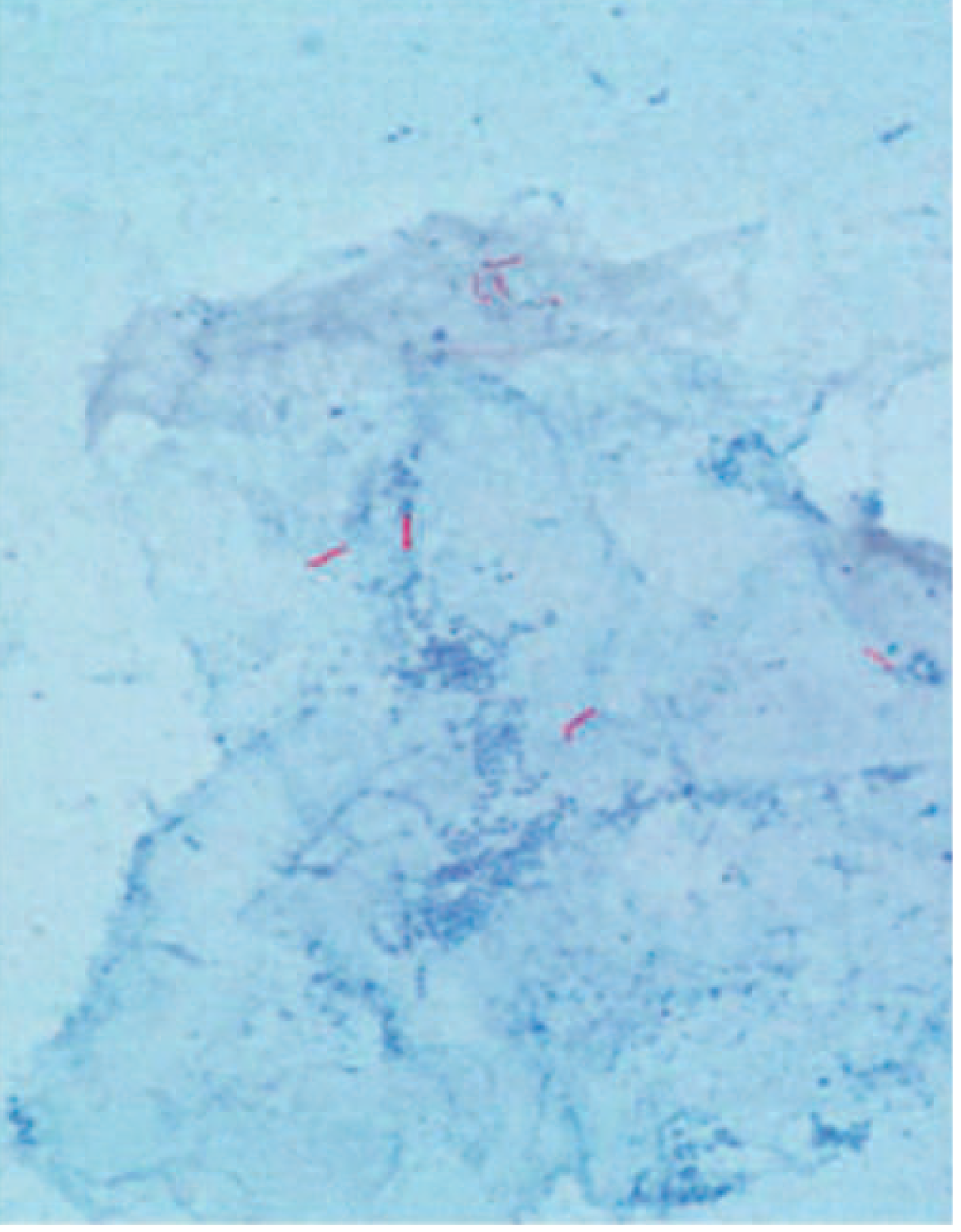
Figure: Ziehl-Neelsen stained smear showing acid fast bacilli (red rods) of M. tuberculosis against blue background
IV. SPECIMENS FOR AFB DIAGNOSIS IN ORTHOPAEDICS
| Specimen | Comments |
|---|---|
| Synovial fluid (joint aspirate) | AFB stain positive in only 20-25%; culture positive in 60-80% |
| Synovial/bone biopsy | Highest yield; enables histology (granuloma) + culture |
| Pus from cold abscess | Aspirated under ultrasound guidance |
| Early morning urine (EMU) x 3 | For genitourinary TB (Ziehl-Neelsen + culture) |
| Sputum | For associated pulmonary TB (3 samples, early morning preferred) |
| CSF (30 mL spun) | For tuberculous meningitis - increases yield |
Key point: Granulomatous inflammation on histology, even without bacteriologic proof, is sufficient evidence to begin anti-TB therapy unless another cause is found.
V. CULTURE
- Gold standard for definitive diagnosis
- Specimens inoculated on:
- Lowenstein-Jensen (LJ) medium (egg-based) - most widely used
- Middlebrook 7H10/7H11 (agar-based) - allows colony morphology
- MGIT (Mycobacteria Growth Indicator Tube) - liquid medium using fluorescent oxygen-sensitive compound; 10 days to 3 weeks positivity; WHO recommended reference standard
- Conventional solid medium: growth in 4-8 weeks at 37°C
- Modern liquid culture methods reduce time to 2-3 weeks
Colony characteristics of M. tuberculosis on LJ medium:
- Slow growing (>3 weeks)
- Buff/cream colored, rough, dry, wrinkled colonies
- "Cauliflower-like" or "serpentine cord" pattern microscopically (due to cord factor - trehalose-6,6-dimycolate)
VI. MOLECULAR DIAGNOSTICS
Xpert MTB/RIF (GeneXpert)
- WHO recommended for rapid diagnosis
- Detects M. tuberculosis DNA and rifampin resistance (rpoB gene mutation) in 2 hours
- For bone and joint TB: pooled sensitivity 81%, specificity 99% vs composite reference standard; 96% sensitivity vs culture
- Can be used on synovial fluid, tissue, pus, CSF
Line Probe Assays (LPA)
- Detects resistance to isoniazid (katG, inhA) and rifampin (rpoB)
- Used for MDR-TB screening
Drug Susceptibility Testing (DST)
- Universal DST recommended by WHO for all TB patients
- Rapid genotypic methods detect resistance to rifampin (rpoB), isoniazid (katG and inhA)
VII. MUSCULOSKELETAL / ORTHOPAEDIC TUBERCULOSIS
Musculoskeletal TB is the 4th most common extrapulmonary manifestation of TB, found in 1-5% of all TB patients.
Pathogenesis:
- M. tuberculosis disseminates hematogenously after acute or reactivated pulmonary infection
- Preference for metaphyses of long bones due to rich blood supply + scarcity of phagocytic cells
- Infection begins in subchondral region → spreads to cartilage, synovium, joint space
- Results in: metaphyseal erosion, cysts, cartilage loss, joint space narrowing
Distribution:
| Site | Frequency |
|---|---|
| Spine (Pott's disease / tuberculous spondylitis) | 50-66% |
| Peripheral joints (hip, knee) | 20-30% |
| Osteomyelitis | 10-20% |
| Tenosynovitis, bursitis | 1-3% |
Important: <50% of musculoskeletal TB patients have radiographic evidence of pulmonary TB
A. Spinal TB (Pott's Disease)
- Most common orthopaedic TB
- Adults: lower thoracic and upper lumbar vertebrae most commonly
- Children: upper thoracic spine
- Two or more adjacent vertebral bodies involved + intervertebral disc (disc early involvement is characteristic)
- Anterior superior or inferior angle of vertebral body affected first
- Collapse → kyphosis (gibbus deformity)
- Paravertebral cold abscess formation:
- Upper spine: may track to chest wall
- Lower spine: presents as psoas abscess tracking to inguinal ligament
- CT/MRI are diagnostic: vertebral body destruction, disc involvement, paravertebral abscess
- Catastrophic complication: Pott's paraplegia (abscess or lesion compressing spinal cord) - medical emergency requiring rapid drainage
B. Hip TB
- Involves head of femur
- Presents with pain and restricted movement
- If unrecognized: joint destruction
C. Knee TB
- Pain and swelling
- Synovial fluid: thick, high protein, variable cell count
- Culture positive in high percentage
D. Solitary vs Multicentric
- Immunocompetent: usually solitary lesion
- AIDS patients: multicentric distribution in ~30%
VIII. TREATMENT
Anti-Tubercular Therapy (ATT) - Standard Regimen
Regimen: 2HRZE / 4HR
| Phase | Duration | Drugs |
|---|---|---|
| Intensive | 2 months | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) |
| Continuation | 4 months | Isoniazid (H) + Rifampicin (R) |
- Cure rate: >90% in drug-susceptible TB
- Daily administration throughout is recommended (intermittent regimens associated with higher failure/relapse/resistance)
- For musculoskeletal TB: extended treatment often used (6-18 months depending on site and response)
Drug Mechanisms
| Drug | Mechanism | Key Toxicity |
|---|---|---|
| Isoniazid (H) | Inhibits mycolic acid synthesis (InhA + KatG) | Peripheral neuropathy, hepatotoxicity |
| Rifampicin (R) | Inhibits RNA polymerase (rpoB) | Hepatotoxicity, drug interactions |
| Pyrazinamide (Z) | Disrupts membrane potential (acidic pH, kills intracellular bacilli) | Hyperuricemia, hepatotoxicity |
| Ethambutol (E) | Inhibits arabinosyltransferase (arabinogalactan synthesis) | Optic neuritis |
Surgical Indications in Orthopaedic TB
- Pott's paraplegia (abscess decompression)
- Failure of conservative management
- Spinal instability / progressive kyphosis requiring stabilization
- Large cold abscess requiring drainage
- Diagnosis (biopsy) when culture/AFB inconclusive
- Joint destruction requiring arthroplasty/arthrodesis
MDR-TB Treatment
- Defined as resistant to at least rifampin (RR-TB) or both isoniazid + rifampin (MDR-TB)
- Requires second-line agents: bedaquiline, linezolid, levofloxacin, moxifloxacin (Group A); clofazimine, cycloserine (Group B)
IX. EPIDEMIOLOGY
- 10.8 million new TB cases estimated globally in 2023 (WHO)
- 1.25 million TB deaths in 2023
- India accounts for 26% of global TB burden
- India is among 8 high-burden countries accounting for 2/3 of global cases
- Musculoskeletal TB: 1-5% of all TB cases; ~10% of extrapulmonary TB in developed nations
X. DIFFERENTIAL DIAGNOSIS OF AFB-POSITIVE LESIONS
| Condition | Distinguishing Feature |
|---|---|
| Pyogenic osteomyelitis | Disc involved early, rapid sclerosis, acute onset |
| Brucella spondylitis | Similar to TB but Brucella serology positive |
| Sarcoidosis | Non-caseating granulomas, AFB negative, ACE elevated |
| Metastatic disease | No disc space narrowing, known primary tumor |
| Fungal osteomyelitis | Fungal culture positive, different organism morphology |
| Non-tuberculous mycobacteria (NTM) | M. avium, M. kansasii - seen in immunocompromised; need species identification |
SUMMARY
Acid Fast Bacilli, principally Mycobacterium tuberculosis, are defined by their resistance to acid-alcohol decolorization due to mycolic acid-rich cell walls. In orthopaedics, AFB cause musculoskeletal TB with spinal TB (Pott's disease) being the most common form. Diagnosis requires ZN staining (20-25% positive in joint fluid), culture on LJ/MGIT medium (gold standard, 60-80% positive), biopsy showing caseating granulomas, and increasingly, rapid molecular tests like Xpert MTB/RIF. Standard ATT (2HRZE/4HR) cures >90% of drug-susceptible cases; surgery is reserved for complications like paraplegia, instability, and abscess drainage.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Jawetz Melnick & Adelberg's Medical Microbiology 28E | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases | Firestein & Kelley's Textbook of Rheumatology
Acid fast bacilli ms ortho 20 marks answer
The previous response covered this topic in full detail. Here is the complete 20-mark MS Ortho answer on Acid Fast Bacilli, reproduced and refined:
Acid Fast Bacilli (AFB)
MS Ortho — 20 Marks
I. DEFINITION
Acid Fast Bacilli are organisms that, once stained with carbol fuchsin, resist decolorization by acid-alcohol (3% HCl in 95% ethanol). This property — acid fastness — is the basis of their laboratory identification.
In clinical orthopaedic practice, AFB = Mycobacterium tuberculosis unless proven otherwise.
II. ORGANISM — MYCOBACTERIUM TUBERCULOSIS
Classification: Family Mycobacteriaceae, Order Actinomycetales
Morphology:
- Rod-shaped, non-spore-forming, thin, obligate aerobe
- Size: 0.5 μm × 3 μm
- Neutral on Gram stain — appears as "ghost" or gram-invisible
- Slow growing — doubling time ~20 hours; culture takes 4-8 weeks
- The M. tuberculosis complex includes: M. tuberculosis, M. bovis, M. africanum, M. caprae, M. microti
Cell Wall — Basis of Acid Fastness:
The cell wall has a unique trilayer architecture:
- Peptidoglycan (inner)
- Arabinogalactan (middle)
- Mycolic acids — long-chain, cross-linked fatty acids (outer, waxy coat)
This lipid-rich outer layer:
- Binds carbol fuchsin tightly and resists acid-alcohol decolorization
- Reduces cell wall permeability → resistance to most antibiotics
- Causes slow growth and resistance to desiccation
- Gives characteristic microscopic "cord factor" appearance (trehalose-6,6-dimycolate causes serpentine cords)
Other organisms showing acid fastness:
- Nocardia (partially acid-fast, modified ZN stain)
- Rhodococcus, Gordonia, Tsukamurella
- Legionella micdadei
- Protozoa: Cryptosporidium, Isospora (Cystoisospora)
- Mycobacterium leprae (AFB causing leprosy)
III. STAINING METHODS
A. Ziehl-Neelsen (ZN) Stain — Classic Method
| Step | Agent | Purpose |
|---|---|---|
| 1. Primary stain | Carbol fuchsin + heat (steaming 3-5 min) | Drives dye through waxy cell wall |
| 2. Decolorization | 3% acid-alcohol | Removes dye from non-AFB organisms |
| 3. Counterstain | Methylene blue or malachite green | Background colour |
Result: AFB appear as bright red/pink rods on a blue background
B. Kinyoun Cold Stain (Modified ZN)
- No heat required
- Uses higher concentration of carbol fuchsin to penetrate without heating
- Easier and safer to perform; widely used
C. Auramine-Rhodamine Fluorochrome Stain (Preferred for Clinical Specimens)
- AFB fluoresce orange-yellow against a dark background
- More sensitive than ZN for initial screening
- Scanned at lower magnification — faster and easier
- Positive results confirmed by ZN stain
- LED fluorescence microscopes now available in resource-limited settings
Sensitivity comparison:
- AFB smear: 50-65% sensitivity
- Culture: 80-85% sensitivity
- A positive smear confirms mycobacteria present but does NOT confirm species as M. tuberculosis
IV. CULTURE (GOLD STANDARD)
| Medium | Type | Time to Growth |
|---|---|---|
| Lowenstein-Jensen (LJ) | Egg-based solid | 4-8 weeks |
| Middlebrook 7H10/7H11 | Agar-based solid | 4-8 weeks |
| MGIT (Mycobacteria Growth Indicator Tube) | Liquid (WHO recommended) | 10 days – 3 weeks |
Colony characteristics of M. tuberculosis on LJ:
- Buff/cream-coloured, rough, dry, wrinkled ("breadcrumb-like" or cauliflower appearance)
- Non-pigmented, slow-growing (>3 weeks)
Microscopic cord formation (serpentine cords) due to cord factor is characteristic.
V. MOLECULAR DIAGNOSTICS
Xpert MTB/RIF (GeneXpert)
- Detects M. tuberculosis DNA and rifampicin resistance (rpoB mutation) within 2 hours
- For bone and joint TB specimens: pooled sensitivity 81%, specificity 99% vs composite reference standard
- 96% sensitivity vs culture
- Can be used on synovial fluid, pus, tissue, CSF
Line Probe Assays (LPA)
- Detects resistance to isoniazid (katG, inhA genes) and rifampicin (rpoB)
- Used for rapid MDR-TB identification
Drug Susceptibility Testing (DST)
- WHO recommends universal DST for all TB patients
- At minimum: rifampicin resistance testing on all initial isolates
VI. SPECIMENS IN ORTHOPAEDIC PRACTICE
| Specimen | AFB Smear Yield | Culture Yield |
|---|---|---|
| Synovial fluid | 20-25% | 60-80% |
| Synovial/bone biopsy | Highest yield | Also allows histology |
| Cold abscess aspirate | Variable | Variable |
| Early morning urine ×3 | For genitourinary TB | For genitourinary TB |
| Sputum ×3 | For associated pulmonary TB | For associated pulmonary TB |
Key principle: Granulomatous inflammation on histology, even without bacteriologic confirmation, is sufficient evidence to begin ATT unless an alternative diagnosis is identified.
VII. MUSCULOSKELETAL TUBERCULOSIS
Epidemiology
- 4th most common extrapulmonary manifestation of TB
- Occurs in 1-5% of all TB patients
- <50% have radiographic evidence of pulmonary TB at presentation
- India bears ~26% of global TB burden (WHO 2023: 10.8 million new cases worldwide)
Pathogenesis
- Droplet inhalation → alveolar macrophage phagocytosis
- Primary pulmonary focus → hematogenous dissemination to skeletal sites
- Predilection for metaphyses of long bones (rich blood supply, few phagocytes)
- Infection begins in subchondral region → spreads to cartilage, synovium, joint space
- Granuloma formation → central caseation → cold abscess (no signs of acute inflammation — hence "cold")
- Disc involvement: spread from anterior angle of vertebral body to adjacent vertebra + disc
Distribution of Musculoskeletal TB
| Site | Frequency |
|---|---|
| Spine (Pott's disease) | 50-66% |
| Peripheral joints (hip, knee) | 20-30% |
| Osteomyelitis (long bones) | 10-20% |
| Tenosynovitis, bursitis | 1-3% |
Immunocompetent: solitary lesion | AIDS patients: multicentric (~30%)
VIII. SPINAL TB (POTT'S DISEASE)
Most common form of musculoskeletal TB
Vertebral Levels:
- Adults: lower thoracic + upper lumbar (T10-L2 most common)
- Children: upper thoracic spine
Pathological Stages:
- Stage I (Synovitis/Pre-destructive): Soft tissue swelling, mild osteopenia
- Stage II (Early destructive): Anterior wedging, disc space narrowing
- Stage III (Late destructive): Vertebral collapse, kyphosis
- Stage IV (Deformity): Gibbus (angular kyphosis), cold abscess, neurological deficit
Cold Abscess Tracking:
- Cervical spine: Retropharyngeal abscess → dysphagia/stridor
- Thoracic spine: Paravertebral abscess → may track along ribs to chest wall
- Lumbar spine: Psoas abscess → inguinal region, groin
Pott's Paraplegia (Catastrophic Complication):
- Abscess or granulation tissue compressing spinal cord
- Medical emergency — requires urgent drainage
- Early (within 2 years): due to abscess/granulation — responds to ATT ± drainage
- Late (>2 years): due to bony collapse/fibrous tissue — often requires surgery
Radiological Features:
- X-ray: Loss of disc space, vertebral end plate erosion, vertebral collapse, paraspinal shadow
- CT: Bony destruction, abscess extent, calcification
- MRI: Most sensitive (100%) and specific (88%) — vertebral body disease, disc destruction, cold abscess, cord compression; allows diagnosis before deformity develops
IX. HISTOPATHOLOGY — THE GRANULOMA
The hallmark histological feature:
Tuberculous (Caseating) Granuloma:
- Central caseous necrosis (cheese-like, acellular)
- Surrounded by epithelioid macrophages (activated macrophages)
- Langhans giant cells (peripheral nuclei in horseshoe arrangement) — pathognomonic
- Rim of lymphocytes
- Outer fibrous capsule
AFB stain on tissue section may demonstrate bacilli within the granuloma.
X. DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Feature |
|---|---|
| Pyogenic osteomyelitis | Disc involved early, acute onset, rapid sclerosis, polymorphs on FNA |
| Brucella spondylitis | Brucella serology positive, disc involved early |
| Sarcoidosis | Non-caseating granulomas, AFB negative, elevated serum ACE |
| Metastatic disease | No disc narrowing, known primary tumour, pedicle destruction |
| Lymphoma/myeloma | Systemic features, bone marrow involvement |
| Fungal osteomyelitis | Fungal culture positive, endemic area history |
| NTM (non-tuberculous mycobacteria) | M. avium, M. kansasii in HIV/immunocompromised |
XI. ANTI-TUBERCULAR THERAPY (ATT)
Standard Regimen: 2HRZE / 4HR
| Phase | Duration | Drugs | Purpose |
|---|---|---|---|
| Intensive | 2 months | H + R + Z + E | Kill majority of bacilli; rapid symptom relief |
| Continuation | 4 months | H + R | Eliminate persisting bacilli; prevent relapse |
Cure rate: >90% in drug-susceptible TB. Daily administration throughout is recommended.
Mechanism of Action
| Drug | Target | Key Adverse Effect |
|---|---|---|
| Isoniazid (H) | Mycolic acid synthesis (InhA/KatG) | Peripheral neuropathy, hepatotoxicity |
| Rifampicin (R) | RNA polymerase (rpoB) | Hepatotoxicity, drug interactions, orange urine |
| Pyrazinamide (Z) | Membrane potential (kills intracellular bacilli in acidic pH) | Hyperuricemia, hepatotoxicity |
| Ethambutol (E) | Arabinosyltransferase (arabinogalactan synthesis) | Optic neuritis (dose-dependent, reversible) |
Musculoskeletal TB Duration:
- Spine TB (Pott's disease): 6-9 months (some centres extend to 12-18 months)
- Peripheral joint TB: 6-9 months
- Treatment is primarily conservative (ATT); surgery for specific indications
MDR-TB (Multi-Drug Resistant):
- Defined as resistance to rifampicin ± isoniazid
- Requires Group A drugs: bedaquiline, linezolid, levofloxacin/moxifloxacin
- Plus Group B: clofazimine, cycloserine
XII. SURGICAL INDICATIONS IN ORTHOPAEDIC TB
- Pott's paraplegia — abscess drainage ± decompression (medical emergency)
- Spinal instability — fixation and fusion
- Progressive kyphosis (gibbus) — surgical correction
- Diagnostic biopsy — when AFB/culture inconclusive
- Large cold abscess not responding to aspiration
- Joint destruction — arthroplasty or arthrodesis (after disease control with ATT)
- Failure of conservative management
SUMMARY TABLE
| Feature | Detail |
|---|---|
| Organism | M. tuberculosis — rod-shaped aerobe, 0.5 × 3 μm |
| Acid fastness | Due to mycolic acids in cell wall |
| Best stain | Auramine-rhodamine (fluorochrome) for screening; ZN for confirmation |
| Gold standard diagnosis | Culture on MGIT / LJ medium |
| Rapid molecular test | Xpert MTB/RIF (2 hours) |
| Most common ortho site | Spine (Pott's disease) — 50-66% |
| Hallmark histology | Caseating granuloma with Langhans giant cells |
| Standard treatment | 2HRZE / 4HR (>90% cure) |
| Key complication | Pott's paraplegia — urgent surgery |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Jawetz Medical Microbiology 28E | Murray & Nadel's Respiratory Medicine | Fishman's Pulmonary Diseases | Firestein & Kelley's Textbook of Rheumatology
This is a shared conversation. Sign in to Orris to start your own chat.