Explain the menstrual cycle with hormonal changes and diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compose the full, detailed answer.
The Menstrual Cycle: Hormonal Changes and Phases
Diagram
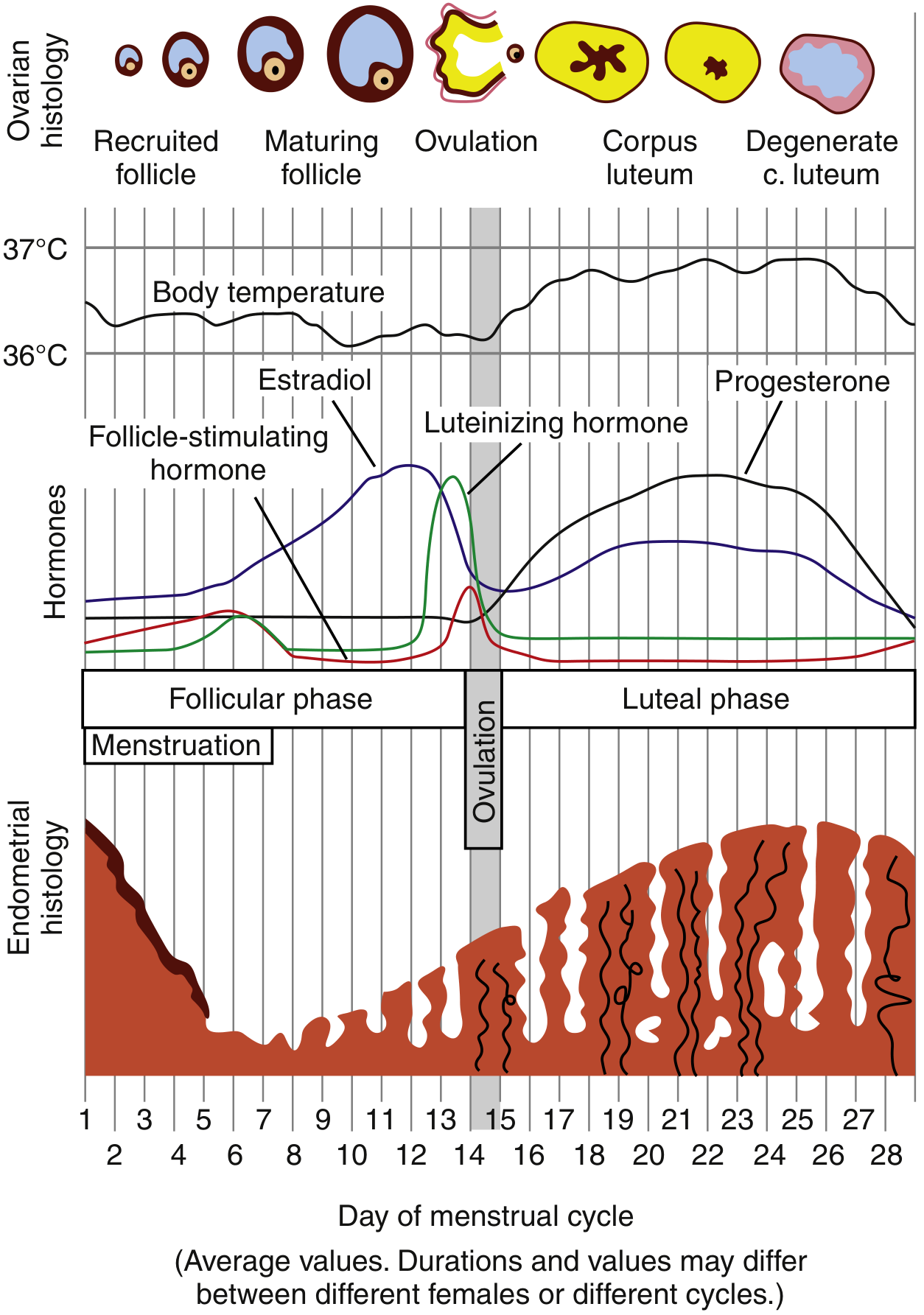
The diagram shows body temperature, FSH, LH, estradiol, and progesterone curves across days 1-28, alongside ovarian follicle development (top) and endometrial thickness changes (bottom). - Rosen's Emergency Medicine
Overview
The menstrual cycle averages 28 days (range: 21-35 days) and is a coordinated interaction among the hypothalamus, anterior pituitary, ovary, and uterus. By convention, Day 1 is the first day of menstrual bleeding. The cycle is divided into two major phases:
- Follicular phase (Days 1-14): also called the proliferative phase
- Luteal phase (Days 14-28): also called the secretory phase
Level 1: Hypothalamic Control - GnRH
The entire cycle is driven by GnRH (gonadotropin-releasing hormone), a decapeptide produced by neurons in the arcuate nucleus of the hypothalamus. GnRH must be released in a pulsatile fashion - continuous infusion causes downregulation of pituitary GnRH receptors and suppresses gonadotropins (this is the principle behind GnRH agonist therapy).
- Follicular phase: frequent, small-amplitude GnRH pulses → favors LH secretion
- Late follicular phase: increased pulse frequency and amplitude
- Luteal phase: longer intervals between pulses, higher amplitude → favors FSH secretion
GnRH has a very short half-life (2-4 minutes) due to rapid proteolytic cleavage. - Berek & Novak's Gynecology, p. 270
Phase 1: Follicular Phase (Days 1-14)
Menstruation (Days 1-5)
At the start of the cycle, estrogen and progesterone levels are at their nadir. The withdrawal of hormonal support causes:
- Vasospasm of the spiral arteries (mediated by prostaglandin F2α)
- Necrosis and shedding of the stratum functionale of the endometrium
- Menstrual bleeding (approximately 50-80 mL blood loss)
The stratum basale (supplied by short, straight basilar arteries) is preserved and serves as the regenerative layer.
Follicle Recruitment and Growth (Days 1-13)
- At the start of each cycle, FSH rises slightly (due to low estrogen/progesterone feedback from the previous cycle)
- FSH stimulates several primordial follicles to enlarge and develop an antrum (cavity filled with follicular fluid)
- By Day 6, one dominant follicle is selected - the one best able to produce intrafollicular estrogen for final maturation
- The theca interna cells of the follicle produce androgens, which are aromatized to estrogen (17β-estradiol) by the granulosa cells (the two-cell theory)
- Rising estradiol exerts negative feedback on FSH, causing FSH to fall, which leads to atresia of all non-dominant follicles
Endometrial Changes (Proliferative Phase)
Estradiol stimulates:
- Rapid growth of the endometrium (Days 5-14)
- Lengthening and straightening of uterine glands (not yet secretory)
- Elongation of spiral arteries
- Cervical mucus becomes copious, watery, elastic, and shows "ferning" on a glass slide - channels in the mucus help sperm penetrate the cervix
The LH Surge and Ovulation (Day 14)
As the dominant follicle matures, estradiol rises to a critical threshold (~200 pg/mL sustained for ~50 hours). This triggers a switch from negative to positive feedback, producing the massive LH surge (and a smaller FSH surge). This is the most dramatic hormonal event of the cycle.
- The LH surge triggers resumption of meiosis I in the oocyte (previously arrested in prophase I since fetal life)
- The follicle ruptures approximately 36 hours after the LH surge peak
- The secondary oocyte is released and picked up by the fimbriated ends of the fallopian tube
- The secondary oocyte immediately begins meiosis II, but arrests again at metaphase II - it only completes meiosis II if fertilized by a sperm
Minor intraperitoneal bleeding at ovulation may cause brief lower abdominal pain known as Mittelschmerz ("middle pain"). - Ganong's Review of Medical Physiology, 26e, p. 404
Phase 2: Luteal Phase (Days 14-28)
Corpus Luteum Formation
After ovulation, the ruptured follicle fills with blood (corpus hemorrhagicum), then the granulosa and theca cells luteinize under continued LH stimulation, becoming the corpus luteum (yellow body, rich in lipid-laden luteal cells). VEGF drives its vascularization.
The corpus luteum secretes both estrogen and progesterone in large amounts.
Hormonal Profile
| Hormone | Level | Effect |
|---|---|---|
| Progesterone | Rises sharply, peaks ~Day 21 | Dominant hormone of luteal phase |
| Estradiol | Second smaller peak | Supports endometrium |
| LH & FSH | Suppressed by negative feedback | Fall to basal levels |
| Inhibin A | Rises | Selectively suppresses FSH |
Endometrial Changes (Secretory Phase)
Under progesterone + estrogen:
- Endometrial proliferation slows; thickness decreases slightly
- Uterine glands become tortuous and coiled, accumulate glycogen in vacuoles, and increase mucus secretion
- Stroma becomes edematous
- Spiral arteries elongate and become coiled, ready for implantation
- Cervical mucus becomes thick, scant, non-elastic - does not fern (sperm penetration is no longer needed)
Progesterone also has a thermogenic effect - basal body temperature rises by ~0.2-0.5°C in the luteal phase (the basis of the rhythm method for contraception). - Costanzo Physiology 7e, p. 479
Luteal Regression (Without Pregnancy)
If fertilization does not occur:
- The corpus luteum degenerates around Day 24-26 (luteolysis)
- Estrogen and progesterone levels fall sharply
- Loss of hormonal support causes endometrial ischemia and necrosis
- The cycle restarts on Day 1 (next menstruation)
If Pregnancy Occurs
The trophoblast of the implanting embryo secretes hCG (human chorionic gonadotropin) by Day 8-10, which rescues the corpus luteum from degeneration. The corpus luteum continues producing progesterone to maintain the endometrium until the placenta takes over at ~8-10 weeks (luteo-placental shift).
Hormone Summary Table
| Phase | Days | Dominant Hormone | FSH | LH | Estradiol | Progesterone |
|---|---|---|---|---|---|---|
| Menstruation | 1-5 | - | Low-rising | Low | Low | Low |
| Early follicular | 1-7 | FSH | Rising | Low | Rising | Low |
| Late follicular | 8-13 | Estradiol | Falling | Low | Peak (1st) | Low |
| Ovulation | 14 | LH surge | Small surge | Massive surge | Slight drop | Low |
| Early luteal | 15-20 | Progesterone | Suppressed | Falling | Rising (2nd peak) | Rising |
| Mid-luteal | 21-23 | Progesterone | Low | Low | 2nd peak | Peak |
| Late luteal | 24-28 | - | Rising (for next cycle) | Low | Falling | Falling |
Feedback Mechanisms
| Signal | Effect on Pituitary | Timing |
|---|---|---|
| Low estrogen | Negative feedback - allows FSH rise | Menstruation / early follicular |
| High estrogen (sustained) | Positive feedback - triggers LH surge | Late follicular (Day 13) |
| Progesterone + estrogen | Negative feedback - suppresses FSH & LH | Luteal phase |
| Inhibin B (from granulosa cells) | Selectively suppresses FSH | Follicular phase |
| Inhibin A (from corpus luteum) | Selectively suppresses FSH | Luteal phase |
Clinical Correlations
- Anovulatory cycles: No LH surge, no corpus luteum, no progesterone rise - common at menarche and perimenopause; causes irregular or heavy bleeding
- GnRH agonists: Continuous administration desensitizes the pituitary, suppressing gonadotropins - used in endometriosis, fibroids, IVF protocols
- Clomiphene: Blocks estrogen receptors at the hypothalamus, preventing negative feedback, leading to increased FSH release and follicular recruitment - used for ovulation induction
- Basal body temperature charting: Rise in BBT confirms ovulation (progesterone thermogenic effect)
- Cervical mucus monitoring: Spinnbarkeit (elasticity) peaks at ovulation
Sources:
- Berek & Novak's Gynecology, Chapter 7 (Menstrual Cycle Physiology), pp. 264-270
- Ganong's Review of Medical Physiology, 26th Edition, Chapter 22, pp. 404-406
- Costanzo Physiology, 7th Edition, p. 479
This is a shared conversation. Sign in to Orris to start your own chat.