Iron and its disorders, NAC in pediatrics, detail explanation, in simple language - mbbs final year , pedia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have all the material needed for a thorough, exam-oriented answer. Let me write it up.
Iron and Its Disorders + NAC in Pediatrics
MBBS Final Year - Pediatrics Focus
PART 1: IRON METABOLISM
What is Iron and Why Does the Body Need It?
Iron is one of the most important minerals in the body. Total body iron = 4-5 grams.
| Iron Pool | Form | Amount |
|---|---|---|
| Hemoglobin | Functional | ~65% |
| Myoglobin | Functional | ~4% |
| Enzymes (cytochromes, peroxidase, catalase) | Functional | ~1% |
| Transferrin (transport, plasma) | Transport | ~0.1% |
| Ferritin + Hemosiderin (liver, RES) | Storage | 15-30% |
Think of it simply: most iron is working (in Hb), a small bit is travelling (on transferrin), and the rest is stored (as ferritin).
Iron Metabolism Pathway
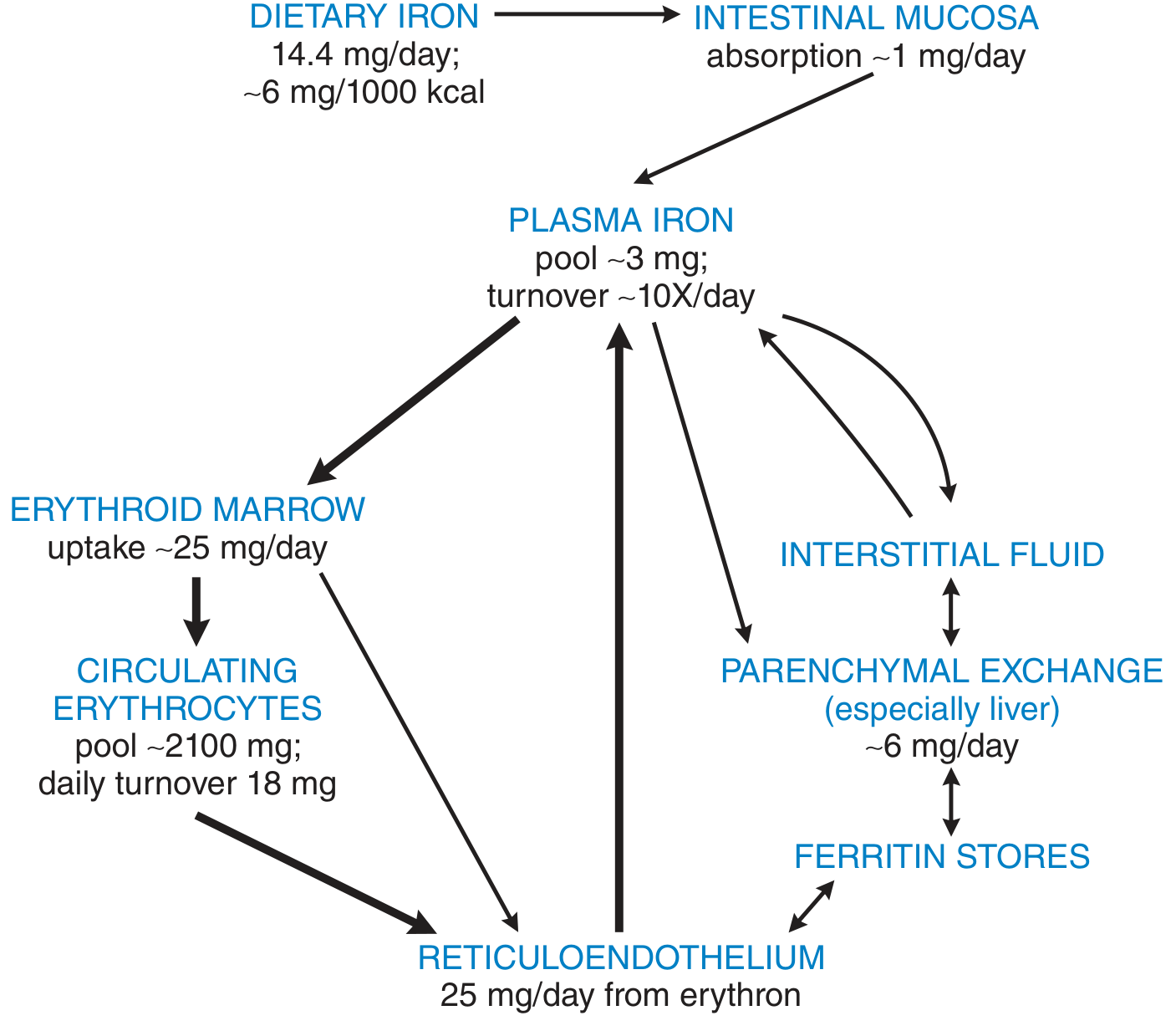
Iron metabolism flow - Goodman & Gilman's Pharmacological Basis of Therapeutics
Step-by-step in simple terms:
-
Absorption: Dietary iron (~14 mg/day eaten; only ~1 mg absorbed) enters through intestinal mucosa. Ferrous (Fe2+) is absorbed 3x better than ferric (Fe3+). Heme iron (from meat) is absorbed much better than non-heme iron.
- Enhancers: Vitamin C (ascorbic acid), meat/fish
- Inhibitors: Phytates (wheat bran), phosphates, tannins (tea), calcium
-
Transport in blood: Absorbed iron binds to apotransferrin → forms transferrin (a beta-globulin, 76 kDa glycoprotein) in plasma. Transferrin carries iron to where it's needed.
-
Delivery to marrow: Transferrin binds to transferrin receptors on erythroblasts → endocytosed → iron released inside the cell → goes to mitochondria → heme is synthesized.
-
Storage: Excess iron stored as:
- Ferritin - soluble, dispersed form (apoferritin shell + Fe inside; up to 4000 iron atoms per molecule)
- Hemosiderin - insoluble aggregate, visible under light microscope (seen in overload states)
-
Recycling: After ~120 days, old RBCs are destroyed by macrophages → iron released → stored as ferritin → recycled back to plasma. ~25 mg/day recycled this way (far more than the 1 mg absorbed daily).
-
Loss: Men lose ~0.6 mg/day (mostly in feces). Women lose ~1.3 mg/day (includes menstrual loss).
Iron Regulation - The Hepcidin Master Switch
Hepcidin (made by liver) is the key regulator:
- Iron overload / inflammation → hepcidin ↑ → blocks ferroportin → less iron exported from intestinal cells and macrophages → less iron in blood
- Iron deficiency / anemia / hypoxia → hepcidin ↓ → more iron released
IRPs (Iron Regulatory Proteins) control ferritin and transferrin receptor synthesis at the cellular level - when iron is low, cells make more transferrin receptors and less ferritin.
PART 2: IRON REQUIREMENTS IN PEDIATRICS
This is high-yield for finals!
| Age Group | Iron Requirement (µg/kg/day) |
|---|---|
| Infant | 67 (highest per kg - rapid growth!) |
| Child | 22 |
| Adolescent male | 21 |
| Adolescent female | 20 |
| Pregnant (2nd-3rd trimester) | 80 (very high!) |
Key exam point: Infants have a safety factor of 0.5-1 (barely meeting needs). If on a poor diet, infants are the most at-risk group.
PART 3: IRON DEFICIENCY ANEMIA (IDA)
Who Gets It?
- Children 6-24 months - Most vulnerable. Birth iron stores are exhausted after 4-6 months.
- Adolescent girls - Menstrual loss + rapid growth + poor diet
- Premature/low birth weight infants - Less iron stored before birth
- "Milk anemia" of infancy - Baby on only milk + carbs, no iron-containing foods
Why cow's milk is dangerous before 12 months: Causes intestinal blood loss (protein intolerance) + has very low iron content.
Pathophysiology - Three Stages
The body loses iron in sequence - think of it as emptying a bucket:
Stage 1: Iron Depletion
- Iron stores (ferritin) ↓
- Plasma ferritin ↓, TIBC (transferrin) ↑
- No anemia yet, Hb still normal
Stage 2: Iron-Deficient Erythropoiesis
- Serum iron ↓, transferrin saturation <15%
- RBC protoporphyrin ↑ (iron needed for heme synthesis, isn't there)
- Anemia mild or absent
- RBCs still normal size
Stage 3: IDA (frank anemia)
- Hb low, RBCs microcytic + hypochromic
- All the above abnormalities present
Clinical Features
General anemia symptoms:
- Pallor (especially conjunctival, palmar, nail bed)
- Fatigue, irritability
- Tachycardia, flow murmur
Iron-deficiency specific signs (iron in tissues):
- Pica - eating ice, dirt, clay (especially children)
- Koilonychia - spoon-shaped nails
- Angular stomatitis - fissures at mouth corners
- Glossitis - smooth, sore tongue
- Dysphagia - Plummer-Vinson syndrome (glossitis + koilonychia + dysphagia = this triad)
- Restless leg syndrome
- Developmental delay / poor school performance in children - iron deficiency in early childhood can cause irreversible cognitive delay
Lab Features
| Test | IDA |
|---|---|
| Hb | ↓ |
| MCV | ↓ (microcytic) |
| MCH/MCHC | ↓ (hypochromic) |
| RDW | ↑ (anisocytosis) |
| Serum Iron | ↓ |
| TIBC | ↑ |
| Transferrin saturation | ↓ (<15%) |
| Serum Ferritin | ↓ (first to fall) |
| Reticulocyte count | ↓ (before treatment) |
| Bone marrow Prussian blue stain | No stainable iron |
Blood film shows: microcytic, hypochromic RBCs, pencil cells (hypochromic elliptocytes), anisocytosis, poikilocytosis.
Treatment of IDA
Oral Iron (first choice):
- Ferrous sulfate - cheapest, most effective (ferrous salts absorbed 3x better than ferric)
- Pediatric dose: 3-6 mg/kg/day of elemental iron in 2-3 divided doses
- Adult: 150-200 mg elemental iron/day (e.g., ferrous sulfate 325 mg TDS)
- Give on empty stomach or with Vitamin C
- Response: Reticulocytosis in 4-7 days, Hb rise of ≥2 g/dL by 4 weeks = good response
- Continue for 3 months after Hb normalizes to replenish stores
Side effects of oral iron: Nausea, heartburn, constipation, black stools (tell parents!), abdominal discomfort. Start low and go up.
IV/Parenteral Iron - when oral fails, malabsorption, ongoing losses, non-compliance:
- Ferric carboxymaltose, iron sucrose, iron dextran
Blood transfusion - only if Hb very low (<5 g/dL) with symptoms, or before urgent surgery.
PART 4: IRON OVERLOAD / POISONING
Iron Poisoning in Children (Pediatric Emergency!)
Accidental iron tablet ingestion is a leading cause of toxic death in young children. As few as 20 mg/kg of elemental iron can cause toxicity; >60 mg/kg is potentially fatal.
4 Stages of Iron Poisoning:
| Stage | Time | Features |
|---|---|---|
| Stage 1 | 0-6 hours | Vomiting, diarrhea, hematemesis, abdominal pain (direct GI toxicity) |
| Stage 2 | 6-24 hours | Apparent improvement (deceptive "quiet phase") |
| Stage 3 | 12-48 hours | Shock, metabolic acidosis, liver failure, coagulopathy, CNS toxicity |
| Stage 4 | 2-6 weeks | GI scarring, pyloric stenosis, bowel obstruction |
Why is free iron toxic? When transferrin is fully saturated, free iron (NTBI = non-transferrin-bound iron) circulates → catalyzes free radical production (Fenton reaction) → oxidative damage to GI, liver, heart, brain.
Treatment of iron poisoning:
- Supportive care (IV fluids, correct acidosis)
- Deferoxamine - specific chelator for iron overload/poisoning. Binds free iron → forms ferrioxamine → excreted in urine (urine turns "vin rose" / reddish-brown color = sign it's working)
- Whole bowel irrigation if large ingestion
Hereditary Hemochromatosis
- Genetic iron overload (usually HFE gene mutation, autosomal recessive)
- Excess iron deposits in liver, heart, pancreas, joints, gonads
- "Bronze diabetes" - skin pigmentation + diabetes + cirrhosis
- Treatment: Phlebotomy (removing blood) is the mainstay
PART 5: NAC (N-ACETYLCYSTEINE) IN PEDIATRICS
What is NAC?
NAC is the antidote for paracetamol (acetaminophen/APAP) poisoning - the most common drug overdose presenting to pediatric emergency. It is also used as a mucolytic.
Why is Paracetamol Toxic?
In normal doses, paracetamol is safely metabolized by:
- Glucuronidation (~55%)
- Sulfation (~30%)
- Only ~5% goes through CYP2E1 → makes NAPQI (toxic metabolite), immediately detoxified by glutathione
In overdose, glucuronidation and sulfation get overwhelmed → more and more goes through CYP2E1 → NAPQI accumulates → glutathione stores depleted → NAPQI binds to liver cell proteins → hepatocellular necrosis
How does NAC work?
NAC works by three mechanisms:
- Replenishes glutathione - NAC is converted to cysteine → used to synthesize new glutathione → NAPQI is neutralized
- Directly detoxifies NAPQI - acts as a sulfhydryl donor
- Counteracts oxidative stress caused by NAPQI
The golden window: NAC is most effective within 8 hours of ingestion. Still useful beyond 8-16 hours but less hepatoprotective effect.
Dosing of NAC (High-Yield!)
| Route | Loading Dose | Maintenance |
|---|---|---|
| Oral | 140 mg/kg | 70 mg/kg q4h × 17 doses (72 hours total) |
| IV (FDA) | 150 mg/kg over 1 hour | 12.5 mg/kg/h × 4h, then 6.25 mg/kg/h × 16h |
| IV (one-bag method) | 150 mg/kg over 1 hour | 12.5 mg/kg/h × 20 hours |
Note: Same weight-based doses apply in children (per kg dosing). IV is preferred in pediatrics because the sulfur taste of oral NAC causes vomiting in children.
When to Give NAC?
- Paracetamol level plots above treatment line on the Rumack-Matthew nomogram (level drawn at ≥4 hours post-ingestion)
- If level cannot be obtained within 8 hours of ingestion → start empirically, stop if level is non-toxic
- Staggered/unknown time overdose → start NAC (safety first)
- Acute liver failure from APAP → continue NAC even if level undetectable (hepatoprotective mechanism beyond glutathione replenishment)
Side Effects of IV NAC (Anaphylactoid Reactions)
These are not true allergies - they are rate-related reactions:
- Flushing, pruritus, urticaria, nausea/vomiting
- Occasionally: bronchospasm, hypotension
- Management: Slow the infusion rate, give antihistamines/antiemetics; rarely need to stop
Minor interference with PT/INR assay - an elevated INR during NAC therapy does not mean liver failure unless INR >2.0.
When to Stop IV NAC?
Stop after the 21-hour protocol is complete IF:
- AST <50% of peak value, AND
- INR <2.0, AND
- Clinical improvement (no encephalopathy)
Otherwise continue until liver function recovers.
NAC as Mucolytic in Pediatrics
- NAC splits disulfide bonds of mucoproteins → reduces sputum viscosity
- Used in:
- Cystic fibrosis
- Bronchiectasis
- Chronic suppurative lung disease
- Meconium ileus equivalent (oral high dose)
- Given by nebulization or orally
QUICK EXAM SUMMARY TABLE
| Topic | Key Points |
|---|---|
| Most common age for IDA | 6-24 months |
| First lab to fall in IDA | Serum ferritin |
| Blood film in IDA | Microcytic, hypochromic, pencil cells, anisocytosis |
| Oral iron dose (peds) | 3-6 mg/kg/day elemental iron |
| Response monitoring | Reticulocytosis at 4-7 days; Hb +2 g/dL at 4 weeks |
| NAC antidote for | Paracetamol (APAP) poisoning |
| NAC mechanism | Replenishes glutathione, detoxifies NAPQI |
| Best window for NAC | Within 8 hours of ingestion |
| IV NAC loading | 150 mg/kg over 1 hour |
| Oral NAC loading | 140 mg/kg |
| Side effect of IV NAC | Anaphylactoid reaction (rate-related, not true allergy) |
| Iron poisoning antidote | Deferoxamine |
| Deceptive stage in iron poisoning | Stage 2 (6-24h) - "quiet phase" |
| Plummer-Vinson triad | Glossitis + koilonychia + dysphagia |
| Pica | Eating non-food (dirt, ice) - seen in IDA |
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Guyton and Hall Medical Physiology; Henry's Clinical Diagnosis and Management by Laboratory Methods; The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.