Total Intravenous Anaesthesia - MD Anaesthesia Pg Exam - 30 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I now have comprehensive data from Miller's Anesthesia and Barash to write a thorough 30-mark MD Anaesthesia PG exam answer. Let me compose it now.
Total Intravenous Anaesthesia (TIVA)
MD Anaesthesia PG Exam Answer - 30 Marks
Definition
Total Intravenous Anaesthesia (TIVA) is a technique of general anaesthesia in which all anaesthetic agents are administered exclusively by the intravenous route, without the use of any volatile inhalational agents. The components of anaesthesia - hypnosis, analgesia, and muscle relaxation - are all delivered intravenously.
Historical Background
The concept of intravenous anaesthesia dates to 1656, when Christopher Wren administered opium intravenously via a quill. Modern TIVA became practical only with the introduction of propofol in the 1980s and the development of target-controlled infusion (TCI) systems. Kruger-Thiemer first described the theoretical framework for achieving steady-state blood concentrations using multi-compartment pharmacokinetic models, later clinically implemented by Schwilden and colleagues. The bolus-elimination-transfer (BET) scheme became the cornerstone of TCI design.
Components of TIVA
| Component | Drug(s) |
|---|---|
| Hypnotic | Propofol (most common), Ketamine, Midazolam, Etomidate |
| Opioid/Analgesic | Remifentanil (preferred), Fentanyl, Sufentanil, Alfentanil |
| Muscle Relaxant | Vecuronium, Rocuronium, Cisatracurium |
The propofol + remifentanil combination is the gold standard TIVA regimen due to their complementary pharmacokinetics.
Pharmacokinetics of Key Drugs
Propofol
Propofol (2,6-di-isopropyl phenol) is the cornerstone of TIVA.
Distribution:
- Highly lipophilic; rapid redistribution after bolus
- Three-compartment pharmacokinetic model
- Initial distribution half-life: 2-8 minutes
- Slow distribution half-life: 30-70 minutes
- Elimination half-life: 4-23.5 hours
- Volume of distribution at steady state: 150-700 L
- Central compartment volume: 6-40 L (smaller in elderly due to reduced cardiac output)
Metabolism:
- Clearance: 1.5-2.2 L/min (exceeds hepatic blood flow)
- Hepatic oxidation to 1,4-diisopropyl quinol, followed by glucuronide conjugation
- Extrahepatic metabolism confirmed (kidney accounts for ~30% of clearance; lungs contribute 20-30% first-pass)
- Propofol inhibits CYP3A4 (even at 3 mcg/mL, reduces CYP3A4 activity by ~37%)
Context-Sensitive Half-Time (CSHT):
- For infusions up to 8 hours, CSHT remains <40 minutes
- Since the required decrease in concentration for awakening is <50%, recovery remains rapid even after prolonged infusion - this makes propofol ideal for TIVA
Remifentanil
- Ultra-short-acting synthetic mu-opioid agonist
- Ester hydrolysis by nonspecific plasma and tissue esterases (independent of hepatic/renal function)
- Context-sensitive half-time: 3-5 minutes (does NOT increase with infusion duration)
- Elimination half-life: ~8-20 minutes
- Dose: 0.05-2 mcg/kg/min by infusion
- Uniquely, neonates have more rapid clearance than older children due to larger volume of distribution and esterase activity
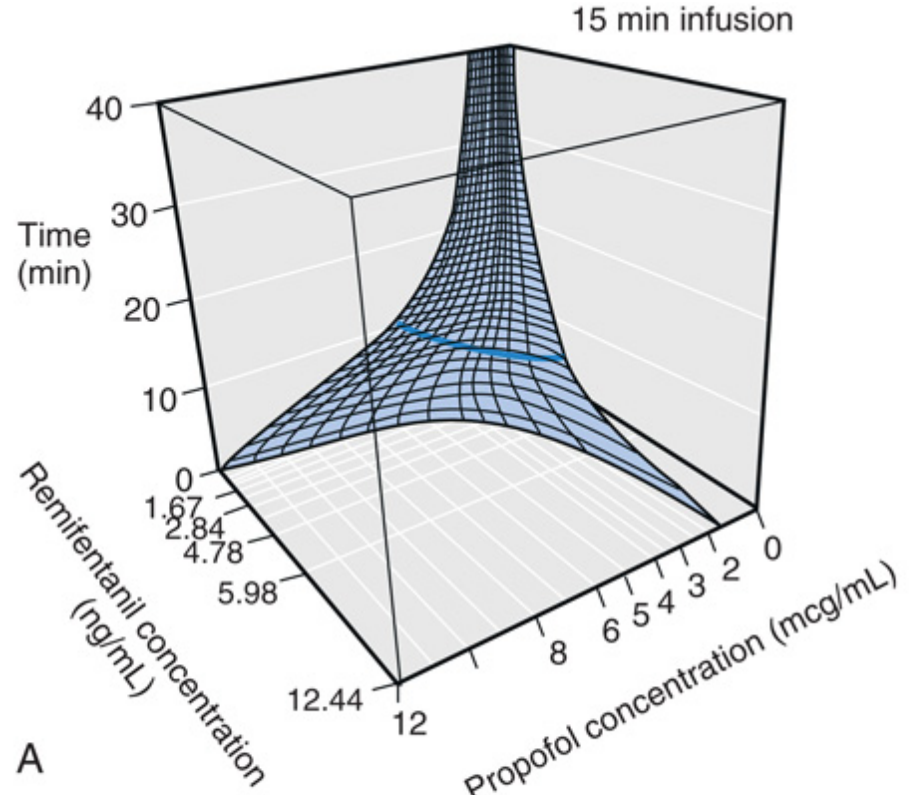
Remifentanil + Propofol interaction: When added to a propofol plasma concentration of 2 mcg/mL, remifentanil concentration required for suppression of surgical stimuli follows a synergistic interaction. The optimal combination is propofol ~2.5 mcg/mL and a lower remifentanil concentration to minimize recovery time.
Target-Controlled Infusion (TCI)
TCI is a computer-controlled infusion system that uses pharmacokinetic models to calculate and deliver drug infusions targeting a clinician-specified plasma or effect-site concentration.
Principle - BET Scheme
The Bolus-Elimination-Transfer (BET) scheme works via:
- Bolus: Initial bolus to rapidly achieve target concentration in the central compartment
- Elimination infusion: Constant rate infusion to replace drug lost by elimination
- Transfer infusion: Exponentially declining infusion to replace drug redistributing to peripheral compartments
Effect-Site (Ce) vs. Plasma (Cp) Targeting
- Plasma TCI (Cp target): Targets the plasma concentration; effect-site concentration lags behind due to the blood-brain equilibration delay (ke0)
- Effect-site TCI (Ce target): Targets the biophase/effect-site concentration; produces faster onset by temporarily overshooting plasma concentration
Propofol TCI Models
| Model | Key Features |
|---|---|
| Marsh | Simple three-compartment; uses total body weight; commonly used in clinical practice |
| Schnider | Uses age, total body weight, height, lean body mass; includes effect-site; more refined for elderly |
| Eleveld | Most recent; allometric scaling; better accuracy across a wide range of body weights including obese patients |
Schnider model limitation: Uses the James equation for lean body mass calculation, which yields negative values in morbidly obese patients - making it invalid in this population.
For obese patients: Adjusted body weight (ABW = ideal weight + 40% × [total - ideal weight]) with Marsh or Schnider models, or the Eleveld model, provides best accuracy.
Remifentanil TCI
- Minto model: Uses age, weight, height, and lean body mass; accounts for age-related changes in pharmacokinetics
Induction and Maintenance Doses
| Agent | Induction | Maintenance |
|---|---|---|
| Propofol (manual) | 1-2.5 mg/kg IV | 4-12 mg/kg/h (66-200 mcg/kg/min) |
| Propofol TCI (Cp) | Target 4-8 mcg/mL | Target 3-6 mcg/mL |
| Remifentanil infusion | 0.5-1 mcg/kg/min | 0.05-2 mcg/kg/min |
| Ketamine | 1-2 mg/kg IV | 1-3 mg/kg/h |
Advantages of TIVA
- Reduced PONV - Propofol has intrinsic antiemetic properties; avoiding volatile agents significantly reduces postoperative nausea and vomiting
- Safe in malignant hyperthermia (MH) susceptible patients - TIVA avoids all triggering volatile agents and succinylcholine; it is the technique of choice in MH-susceptible individuals
- Better maintenance of surgical field - Reduces bronchospasm; ideal for airway surgery, ENT, and sinus surgery (TIVA with remifentanil reduces coughing and improves surgical conditions)
- Smooth induction and emergence - No excitation on induction; rapid, clear-headed recovery
- Reduced pollution - No theatre pollution from volatile agents
- Better neurophysiologic monitoring - TIVA (propofol + remifentanil) causes less suppression of evoked potentials (MEP, SSEP) compared to volatile agents; preferred for spine and neurosurgery
- Use in remote locations - Can be administered without an anaesthetic machine
- Facial nerve monitoring - Propofol + remifentanil provides reliable conditions for facial nerve monitoring during ear surgery (Choe et al.)
- Reduced airway reactivity - Propofol suppresses laryngeal reflexes; ideal with LMA
- Anti-epileptic properties - Propofol useful in patients with epilepsy
- Opioid-free TIVA variants - Reduces PONV further in bariatric surgery beyond triple prophylaxis
Disadvantages of TIVA
- Risk of intraoperative awareness - No reliable exhaled agent monitoring; reliance on PK models which may be inaccurate; BIS/processed EEG monitoring strongly recommended
- Venous access dependent - Disconnection, dislodgement, or extravasation can cause awareness or drug toxicity
- Propofol infusion syndrome (PRIS) - Rare but life-threatening complication with high-dose, prolonged infusions (>4 mg/kg/h for >48h); characterised by metabolic acidosis, rhabdomyolysis, cardiac failure, lipaemia
- Injection pain - Propofol causes burning on injection (50-70% if given into small peripheral vein); using large antecubital vein, lidocaine pretreatment, or using lipid formulations mitigates this
- Haemodynamic effects - Propofol causes vasodilation and myocardial depression, especially at induction; caution in hypovolaemic and elderly patients
- Cost - Higher cost than inhalational anaesthesia for routine cases
- Pharmacokinetic variability - TCI models are population-based averages; individual variability (obesity, elderly, hepatic disease, cardiac failure) can lead to under- or overdosing
- Supports microbial growth - Propofol's lipid emulsion supports bacterial and fungal growth; strict aseptic handling required; discard within 12 hours of opening
- Apnoea - High-dose propofol causes respiratory depression and apnoea
- Dose calculation complexity - Manual TIVA requires careful calculation of infusion rates
Indications for TIVA
- Malignant hyperthermia susceptibility (absolute)
- Airway surgery (shared airway, laser surgery, microlaryngoscopy)
- ENT surgery - sinus surgery, middle ear surgery, thyroidectomy
- Neuroanaesthesia with neurophysiological monitoring
- Neurosurgery requiring cerebral protection (propofol reduces CMRO2)
- Patients prone to PONV
- Remote anaesthesia (MRI, radiotherapy, catheterisation labs)
- Robotic and laparoscopic surgery
- Paediatric anaesthesia (where TIVA is feasible and MH risk exists)
- Day-case and ambulatory surgery
Monitoring During TIVA
Depth of Anaesthesia Monitoring
Monitoring depth of anaesthesia is particularly important in TIVA because there is no end-tidal volatile agent concentration to guide dosing.
Processed EEG monitors:
- BIS (Bispectral Index): Most widely used; value 40-60 = adequate anaesthesia; <40 = deep; >60 = risk of awareness
- Entropy (State Entropy / Response Entropy)
- Narcotrend
BIS target range during TIVA: 40-60. An adequate TIVA requires BIS monitoring as TCI models alone cannot guarantee adequate depth in every individual.
Standard monitoring (AAGBI minimum):
- Continuous ECG
- SpO2 pulse oximetry
- NIBP (or IBP in high-risk patients)
- Capnography (EtCO2)
- Neuromuscular monitoring (if muscle relaxants used)
- Temperature monitoring
TIVA in Special Populations
Elderly Patients
- Reduced central compartment volume - higher peak plasma concentrations after bolus
- Reduced clearance and cardiac output
- Reduce induction dose of propofol by 30-50%
- Schnider model incorporates age as a covariate and is preferred
Obese Patients
- Marsh model using total body weight overestimates required dose
- Use adjusted body weight or Eleveld model
- Effect-site TCI with Schnider model risks negative lean body mass calculations
Paediatric Patients
- TIVA increasingly used; propofol + remifentanil are the main agents
- Remifentanil clearance is paradoxically more rapid in neonates (esterase-based clearance; not liver/kidney dependent)
- Propofol not licensed for sedation in paediatric ICU (<16 years) due to risk of PRIS
Hepatic/Renal Impairment
- Propofol clearance minimally affected by liver disease (extrahepatic metabolism predominates)
- Remifentanil is safe in renal and hepatic failure (ester hydrolysis)
Propofol Infusion Syndrome (PRIS)
A rare but potentially fatal complication associated with high-dose propofol infusion.
Risk factors:
- Dose >4 mg/kg/h (>67 mcg/kg/min)
- Duration >48 hours
- High carbohydrate, low fat intake
- Concomitant catecholamine or steroid infusion
- Sepsis, brain injury
Features (SCALP mnemonic):
- S - Severe metabolic acidosis (lactic/anion gap)
- C - Cardiac failure (new right bundle branch block, ST changes, arrhythmias)
- A - Acute rhabdomyolysis
- L - Lipaemia (hypertriglyceridaemia)
- P - Pancreatic enlargement / pancreatitis
Management: Stop propofol immediately, haemodynamic support, renal replacement therapy if needed.
TIVA vs. Inhalational Anaesthesia - Key Comparison
| Parameter | TIVA | Inhalation |
|---|---|---|
| PONV | Significantly lower | Higher |
| Emergence quality | Smoother, less agitation | More agitation possible |
| MH safety | Safe | Contraindicated in MH |
| Theatre pollution | None | Present |
| Intraoperative awareness | Higher risk (no exhaled monitor) | Lower risk (MAC-based monitoring) |
| Cost | Higher | Lower |
| Neurophysiology | Better EP preservation | Volatile agents suppress EPs |
| Recovery | Rapid (propofol CSHT <40 min) | Variable with long volatile use |
Closed-Loop TIVA
An advanced development where processed EEG feedback (BIS) is used to automatically adjust the TCI target concentration - creating a truly automated anaesthetic delivery system. Research demonstrates small improvements in haemodynamic control and BIS stability with closed-loop advisory display systems compared to standard TCI.
Summary Points for Exam
- TIVA = all anaesthetic components given IV; no volatile agents
- Gold standard regimen: propofol + remifentanil ± muscle relaxant
- Propofol is ideal for TIVA: rapid onset, short CSHT (<40 min for 8h infusions), antiemetic
- Remifentanil: ester hydrolysis, CSHT 3-5 min regardless of infusion duration
- TCI uses BET schemes based on 3-compartment PK models
- Common TCI models: Marsh (simple, total body weight) and Schnider (includes age, LBM; better for elderly)
- Plasma TCI vs Effect-site TCI - effect-site gives faster onset by overshooting plasma concentration
- TIVA is technique of choice in malignant hyperthermia and neurosurgery with neurophysiological monitoring
- Main risk: intraoperative awareness - always use processed EEG (BIS 40-60)
- PRIS: high-dose, prolonged propofol - present with lactic acidosis, cardiac failure, rhabdomyolysis
- Propofol: injection pain, supports microbial growth, CYP3A4 inhibitor, extrahepatic metabolism (30% renal, 20-30% pulmonary)
- TIVA reduces PONV significantly - benefit particularly in bariatric, ENT, and gynaecological surgery
Sources: Miller's Anesthesia 10th edition; Barash Clinical Anesthesia 9th edition; Morgan & Mikhail Clinical Anesthesiology 7th edition; Scott-Brown's Otorhinolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.