Major histocompatibility complex (MHC) and antigen presentation, endogenous and exogenous antigen processing pathways. Role of Human leucocyte antigens (HLA) in susceptibility and pathogenesis of rheumatic diseases. Add a note on HLA typing. Detailed notes From rheumatology textbooks and journals
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
HLA MHC antigen presentation rheumatic disease
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple rheumatology and immunology textbooks. Let me compile the detailed notes.
MHC, Antigen Presentation, HLA, and Rheumatic Diseases - Detailed Notes
Part 1: Major Histocompatibility Complex (MHC) - Structure and Organization
Overview
The MHC is a cluster of genes on chromosome 6p21.3 that encodes cell-surface proteins critical to adaptive immune responses. In humans, these proteins are called Human Leukocyte Antigens (HLA). The HLA locus contains more than 200 genes organized into three classes:
Class I genes: HLA-A, HLA-B, HLA-C - present on virtually all nucleated cells
Class II genes: HLA-DP, HLA-DQ, HLA-DR - present primarily on antigen-presenting cells (APCs) - dendritic cells, macrophages, B lymphocytes
Class III genes: Complement components (C2, C4, Factor B), cytokines (TNF-alpha), heat shock proteins - immunologically relevant but not directly involved in antigen presentation
Class II genes: HLA-DP, HLA-DQ, HLA-DR - present primarily on antigen-presenting cells (APCs) - dendritic cells, macrophages, B lymphocytes
Class III genes: Complement components (C2, C4, Factor B), cytokines (TNF-alpha), heat shock proteins - immunologically relevant but not directly involved in antigen presentation
"The HLA locus consists of more than 200 genes that encode cell surface proteins involved in presenting intracellular antigens to the immune system." - Tietz Textbook of Laboratory Medicine, 7th Edition
Molecular Structure
MHC Class I consists of an alpha (heavy) chain non-covalently associated with beta-2 microglobulin (not MHC-encoded). The alpha chain has three domains: alpha-1 and alpha-2 form the peptide-binding groove; alpha-3 interacts with CD8 on cytotoxic T cells. Class I binds peptides of 8-10 amino acids (anchor at both ends, groove closed).
MHC Class II consists of two chains, alpha and beta, both MHC-encoded. The alpha-1 and beta-1 domains form the peptide-binding groove, which is open at both ends and accommodates peptides of 15-24 amino acids (binding register of ~9 amino acids, flanking residues extend beyond the groove). Class II engages CD4 on helper T cells via the beta-2 domain.
"Unlike class I, the class II groove is open at both ends and therefore can bind longer peptides, typically about 15-20 amino acids long. However, just as for class I, it is a stretch of about 9 amino acids that are directly involved in the interaction." - Roitt's Essential Immunology
HLA Polymorphism
The HLA system is the most polymorphic genetic system known in humans. Over 3,000 HLA-B alleles alone have been recognized by the WHO. This extraordinary diversity:
- Protects species from microbial molecular mimicry
- Maintains diversity of antigenic recognition in the lymphoid system
- Ensures heterozygosity (hybrid vigor)
Each allele is named by gene designation + up to 4 sets of digits (e.g., HLA-DRB1*0401), where the first two digits indicate the allele group (serological type) and subsequent digits denote specific allele variants.
Part 2: Antigen Processing and Presentation Pathways
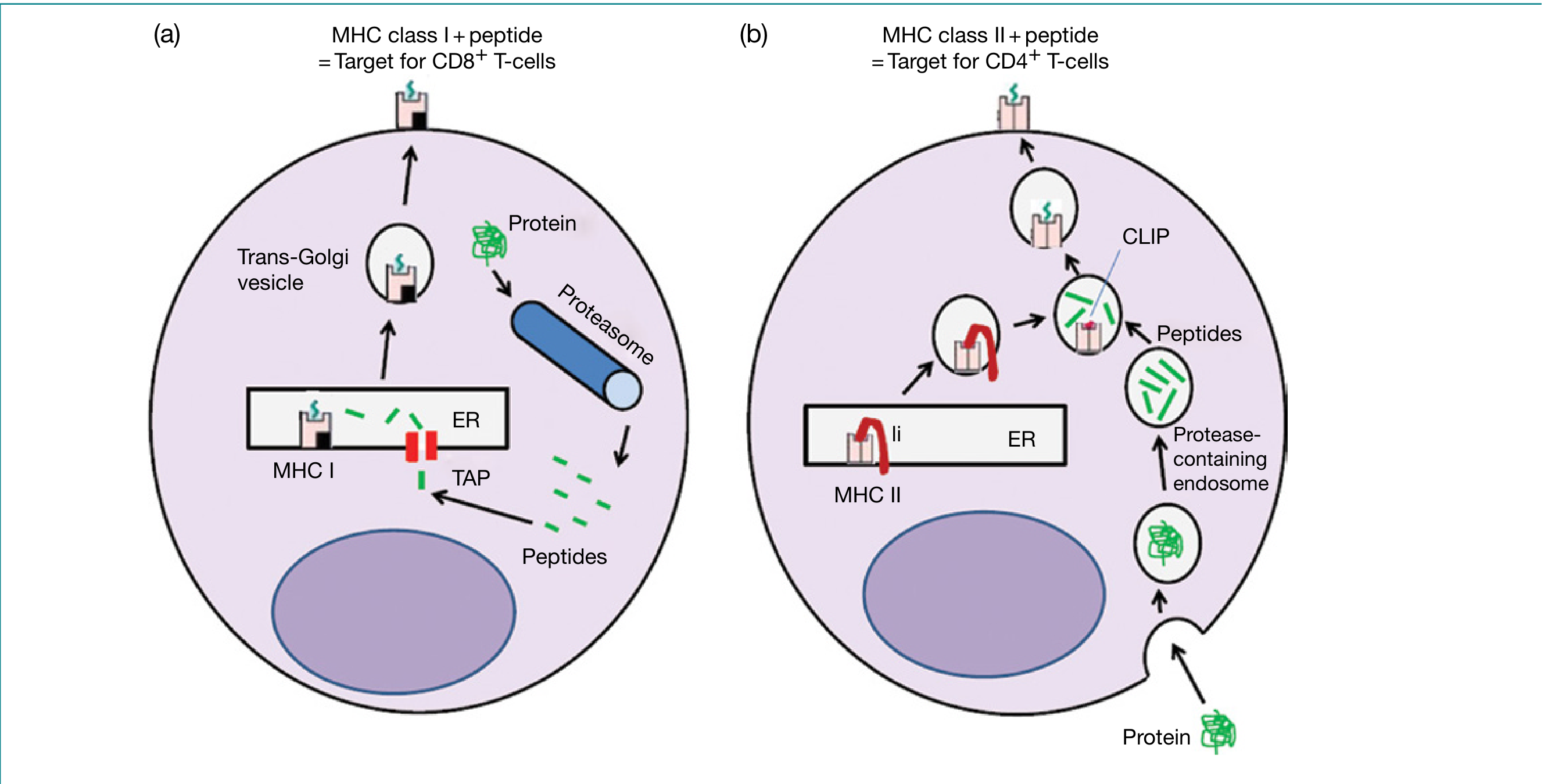
A. Endogenous Antigen Processing Pathway (MHC Class I)
This pathway handles proteins synthesized within the cell - viral proteins, tumor antigens, and normal self-proteins.
Steps:
-
Protein ubiquitination: Intracytoplasmic proteins (viral, tumor, normal self-proteins) are tagged with multiple ubiquitin molecules in an ATP-dependent reaction. Misfolded/disassembled proteins from the ER (via ER-associated protein degradation, ERAD) and mitochondrial-derived proteins can also enter this pathway.
-
Proteasomal degradation: Polyubiquitinated proteins are directed to the 26S proteasome, which cleaves them into peptide fragments. The standard (housekeeping) proteasome generates mostly fragments that are too short or too long for MHC class I binding.
-
Immunoproteasome: IFN-gamma induces replacement of three standard catalytic subunits (beta-1, beta-2, beta-5) with immunoproteasome-specific subunits (beta-1i/LMP2, beta-2i/MECL-1, beta-5i/LMP7), encoded within the MHC. This "immunoproteasome" has modified cleavage specificity that greatly increases the proportion of 8-10 amino acid peptides optimal for MHC class I binding.
-
TAP transport: Peptide fragments are translocated from the cytosol into the endoplasmic reticulum (ER) lumen by the TAP1/TAP2 heterodimer (Transporters associated with Antigen Processing), ABC transporter proteins also encoded within the MHC. Peptides slightly too long undergo further trimming by ER-resident aminopeptidases ERAP-1 and ERAP-2 in humans (ERAAP in mice). Notably, ERAP1 variants are associated with ankylosing spondylitis, highlighting the role of peptide trimming in disease pathogenesis.
-
MHC class I assembly: In the ER, newly synthesized MHC class I heavy chains associate with beta-2 microglobulin and the chaperone calnexin (prior to beta-2m association) and then calreticulin + ERp57 (after). The peptide loading complex (calreticulin, ERp57, tapasin) stabilizes the empty groove and facilitates optimal peptide loading. Tapasin bridges TAP and the MHC class I molecule.
-
Surface transport: The stable MHC class I-peptide complex is transported via the trans-Golgi network to the cell surface.
-
T-cell recognition: CD8+ cytotoxic T lymphocytes recognize the MHC class I-peptide complex via their TCR. The peptide occupies the groove with anchor residues pointing into the groove pockets and a minority of side-chains (17-27% solvent accessibility) pointing toward the TCR.
Key point: About 75% of class I natural ligands are self-peptides from cytosolic proteins (histones, heat-shock proteins, enzymes) at 100-400 copies per cell. Proteins expressed in unusual abundance (viral antigens, oncofetal proteins) are readily detected by resting T cells.
B. Exogenous Antigen Processing Pathway (MHC Class II)
This pathway handles proteins taken up from outside the cell by endocytosis or phagocytosis.
Steps:
-
Endocytosis/Phagocytosis: Extracellular antigens (bacteria, soluble proteins, immune complexes) are internalized into endosomes/phagosomes.
-
Endosomal/lysosomal degradation: The endocytic vesicles progressively acidify and acquire proteases (cathepsins B, D, S, L). These degrade the ingested proteins into peptide fragments within protease-containing endosomes/lysosomes.
-
MHC class II synthesis with invariant chain (Ii): Newly synthesized MHC class II alpha-beta heterodimers in the ER associate with the invariant chain (Ii). The Ii serves two functions:
- Its CLIP (Class II-associated Invariant chain Peptide) segment acts as a "molecular stopper," sitting in the peptide-binding groove and preventing premature peptide loading by ER-resident peptides (which would otherwise compete with class I).
- The Ii contains targeting signals that direct the MHC class II-Ii complex away from the secretory pathway toward the endocytic compartments.
-
MIIC formation and CLIP exchange: The MHC class II-Ii complex is transported to specialized late endosomal compartments called MIIC (MHC class II compartments). Here, Ii is progressively degraded by lysosomal proteases, leaving only the CLIP fragment in the groove. The non-classical MHC class II molecule HLA-DM (encoded within the MHC) then catalyzes the exchange of CLIP for high-affinity antigenic peptides. HLA-DO modulates HLA-DM activity in B cells.
-
Peptide loading and surface expression: Antigenic peptides generated in endosomes compete for binding to MHC class II. The class II-peptide complex is then transported to the cell surface.
-
T-cell recognition: CD4+ helper T lymphocytes recognize MHC class II-peptide complexes. Class II-bound peptides extend from both ends of the open groove with greater solvent accessibility (35%) and more side-chains pointing toward the TCR.
C. Cross-Presentation Pathway
Dendritic cells uniquely can present exogenous antigens via MHC class I to CD8+ T cells - a process called cross-presentation. This is essential for priming cytotoxic T cell responses against extracellular pathogens and tumor antigens.
D. CD1 Pathway
Lipid antigens and glycolipids are presented by CD1 molecules (non-classical MHC class I-like), which are important in mycobacterial immunity and NKT cell activation.
Part 3: Role of HLA in Susceptibility and Pathogenesis of Rheumatic Diseases
General Principles
HLA molecules directly govern which peptide antigens are presented to T cells and, consequently, which T cell clones are selected or deleted during thymic education and which self-reactive T cells remain in the periphery. The extraordinary polymorphism of HLA means that different individuals present different peptide repertoires to their immune systems, explaining why HLA alleles are among the strongest genetic risk factors for autoimmune diseases.
Three major mechanisms are proposed:
-
Arthritogenic peptide hypothesis: Specific HLA alleles present self-peptides (autoantigens) to autoreactive T cells, driving pathological autoimmune responses.
-
Thymic selection hypothesis: HLA alleles shape the TCR repertoire during thymic development, selecting for (or failing to delete) autoreactive T cell clones.
-
Molecular mimicry: Structural similarities between the HLA-peptide complex and microbial antigens may trigger cross-reactive immune responses.
3A. Rheumatoid Arthritis (RA)
HLA-DRB1 and the Shared Epitope (SE)
The association of RA with HLA was first reported by Stastny in the 1970s using cellular and antibody reagents. The DRB1*0401 allele (originally the "Dw4" type) was the first to be associated with RA in White populations.
The key genetic risk alleles at the DRB1 locus are:
- DRB1*0401, *0404, *0405 (DR4 subtypes) - strongest risk in White/North European populations
- DRB1*0101 (DR1) - risk in some ethnic groups; lower relative risk than DR4
- DRB1*1001 (DR10) - risk in Southern European and some Middle Eastern populations
- DRB1*0901 - risk allele in Asians
Most of these alleles share a common amino acid sequence at positions 70-74 of the DRB1 chain: Q/K-R-R-A-A, located on the alpha-helical portion of the peptide-binding groove. This is the Shared Epitope (SE), a term coined by Gregersen et al. in 1987. The SE region:
- Influences the shape of the antigen-binding groove (positions 70-74)
- May determine which peptides are bound and presented to T cells
- Is positioned where it can interact with both incoming peptides and TCR
"Most of these risk alleles share a common sequence: Q or K-R-R-A-A, which has been termed the shared epitope (SE). This structural feature is located on the α-helical portion of the DR β chain in a position where it may influence both peptide binding and T cell receptor interactions with the DRB1 molecule." - Firestein & Kelley's Textbook of Rheumatology
Relative Risks (DRB1 Genotypes for RA):
| DRB1 Genotype | Relative Risk | P Value |
|---|---|---|
| 0101/DRX | 2.3 | 10^-3 |
| 0401/DRX | 4.7 | 10^-11 |
| 0404/DRX | 5.0 | 10^-9 |
| 0101/0401 | 6.4 | 10^-4 |
| 0401/0404 | 31.3 | 10^-32 |
The combination of DRB1*0401/*0404 carries an OR of >30 - a dramatic gene-dosage effect.
Refinement of the SE hypothesis (modern understanding):
Massively parallel genotyping with bioinformatics has refined the key positions: an amino acid at position 11 or 13 (within the peptide-binding groove but outside the classic SE motif) is the most associated with RA susceptibility, followed by positions 71 and 74 (within the SE). Additionally, amino acids in HLA-B (position 9) and HLA-DPB1 (position 9) show independent association. Together, five amino acids in three HLA proteins (DRB1, B, DPB1) explain almost all HLA-region associations with RA.
SE and ACPA: The SE alleles associate most strongly with anti-citrullinated protein antibody (ACPA)-positive RA. Citrullinated peptides (generated by PAD enzymes in the inflamed joint) have particular affinity for DRB1*0401 alleles, supporting the arthritogenic peptide hypothesis. Smoking upregulates PAD enzymes and promotes citrullination - explaining the gene-environment interaction between SE and smoking in ACPA-positive RA.
Protective alleles: DRB1*01:03 and certain other alleles are associated with protection against RA.
Non-HLA genes: GWAS has identified >120 confirmed RA susceptibility loci, including:
- PTPN22 (R620W variant) - disrupts Csk-mediated inhibition of Lck, leading to TCR signaling threshold lowering
- STAT4, CTLA4, PADI4, TRAF1-C5, PTPRC, CD40, and many others
- Heritability of RA ~65%; HLA-DRB1 contributes approximately 30-50% of genetic risk
3B. Ankylosing Spondylitis (AS) and Spondyloarthropathies
HLA-B27
The association of AS with HLA-B27 is one of the strongest HLA-disease associations in any common disease:
- 80-95% of AS patients are HLA-B27 positive (White Europeans); odds ratio ~90-100
- In White Europeans, HLA-B27 frequency is ~8% in the general population vs ~90% in AS patients
- Only ~5% of HLA-B27-positive individuals develop AS, indicating that HLA-B27 is necessary but not sufficient
- Heritability of AS is >90%; HLA-B27 contributes <50% of this genetic risk
- First-degree relatives of AS patients have 5-16x greater risk of AS than HLA-B27+ general population individuals - implying HLA-B27-modifying genes
"Of patients who have ankylosing spondylitis, 88% to 96% are HLA-B27 positive, but only 5% of the HLA-B27 population develops ankylosing spondylitis." - Campbell's Operative Orthopaedics
HLA-B27 subtypes: Over 100 subtypes (B*27:01 to B*27:117+). HLA-B*27:05 is the most common subtype associated with AS in Europeans. B*27:06 and B*27:09 appear protective or non-pathogenic.
Mechanisms of HLA-B27 in AS - proposed hypotheses:
-
Arthritogenic peptide hypothesis: HLA-B27 presents specific self or bacterial (Klebsiella, Chlamydia) peptides to CD8+ cytotoxic T cells, triggering joint inflammation.
-
Misfolding/UPR hypothesis: HLA-B27 heavy chains have a propensity to misfold in the ER and form homodimers. Misfolded B27 activates the unfolded protein response (UPR), leading to IL-23 production and downstream Th17 pathway activation.
-
Free heavy chain hypothesis: Cell surface HLA-B27 homodimers (B27-HC) engage NK and T cell receptors (e.g., KIR3DL2), activating Th17 responses.
-
ERAP1 interaction: ERAP1 (aminopeptidase involved in trimming peptides for class I loading) variants strongly modify AS risk in an HLA-B27-dependent manner - loss-of-function ERAP1 variants protect against AS only in HLA-B27-positive individuals, directly implicating peptide processing in pathogenesis.
HLA-B27 and other spondyloarthropathies:
| Disease | HLA-B27 Frequency | Relative Risk |
|---|---|---|
| Ankylosing spondylitis | 90-95% | ~90 |
| Reactive arthritis | ~60-80% | ~37 |
| Psoriatic arthritis (axial) | ~50-70% | Variable |
| Enteropathic arthritis (axial) | ~50% | Variable |
| Undifferentiated SpA | ~70% | Variable |
Non-B27 MHC and non-MHC genes in AS: GWAS has identified 115 loci, including ERAP1, ERAP2, IL23R, IL12B, STAT3, CARD9, RUNX3. The IL-23/Th17 pathway genes are particularly overrepresented.
3C. Systemic Lupus Erythematosus (SLE)
HLA associations in SLE are less striking than in RA or AS but still significant:
- HLA-DR2 (DRB1*1501) and HLA-DR3 (DRB1*0301) are associated with increased SLE susceptibility (OR ~2-3)
- DR2/DR3 heterozygotes have higher risk than either homozygote
- HLA-DR2 associates particularly with anti-dsDNA and anti-Sm antibodies
- HLA-DR3 associates with anti-Ro/SSA and anti-La/SSB antibodies
- C4A null allele (class III MHC) - complement deficiency impairs immune complex clearance and is a strong SLE risk factor
- Non-MHC genes: IRF5, TREX1, STAT4, BLK, PTPN22, FCGR2A/3A, ITGAM
3D. Primary Sjogren's Syndrome (pSS)
- HLA-DR3 (DRB1*0301) and HLA-DQ2 (DQB1*0201) are the main risk alleles
- HLA-DQ associations mediated through linkage disequilibrium with DR3
- Anti-Ro/SSA antibodies associate strongly with DR3
- HLA-DRB1*1501 (DR2) also associated in some populations
3E. Juvenile Idiopathic Arthritis (JIA)
JIA is a heterogeneous disease with different HLA associations by subtype:
- RF-positive polyarticular JIA: Shares HLA-DRB1 shared epitope alleles with adult RA (DRB1*01/*04)
- Oligoarticular/RF-negative: HLA-DRB1*0801, *11, *1301; DRB1*1301-DQA1*01-DQB1*06 haplotype associated with oligoarticular disease
- Enthesitis-related arthritis (ERA): HLA-B27 associated (as in adult AS)
- Systemic JIA: Less clear HLA association; different pathogenic mechanism (autoinflammatory)
"The shared epitope (consisting of selected HLA-DRB1*01/*04 alleles) is associated only with RF-positive polyarticular JIA, a finding supporting the fact that this JIA category is the childhood equivalent of adult RA." - Rheumatology, 2-Volume Set (Elsevier)
3F. Other Rheumatic Diseases and HLA Associations (Summary Table)
| Disease | Key HLA Association |
|---|---|
| Rheumatoid arthritis | DRB1*0401, *0404, *0101 (Shared Epitope) |
| Ankylosing spondylitis | B*27 |
| Reactive arthritis | B*27 |
| Psoriatic arthritis | B*27 (axial); Cw*06 (psoriasis) |
| SLE | DR2 (DRB1*1501), DR3 (DRB1*0301) |
| Primary Sjogren's | DR3, DQ2 |
| Myositis (PM/DM) | DR3, DQ1 |
| Systemic sclerosis | DR1, DR5, DQ2 |
| Behcet's disease | B51 |
| Gout-flares | Not strongly HLA-linked |
| JIA (RF+ polyarticular) | Shared epitope DRB1*01/*04 |
| JIA (oligoarticular) | DRB1*1301, DRB1*0801 |
| Celiac disease | DQ2 (DQA1*05/DQB1*02), DQ8 |
Part 4: Note on HLA Typing
Why HLA Typing?
HLA typing is performed for:
- Transplantation - organ and hematopoietic stem cell transplantation (HSCT)
- Disease susceptibility/diagnosis - ankylosing spondylitis, celiac disease, narcolepsy
- Pharmacogenomics - predicting drug hypersensitivity (abacavir/HLA-B*57:01; carbamazepine/HLA-B*15:02)
- Research - population genetics, autoimmune disease studies
Methods of HLA Typing
1. Serological (Complement-Dependent Cytotoxicity - CDC) - Historical
- Lymphocytes incubated with panels of anti-HLA antibodies + complement
- Dead cells indicate HLA match
- Disadvantages: Can only distinguish major allele groups (low resolution); requires viable lymphocytes; laborious; cannot distinguish many alleles
- Now largely replaced by molecular methods
2. Cellular Typing - Historical
- Mixed Lymphocyte Reaction (MLR) - measures T cell proliferative response to allogeneic cells
- Primed Lymphocyte Test (PLT)
- Also replaced by molecular methods
3. Molecular/DNA-Based Methods - Current Standard
"HLA alleles are defined by their gene sequences and individuals can be typed by the polymerase chain reaction (PCR) using discriminating pairs of primers. Molecules encoded by the class II HLA-DP, -DQ, and -DR loci provoke CD4 T-cell responses, whereas HLA-A, -B, and -C gene products are targets for alloreactive CD8 T-cells." - Roitt's Essential Immunology
a. PCR-SSP (Sequence-Specific Primers)
- Multiple parallel PCR reactions each using primers specific for one allele
- Presence/absence of PCR product identifies the allele
- Medium resolution; fast; suited for routine typing
b. PCR-SSOP (Sequence-Specific Oligonucleotide Probe)
- PCR amplification of HLA loci, then hybridization with labeled allele-specific probes
- Can be done in reverse (reverse SSO/Luminex bead array) - highly multiplexed
- Medium to high resolution; now widely automated
c. PCR-SBT (Sequence-Based Typing)
- Sanger sequencing of amplified HLA exons (exons 2 and 3 for class I; exon 2 for class II)
- High-resolution (allele-level) typing
- Gold standard but laborious; subject to phase ambiguities
d. Next-Generation Sequencing (NGS)/Massively Parallel Sequencing
- Full-length HLA gene sequencing at ultra-high resolution
- Resolves phase ambiguities
- Becoming the new gold standard, especially for HSCT
- Cost-effective at scale; can type all HLA loci simultaneously
e. Reverse Transcriptase PCR / RSCA (Reference Strand-mediated Conformational Analysis)
- Fluorescent-labeled heteroduplex analysis
- Automated, high-throughput
f. Surrogate SNP-based Typing
- Single SNP variants in LD with HLA alleles (e.g., HCP5 rs2395029 as surrogate for HLA-B*57:01 with 99.9% predictive value)
- Useful in population screening; risk of false negatives in copy number variation regions
- Supplemented by serological phenotyping (B57/B58 detection) or skin patch testing
Resolution Levels in HLA Typing
| Level | Example | Use |
|---|---|---|
| Low (2-digit) | DRB1*04 | Screening, broad compatibility |
| Intermediate (4-digit) | DRB1*0401 | Solid organ transplant, disease assoc. |
| High/Allele (6-8 digit) | DRB1*04:01:01 | HSCT, pharmacogenomics |
"The level of HLA typing resolution required for hematopoietic stem cell transplantation differs from that of renal transplantation. Higher-resolution HLA typing is required to match the donor and recipient for stem cell transplantation because stem cell transplantation involves the transfer of an entire immune system to the patient." - Henry's Clinical Diagnosis and Management by Laboratory Methods
HLA Typing for HSCT
Current standard: Allele-level (high-resolution) matching of HLA-A, -B, -C, and -DRB1 for unrelated donors. HLA-DQB1 and HLA-DPB1 matching is also considered and may affect outcomes. Single mismatches may be tolerated but multiple mismatches negatively impact survival. HLA-DPB1 non-permissive mismatches increase GvHD risk.
HLA-B*57:01 Testing in Pharmacogenomics
Screening for HLA-B*57:01 before initiating abacavir (HIV antiretroviral) eliminates hypersensitivity reactions (NPV ~100%). FDA-required pharmacogenomic label. Similar testing recommended for:
- HLA-B*15:02 before carbamazepine (Stevens-Johnson syndrome - particularly in Asian populations)
- HLA-B*58:01 before allopurinol (SJS/TEN in Asians)
- HLA-A*31:01 before carbamazepine in Europeans
Key Summary
| Topic | Key Points |
|---|---|
| MHC class I | All nucleated cells; presents 8-10aa peptides to CD8+ T cells; endogenous pathway via proteasome-TAP |
| MHC class II | APCs; presents 15-20aa peptides to CD4+ T cells; exogenous pathway via endosome-HLA-DM-CLIP |
| Endogenous pathway | Proteasome → TAP → ER → peptide loading complex → MHC I → cell surface |
| Exogenous pathway | Endocytosis → lysosome → MIIC → CLIP exchange (HLA-DM) → MHC II → cell surface |
| RA | Shared epitope (DRB1 pos 70-74); DRB1*0401/*0404 highest risk; ACPA link; PTPN22 co-risk |
| AS | HLA-B27 (90% AS patients); ERAP1 interaction; B27 misfolding/UPR/Th17 pathway |
| SLE | HLA-DR2, DR3; C4A null; complement clearance of immune complexes |
| pSS | HLA-DR3, DQ2 |
| HLA typing | Serological (historical) → PCR-SSP/SSOP/SBT → NGS (current gold standard for HSCT) |
Sources:
- Roitt's Essential Immunology (Essentials)
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- Rheumatology 2-Volume Set (Elsevier, 2022)
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Janeway's Immunobiology, 10th Edition
- Cellular and Molecular Immunology (Abbas)
- Campbell's Operative Orthopaedics, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.