Chronic glumarulonephritis
Reading File
Finding Sources
Searching PubMed
"chronic glomerulonephritis"[MeSH Terms] AND management
Finding Sources
Searching PubMed
glomerulonephritis AND "chronic kidney disease"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
chronic glomerulonephritis histology pathology
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
chronic glomerulonephritis pathogenesis clinical features management 2024
Finding Sources
Reading File
Reading File
Finding Sources
I have sufficient information from authoritative textbooks to provide a comprehensive answer. Let me now synthesize everything into a well-organized response.
Chronic Glomerulonephritis
Definition & Overview
Chronic glomerulonephritis (CGN) is not a single disease entity but a final common pathway of diverse glomerular injuries leading to progressive, irreversible glomerular destruction, tubular atrophy, interstitial fibrosis, and ultimately end-stage kidney disease (ESKD). It represents a smoldering, insidious process unfolding over months to years, as opposed to the acute or subacute presentations of postinfectious GN or RPGN.
Etiology & Causes
CGN may arise from almost any primary or secondary glomerular disease. Common precursors include:
| Primary GN | Secondary GN |
|---|---|
| IgA nephropathy (most common worldwide) | Lupus nephritis (SLE) |
| Membranoproliferative GN (MPGN) | Diabetic nephropathy |
| Focal segmental glomerulosclerosis (FSGS) | Henoch-Schönlein purpura |
| Membranous nephropathy | Hepatitis B/C–associated GN |
| Post-infectious GN (minority of cases) | Cryoglobulinemia |
| ANCA-associated vasculitis | Amyloidosis |
In a minority of patients, CGN is discovered at advanced stages with no identifiable antecedent disease. A presumptive diagnosis is then made based on shrunken, scarred kidneys with hypertension and impaired renal function. — Brenner and Rector's The Kidney
Globally, IgA nephropathy is the leading cause; FSGS has become increasingly prevalent, especially in Africa and South Asia, while MPGN has declined in relative frequency.
Pathogenesis
The unifying mechanism is immunologically mediated glomerular injury:
- Immune complex deposition (most common) — circulating antigen-antibody complexes are deposited in the glomerular subendothelial, mesangial, or subepithelial space
- Complement activation — generates C3a and C5a (anaphylatoxins), recruiting neutrophils and monocytes
- Cytokine/growth factor release — TGF-β drives mesangial proliferation and fibrosis; HGF has reno-protective roles that are antagonized in CGN
- Podocyte injury — leads to protein leak and glomerulosclerosis
- Chronic inflammation → sclerosis → fibrosis — sclerosis occurs within the glomeruli, and fibrosis in the tubulointerstitial compartment, reducing nephron mass
Key mediators: TGF-β, PDGF, angiotensin II, endothelin-1 drive progressive glomerulosclerosis and tubulointerstitial fibrosis.
Morphology (Pathology)
Gross Appearance
- Bilaterally shrunken, contracted kidneys with finely granular ("leather-grain") cortical surfaces — this fine, symmetric scarring distinguishes CGN from chronic pyelonephritis (which produces asymmetric, coarse scarring)
- Cortex is thinned; corticomedullary junction is indistinct
Microscopy (Light Microscopy)
- Global glomerulosclerosis — obliteration of glomerular capillaries by fibrous or hyaline material
- Hyalinization of glomerular tufts (replacement by acellular eosinophilic material)
- Tubular atrophy — tubules shrink, with thickened basement membranes
- Interstitial fibrosis with lymphocytic infiltrate
- Vascular changes — hyaline arteriolosclerosis, intimal thickening of arteries
Urinary Sediment ("Telescoped Sediment")
A hallmark of CGN is the "telescoped sediment" — the simultaneous presence of:
- Dysmorphic RBCs and RBC casts (glomerular injury)
- Granular and waxy casts (tubular atrophy)
- Broad casts (indicating dilated, atrophic tubules)
- Heavy proteinuria on dipstick
"With some forms of chronic glomerulonephritis, a 'telescoped' sediment is observed… the presence of the elements of a glomerulonephritis sediment together with waxy or broad casts, the latter indicative of tubular atrophy." — National Kidney Foundation Primer on Kidney Diseases, 8e
Clinical Features
CGN often follows an insidious course. Presentations include:
Asymptomatic Phase
- Detected incidentally: microscopic hematuria, proteinuria, mildly elevated creatinine
- May persist for years
Symptomatic Phase
| Feature | Details |
|---|---|
| Hypertension | Develops early, often severe; may be the presenting complaint |
| Proteinuria | Variable; heavy proteinuria indicates poor prognosis |
| Hematuria | Micro or macroscopic; dysmorphic RBCs on microscopy |
| Edema | Periorbital, dependent; worsens with nephrotic-range proteinuria |
| Oliguria/azotemia | As GFR declines |
| Fatigue, nausea | Uremic symptoms in advanced disease |
Advanced/End-Stage Features
- Uremia: anorexia, vomiting, encephalopathy, pericarditis
- Anemia of CKD (reduced EPO)
- Renal osteodystrophy (secondary hyperparathyroidism)
- Bilateral small kidneys on imaging
Four Presentations of Glomerulonephritis (Classification)
- Acute GN — sudden onset, usually reversible (e.g., post-streptococcal)
- Rapidly progressive GN (RPGN/Crescentic) — weeks to months, crescents on biopsy
- Recurrent macroscopic hematuria — episodic (classic IgA nephropathy)
- Chronic GN — slow progression over years to ESKD
Investigations
Urine
- Dipstick: protein, blood
- Microscopy: dysmorphic RBCs, RBC casts, granular/waxy/broad casts
- 24-hr urine protein or spot PCR
Blood
- Serum creatinine, BUN, eGFR
- Electrolytes (↑K⁺, ↑phosphate, ↓calcium in advanced CKD)
- Serum albumin (↓ if nephrotic)
- C3 and C4 — C3 low in post-infectious GN, MPGN, lupus nephritis; normal in IgA nephropathy
- ANA, anti-dsDNA (SLE)
- ANCA (p-ANCA, c-ANCA for vasculitis)
- Anti-GBM antibodies (Goodpasture)
- Hepatitis B/C serology
- Cryoglobulins, serum protein electrophoresis
- ASO titre, anti-DNase B (post-streptococcal GN)
Imaging
- Renal ultrasound: small, echogenic, contracted kidneys bilaterally (late CGN)
Renal Biopsy
- Essential for definitive diagnosis and management
- Identifies the specific glomerular lesion, determines activity vs. chronicity
- Guides immunosuppressive therapy decisions
- Harrison's (2025): "Increasing appreciation that patients with IgAN have a more rapid GFR decline to end-stage kidney disease has encouraged greater use of renal pathology to guide a more aggressive management strategy."
Management
General / Conservative Measures
| Intervention | Goal |
|---|---|
| ACE inhibitors or ARBs | First-line; reduce proteinuria, slow progression, control BP (target <130/80 mmHg) |
| Dietary protein restriction | 0.6–0.8 g/kg/day in advanced CKD to reduce hyperfiltration |
| Salt restriction | Control hypertension and edema |
| Lipid-lowering (statins) | Reduce cardiovascular risk (leading cause of death in CKD) |
| Avoid nephrotoxins | NSAIDs, aminoglycosides, IV contrast (use with caution) |
| Treat infections | Especially in infection-related GN |
Disease-Specific Immunotherapy
| Disease | Treatment |
|---|---|
| IgA nephropathy | ACEi/ARB; corticosteroids if progressive; complement blockers (budesonide, sparsentan, avacopan); rituximab |
| Lupus nephritis | Hydroxychloroquine ± mycophenolate mofetil ± steroids; belimumab |
| ANCA vasculitis | Rituximab or cyclophosphamide + steroids; avacopan |
| Anti-GBM disease | Plasmapheresis + cyclophosphamide + steroids |
| Membranous nephropathy | Rituximab (first-line); cyclophosphamide + steroids |
| Minimal change / FSGS | Corticosteroids; calcineurin inhibitors |
Recent advance: The FDA approved sparsentan (dual endothelin-1 and angiotensin II receptor antagonist) for adults with primary IgA nephropathy at high risk of progression (urine PCR >1.5 g/g with decreased GFR). — Harrison's 22E (2025)
Renal Replacement Therapy
When ESKD is reached:
- Hemodialysis
- Peritoneal dialysis
- Kidney transplantation (treatment of choice where feasible)
Prognosis
Prognosis varies by underlying cause and the degree of proteinuria/hypertension at presentation:
| Factor | Unfavorable Prognosis |
|---|---|
| Proteinuria | >1–3 g/day persistently |
| GFR at presentation | Significantly impaired |
| Hypertension | Poorly controlled |
| Histology | >50% globally sclerotic glomeruli, severe interstitial fibrosis |
| Genetics | High-risk APOL1 alleles (African ancestry, rapid FSGS/IgAN progression) |
"Prolonged and persistent heavy proteinuria and abnormal GFR mark patients with an unfavorable prognosis." — Robbins Pathologic Basis of Disease
In women with CGN and normal renal function at baseline, a 30-year study found no significant difference in progression to ESKD between those who became pregnant vs. those who did not — provided blood pressure is well controlled and proteinuria is minimal (<1 g/24 hr). — Creasy & Resnik's Maternal-Fetal Medicine
Histology Image
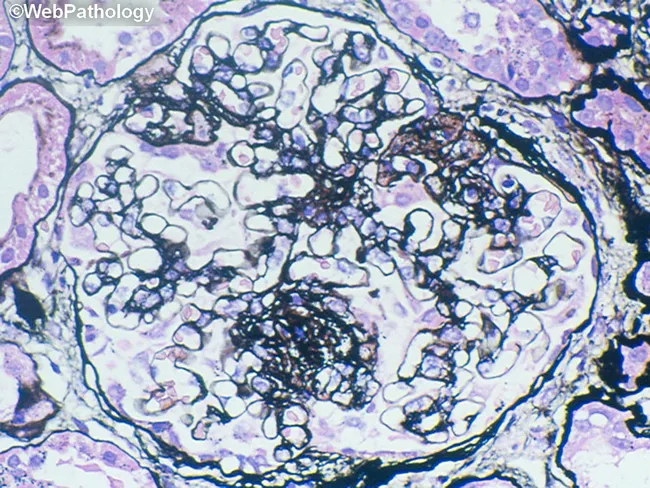
Light microscopy showing glomerular pathology with mesangial expansion and basement membrane thickening, characteristic of chronic immune-mediated glomerulonephritis.
Key Sources
- Harrison's Principles of Internal Medicine, 22e (2025), Ch. 319
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Brenner and Rector's The Kidney, 2-Volume Set
- National Kidney Foundation Primer on Kidney Diseases, 8e
- Tintinalli's Emergency Medicine, 9e
- Comprehensive Clinical Nephrology, 7e
- KDIGO 2021 Clinical Practice Guideline for Glomerular Diseases (updated 2024 for lupus nephritis)
This is a shared conversation. Sign in to Orris to start your own chat.