Take Cummings as reference and give essay answer on torp and porp in ossiculoplasty for Ent pg exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the core content needed. Let me compose the comprehensive PG exam essay.
TORP and PORP in Ossiculoplasty
(Reference: Cummings Otolaryngology — Head and Neck Surgery, 7th Edition)
Introduction
Ossiculoplasty aims to reconstruct the middle ear sound-conducting mechanism and may be performed either concurrently with tympanoplasty or in a staged fashion. The primary goal is to re-establish efficient transfer of induced vibratory energy from the tympanic membrane (TM) to the stapes footplate, thereby reducing the air-bone gap (ABG). The Partial Ossicular Replacement Prosthesis (PORP) and Total Ossicular Replacement Prosthesis (TORP) are the two fundamental alloplastic devices used in modern ossiculoplasty.
Definition and Distinction
| Feature | PORP | TORP |
|---|---|---|
| Full name | Partial Ossicular Replacement Prosthesis | Total Ossicular Replacement Prosthesis |
| Stapes superstructure | Present | Absent |
| Medial end rests on | Stapes capitulum | Stapes footplate |
| Lateral end contacts | TM (via cartilage cap) or malleus handle | TM (via cartilage cap) or malleus handle |
| Typical ABG closure (<20 dB) | 50–85% | 40–50% |
A PORP is used when the stapes superstructure is intact; a TORP is used when the superstructure is absent.
Pathophysiology Requiring Ossiculoplasty
Ossicular Discontinuity
Chronic otitis media — particularly cholesteatoma — is the most common cause of ossicular erosion. The long process of the incus is most vulnerable due to its single nutrient vessel supply. Erosion can range from loss of the lenticular process to complete destruction of the incus body and stapes superstructure. Longitudinal temporal bone fractures also cause incus dislocation.
Audiometric hallmark: Near-maximal (55–60 dB) flat conductive hearing loss; tympanogram shows a deep Ap pattern (high compliance due to flail ossicular chain).
Ossicular Fixation
Tympanosclerosis and chronic otomastoiditis can immobilize ossicles. Otosclerosis is the classic cause of stapes fixation.
Audiometric hallmark: Carhart notch (5–10–15–5 dB dip in bone conduction at 500, 1000, 2000, 4000 Hz); flat tympanogram; worst air conduction in low frequencies.
Classification of Ossicular Defects (Austin–Kartush System)
The Austin–Kartush classification defines the ossicular status relevant to prosthesis choice:
| Type | Malleus | Stapes Superstructure | Prosthesis |
|---|---|---|---|
| A | Present | Present | Incus interposition / PORP |
| B | Absent | Present | PORP |
| C | Present | Absent | TORP |
| D | Absent | Absent | TORP |
This classification guides the surgeon's intraoperative decision.
Materials Used in Ossiculoplasty
1. Autografts
- Incus interposition (sculpted native incus): historically the gold standard
- Advantages: biocompatible, low cost, immediately available, low extrusion rate
- Disadvantages: risk of cholesteatoma recurrence from residual matrix; requires time and skill to sculpt; may be demineralized or eroded
- Cartilage (tragal, conchal, or costal): used primarily as an interposition layer between the prosthesis head and the TM to reduce extrusion
2. Alloplastic (Allograft) Prostheses
Three principal groups:
| Class | Examples |
|---|---|
| Polymers | High-density polyethylene sponge (Plastipore, Polycel), PTFE (Teflon), silicone |
| Ceramics | Hydroxyapatite (HA), Bioglass, Ceravital |
| Metals | Titanium (current standard) |
Hydroxyapatite (HA)
- Undergoes osseointegration — bonds to bone without fibrous encapsulation
- Available in porous and dense forms
- Disadvantage: brittle, difficult to sculpt; top-heavy designs tend to tilt
- Often combined with Plastipore shaft (HA platform + Plastipore body) to exploit bone-bonding while enabling easy length adjustment
Titanium
- Currently the most widely used material
- Low mass (≤4 mg), high rigidity — closest in mass to the ossicles being replaced
- Reduces acoustic impedance and sound damping, particularly at high frequencies
- Open headplate design allows superior intraoperative visualization
- Claw-like medial design grips the stapes head (PORP) securely
- Not top-heavy → stays upright without propping
- Surgeon-friendly: reduced learning curve
PORP — Surgical Details
Indication: Missing incus (most common ossicular abnormality in chronic OM), with intact stapes superstructure, intact malleus, and adequate TM mobility.
Technique:
- After disease clearance, the stapes capitulum and malleus handle are exposed.
- A PORP of appropriate length is selected or adjusted (adjustable vs. fixed-length designs available).
- A 0.5–0.7 mm conchal or tragal cartilage cap is fitted over the prosthesis head. The perichondrium is stripped from the prosthesis-contact surface and left intact on the TM-contact surface.
- The prosthesis is placed perpendicular to the TM, in a vertical plane from the center of the stapes footplate.
- Stabilized with minimal tension from the drum.
- Silastic sheeting or hyaluronic acid sheets may be placed on the promontory to prevent adhesions.
Fig. 145.11 — PORP bridging the stapes capitulum to malleus handle with a cartilage cap:
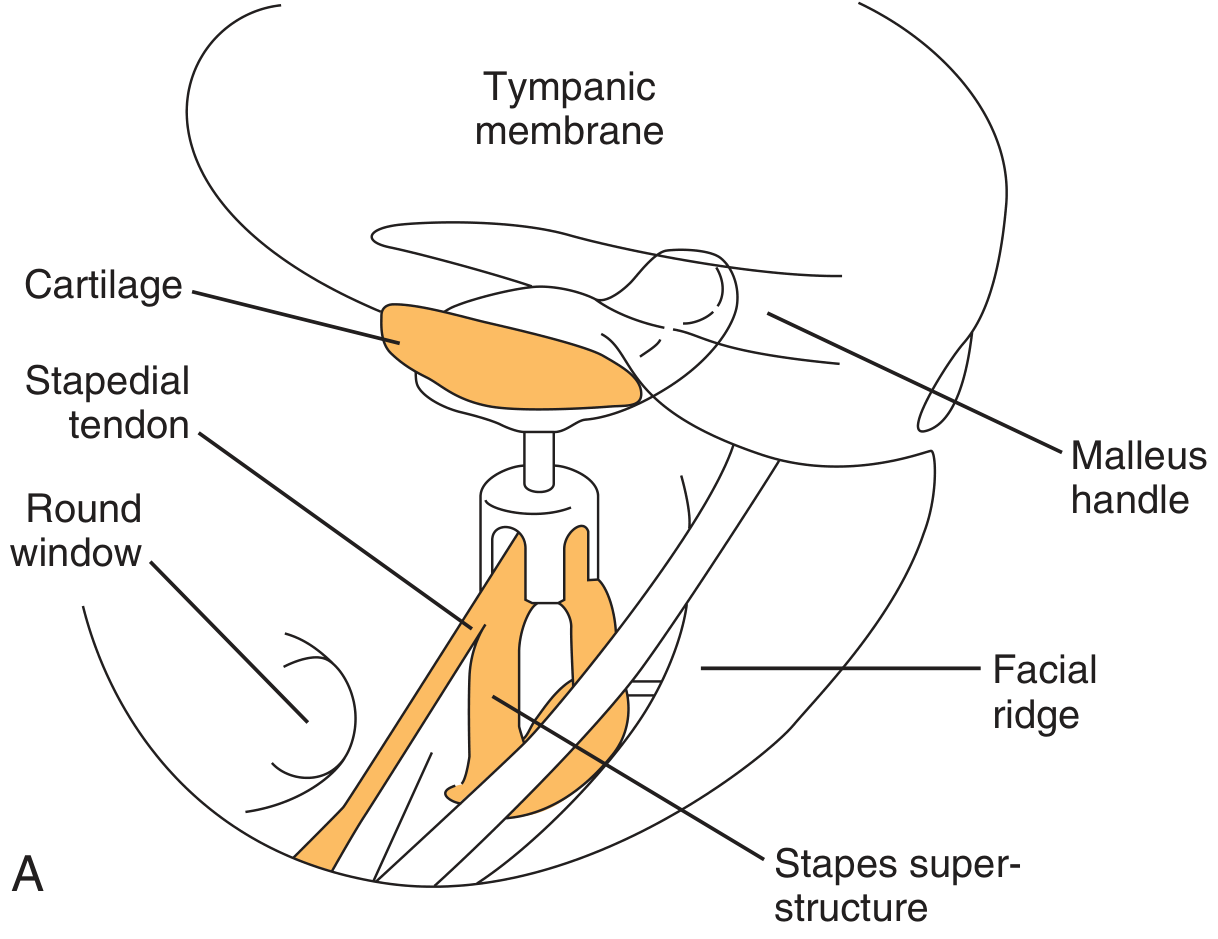
Intraoperative photo (panel D, Fig. 145.11) showing PORP in situ with cartilage cap:

TORP — Surgical Details
Indication: Absent stapes superstructure (crura eroded), with intact or mobile footplate.
Technique:
- The stapes footplate is identified and confirmed to be mobile (a fixed footplate significantly worsens outcome).
- A TORP of appropriate length spans from the stapes footplate to the TM (or malleus handle).
- A cartilage cap is interposed between the prosthesis head and the TM — essential to prevent extrusion.
- The TORP must be placed in parallel piston motion to the footplate — perpendicular orientation is critical.
- Length matters: a short TORP fails to transmit high frequencies and risks dislodgement; a long TORP over-tensions the TM, dampens low frequencies, and risks footplate fracture, subluxation, or perilymph fistula.
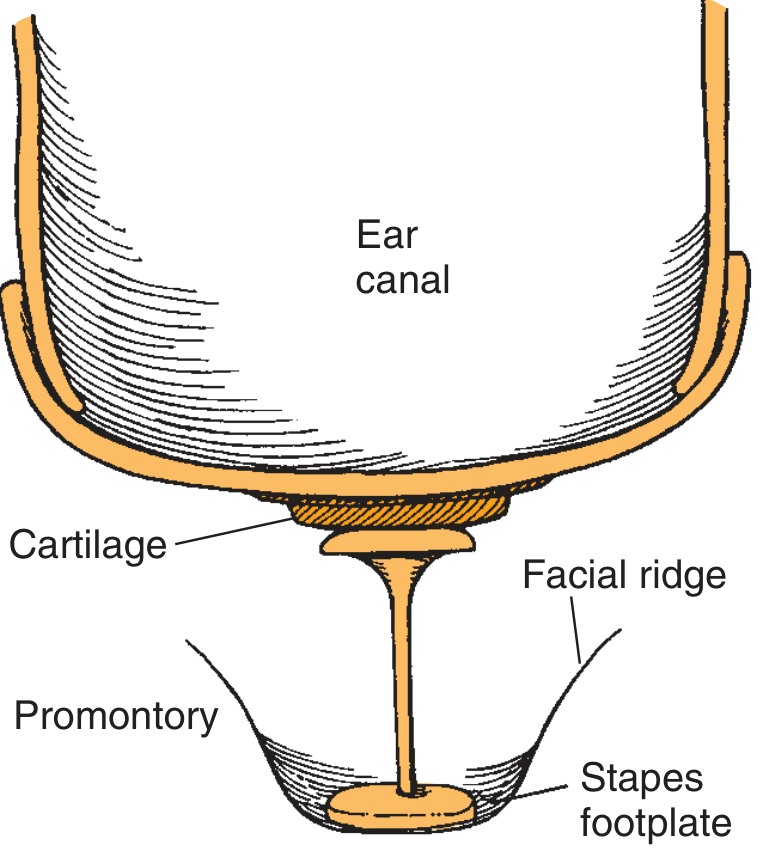
Fig. 145.12–145.13 — TORP positioned from stapes footplate to TM:
Factors Determining Prosthesis Length and Position
The malleus-stapes relationship is the key geometric determinant:
- Favorable geometry: Narrow anteroposterior distance with deeper middle ear → prosthesis lies in a more vertical position → optimal energy transfer
- Unfavorable geometry: Wide AP distance, shallow middle ear → prosthesis lies more horizontally → poor hearing result
In the unfavorable situation, the medial end should be placed on the footplate rather than the capitulum, and the lateral end on the posterosuperior TM quadrant rather than the malleus handle.
Factors Affecting Surgical Outcome (Cummings)
Dornhoffer and Gardner (study of 200 PORPs/TORPs, n=185 patients) identified independent negative predictors:
- Mucosal fibrosis in middle ear
- Revision ear surgery
- Absence of the malleus
- Removal of ear canal wall (open cavity)
Additional factors from Cummings:
| Factor | Impact |
|---|---|
| Status of middle ear mucosa | Thickened/infected mucosa → fibrosis → displaces prosthesis |
| Eustachian tube function | Poor ET function → reconstruction failure |
| Preoperative ABG | If ABG <30 dB, risk of worsening; approach with caution |
| Sensorineural level >30 dB | Results often unsatisfactory for unaided hearing goals |
| Open mastoid cavity | Elective ossiculoplasty often unsatisfying |
| TM integrity | Must be mobile, properly oriented |
| Intraoperative bleeding | Increases fibrosis risk |
| Cholesteatoma recurrence | Argue for staged approach |
Staging: Simultaneous vs. Delayed Ossiculoplasty
The decision to perform ossiculoplasty at the primary operation vs. a staged second look depends on:
- Status of middle ear mucosa — if thickened, infected, or bleeding, delay is prudent
- Cholesteatoma operations — some surgeons prefer to place a Silastic/Gelfilm spacer at the first operation to "set" the TM level on the promontory, then perform ossiculoplasty at the second stage when anatomy is stable and predictable
- Economic/access constraints — if a second-look is not feasible, simultaneous ossiculoplasty is justifiable, keeping in mind that cholesteatoma eradication always takes priority over hearing restoration
Results
| Prosthesis | ABG < 20 dB (Short-term) | 5-year Success (Yung & Vowler) |
|---|---|---|
| PORP | 50–85% | ~2/3 (66%) |
| TORP | 40–50% | ~1/3 (33%) |
Titanium PORP/TORP (Hess-Erga, long-term 5-year Kurz implant data):
- PORP: ABG <20 dB in 82% at 5 years
- TORP: ABG <20 dB in 63% at 5 years
- Extrusion rate: 5%
Titanium vs. non-titanium:
- A 2012 meta-analysis (Zhang et al., 12 studies, n=1388): no significant difference in stability or sound transmission
- The only RCT (94 patients, 24-month follow-up): no significant difference in extrusion rates or hearing gain
- A 2018 systematic review (14 studies): incus interposition and allograft PORPs produce similar hearing improvement (allograft PORP: 71% ABG closure; incus interposition: 64%)
- The severity of middle ear pathology has more influence on outcome than material choice
Important caveat: Long-term follow-up consistently shows significant progressive deterioration of hearing gain regardless of material used.
Complications
| Complication | Mechanism | Prosthesis |
|---|---|---|
| Extrusion | Direct TM-prosthesis contact | Both; commoner with TORP |
| Displacement/dislodgement | Short prosthesis; poor fixation | Both |
| Recurrent conductive loss | Fibrosis, adhesion, revision disease | Both |
| Stapes footplate fracture | Long TORP; excess pressure | TORP |
| Perilymph fistula | Footplate subluxation | TORP |
| TM erosion | Cartilage cap absent or thin | Both |
| Sensorineural hearing loss | Footplate injury, perilymph leak | TORP |
Prevention of extrusion: A cartilage interface equal to the diameter of the prosthesis head causes little effect on acoustic transmission (cadaver studies) while significantly preventing extrusion. Perichondrium is stripped from the prosthesis-contact surface and preserved on the TM-contact surface.
Role of Implantable Devices (Bone-Anchored and Middle Ear Implants)
For patients with mixed hearing loss and ABG >35 dB in whom ossiculoplasty is unlikely to give adequate unaided benefit, osseointegrated bone-conduction devices (BAHA, Ponto, Bonebridge) may outperform conventional hearing aids and provide near-complete ABG closure with minimal cochlear risk.
Key Points for PG Exam
- PORP = stapes superstructure present (stapes crura intact); TORP = stapes superstructure absent
- Both require a cartilage cap to prevent extrusion; cartilage equal in size to the prosthesis head does not impair acoustic transmission
- Titanium is the most widely used material — low mass, rigid, closest to native ossicle mass, MRI-compatible, user-friendly
- ABG <20 dB is the standard for surgical success
- Success rates: PORP > TORP (2:1 at 5 years by Yung & Vowler)
- Titanium vs. non-titanium: no significant difference in RCTs or meta-analyses — disease severity matters more than material
- Malleus absence is a major independent predictor of poor outcome
- Prosthesis must be placed perpendicular to the footplate (parallel piston motion)
- Long-term progressive hearing deterioration occurs regardless of material
- Austin–Kartush classification guides prosthesis selection intraoperatively
Source: Cummings Otolaryngology — Head and Neck Surgery, 7th Ed., Chapters 142 & 145 (pp. 2734–2735, 2772–2773)
Non titanium materials that can be used for torp and porp
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have all the material needed. Here is the focused answer:
Non-Titanium Materials for TORP and PORP in Ossiculoplasty
(Reference: Cummings Otolaryngology — Head and Neck Surgery, 7th Ed.; KJ Lee's Essential Otolaryngology)
Non-titanium materials fall into three broad categories: autografts, polymers, and ceramics. Each has distinct properties, historical context, and trade-offs.
I. Autografts
1. Autograft Ossicles (Incus / Malleus Head)
The incus (sculpted for interposition) was historically the gold standard before alloplastic materials were developed.
| Property | Detail |
|---|---|
| Material | Native incus or malleus head, sculpted intraoperatively |
| Advantages | Immediate availability, obvious biocompatibility, lowest extrusion rate, low cost, no foreign body reaction |
| Disadvantages | Risk of cholesteatoma recurrence (residual matrix in graft); requires time and surgical skill to sculpt; may be demineralized, eroded, or unusable; unsuitable in advanced disease |
| Use | Primarily as incus interposition (Type A defect: both malleus and stapes present) |
A 2018 systematic review (14 studies) found incus interposition and allograft PORPs yield similar hearing improvement, though allograft PORPs had slightly higher ABG closure rates (71% vs. 64%).
2. Autograft Cartilage
- Source: tragus (most common), conchal bowl, costal cartilage
- Not used as a primary PORP/TORP shaft, but as a sculpted strut in some reconstructions (Type A and B)
- Principal role: cartilage cap over any prosthesis head to prevent extrusion
II. Polymers
1. Polyethylene — Plastipore / Polycel (High-Density Polyethylene Sponge, HDPE)
Austin and Shea pioneered the use of early polyethylene and Teflon implants in the 1960s, marking the beginning of alloplastic ossiculoplasty.
| Property | Detail |
|---|---|
| Material | High-density polyethylene sponge |
| Trade names | Plastipore (Shea & Emmett), Polycel |
| Key feature | Porous structure — theorized to promote fibrous tissue ingrowth → better anchorage and biocompatibility |
| Advantages | Easy to trim/cut to appropriate length intraoperatively; lightweight; biocompatible |
| Disadvantages | High extrusion rate in early designs; hearing results did not match homografts; limited tissue bonding |
| Current use | Used as the shaft component in combination prostheses (e.g., HA platform + Plastipore shaft) |
Shea and Emmett introduced Proplast and Plastipore with the concept that porosity improves biocompatibility — but extrusion rates and hearing results with early designs did not match homografts.
2. PTFE — Teflon (Polytetrafluoroethylene)
| Property | Detail |
|---|---|
| Material | Polytetrafluoroethylene (PTFE) |
| Pioneers | Austin and Shea (early 1960s) |
| Advantages | Chemically inert, smooth surface, easy to handle |
| Disadvantages | Unacceptably high extrusion rate; poor tissue integration; largely abandoned for TORP/PORP shafts |
| Residual use | Still used in Teflon piston for stapedectomy (different context) |
3. Silicone Rubber
| Property | Detail |
|---|---|
| Material | Medical-grade silicone elastomer |
| Advantages | Flexible, biocompatible, easy to handle |
| Disadvantages | High extrusion rates; poor acoustic coupling due to dampening; largely replaced by ceramics and metals |
| Use | Occasionally as Silastic sheeting spacer in staged ossiculoplasty (to prevent adhesions), not as primary PORP/TORP shaft currently |
4. Proplast
- A composite porous polymer (PTFE + carbon) introduced alongside Plastipore
- Concept: porosity allows fibrous ingrowth
- Largely abandoned due to fragmentation and foreign body reactions over time
III. Ceramics
1. Hydroxyapatite (HA) — Calcium Phosphate Ceramic
The most clinically important non-titanium alloplastic material in current use.
| Property | Detail |
|---|---|
| Material | Ca₁₀(PO₄)₆(OH)₂ — calcium phosphate ceramic |
| Forms | Porous (Interpore) and dense |
| Key advantage | Osseointegration — achieves real bony integration without fibrous encapsulation; bonds directly to bone/tissue |
| Acoustic properties | Transmits sound well; theoretically excellent coupling to stapes |
| Disadvantages | Brittle; difficult to sculpt or modify intraoperatively; top-heavy designs tend to tilt; higher mass than titanium → increased acoustic impedance |
| Extrusion | Lower extrusion potential than early polymers |
| Comparison with titanium | No significant difference in hearing outcomes or stability (meta-analysis, Zhang et al., 12 studies, n=1388) |
2. Combination: HA Platform + Plastipore (or Polyethylene) Shaft
- IAPEX (KJ Lee): hydroxyapatite with polyethylene composite
- Rationale: exploits the bone-bonding capacity of HA at the platform (lateral end, near TM) while allowing easy length adjustment by cutting the Plastipore shaft
- HA platform → less extrusion, tissue bonding
- Plastipore shaft → easily trimmed to exact length needed
| Component | Material | Advantage |
|---|---|---|
| Head/platform (lateral) | Hydroxyapatite | Tissue bonding, low extrusion |
| Shaft (medial) | Plastipore / polyethylene | Easy to cut to length |
3. Bioglass (Bioactive Glass) — Ceravital
| Property | Detail |
|---|---|
| Material | Silicate-based bioactive glass ceramic |
| Trade names | Ceravital, Bioglass |
| Key feature | Bioactive — forms a bond with both bone and soft tissue through a hydroxyapatite surface layer |
| Advantages | Good biocompatibility; forms tight seal with tissues |
| Disadvantages | Brittle; limited availability; variable long-term results; largely replaced by titanium |
IV. Historical Evolution Summary
| Era | Material | Key Limitation |
|---|---|---|
| 1960s | Teflon, early polyethylene | Unacceptably high extrusion rate |
| 1970s–80s | Plastipore, Polycel, Proplast | Better biocompatibility but still high extrusion; results inferior to homografts |
| 1980s–90s | Hydroxyapatite, Bioglass | Good biocompatibility, osseointegration; but brittle, top-heavy |
| 1990s–2000s | HA + Plastipore composite (IAPEX) | Combined benefits; still limited by brittleness of HA |
| 2000s–present | Titanium (dominant) | Best overall profile; but no material is proven superior in RCTs |
V. Comparative Summary Table
| Material | Class | Extrusion Rate | Osseointegration | Ease of Use | Acoustic Damping | Status |
|---|---|---|---|---|---|---|
| Autograft incus | Autograft | Lowest | N/A | Requires sculpting | Negligible | Active (gold standard for interposition) |
| Polyethylene (Plastipore) | Polymer | High (early) | Fibrous ingrowth | Easy to trim | Low | Used as shaft in composites |
| Teflon (PTFE) | Polymer | Very high | None | Easy | Low | Abandoned for TORP/PORP |
| Silicone | Polymer | High | None | Easy | Moderate | Spacer use only |
| Hydroxyapatite | Ceramic | Low | True osseointegration | Difficult (brittle) | Low–moderate | Active |
| Bioglass / Ceravital | Ceramic | Moderate | Bioactive bonding | Difficult | Low | Largely replaced |
| HA + Plastipore (IAPEX) | Composite | Low | Partial | Moderate | Low | Active |
| Titanium | Metal | 5% (low) | None (MRI-safe) | Excellent | Lowest | Current standard |
VI. Key Exam Point
Despite the varied properties of all these materials, no alloplastic material has been shown to be significantly superior to another in large meta-analyses or RCTs:
- Zhang et al. meta-analysis (12 studies, n=1,388): no significant difference in stability or hearing outcomes between titanium and non-titanium prostheses
- The severity of middle ear pathology influences outcome more than material choice
- Cummings: "The numerous types of prostheses available attest to the fact that no one implant is perfect."
The ideal ossicular prosthesis (KJ Lee criteria) should be: lightweight, biocompatible, easy to trim and adjust, stable in the middle ear, and MRI-compatible — currently best approximated by titanium, but non-titanium materials (especially HA-based composites) remain clinically relevant.
Whatever material used if it is placed on stapes suprastructure is it called porp?
Yes — and this is an important conceptual point.
PORP and TORP are defined by their position in the middle ear (i.e., what the medial end rests on), not by the material they are made from.
The Defining Rule
| Name | Medial end rests on | Stapes superstructure status |
|---|---|---|
| PORP | Stapes capitulum (head) | Present |
| TORP | Stapes footplate | Absent |
So yes — whether the prosthesis is made of titanium, hydroxyapatite, Plastipore, autograft incus, or any other material — if its medial end sits on the stapes capitulum, it is called a PORP.
Why This Matters Clinically
The terminology describes the anatomical reconstruction pattern, not the material:
- PORP = the stapes superstructure (head + crura) is intact and used as the medial support → "partial" replacement because the lower part of the ossicular chain (stapes superstructure) is preserved
- TORP = the crura are gone, nothing remains above the footplate → prosthesis must span the full height from footplate to TM → "total" replacement
Confirming from Cummings
"A partial ossicular replacement prosthesis (PORP) is used when the stapes superstructure is present, and a total ossicular replacement prosthesis (TORP) is used when the superstructure is absent. Many variations [of material] exist..." — Cummings, Ch. 142
The classification is anatomical position, and material is a separate variable entirely. A sculpted autograft incus sitting on the stapes capitulum is functionally a PORP. A hydroxyapatite prosthesis on the footplate is a TORP. The name follows the anatomy.
This is a shared conversation. Sign in to Orris to start your own chat.