Ards according to ATS 2025 guidelines
"acute respiratory distress syndrome" AND "guidelines"
ATS 2025 ARDS guidelines American Thoracic Society
"acute respiratory distress syndrome" AND "mechanical ventilation" AND "American Thoracic Society"
ATS 2024 ARDS clinical practice guideline ECMO prone positioning Am J Respir Crit Care Med
https://reference.medscape.com/cc2/p10/management-acute-resp…
PMID: 38032683
https://academic.oup.com/ajrccm/article/209/1/24/8427573
ATS 2024 ARDS guideline full recommendations corticosteroids dosing ECMO criteria neuromuscular blockade PEEP strategy details
https://pmc.ncbi.nlm.nih.gov/articles/PMC10870893
ARDS: ATS Clinical Practice Guideline (2024)
Note on the "2025" guideline: The most recent ATS ARDS-specific guideline was published January 2024 in Am J Respir Crit Care Med (Qadir N et al., 209(1):24–36, PMID: 38032683). The ATS guideline published in November 2025 addressed Community-Acquired Pneumonia (CAP), not ARDS. The 2024 ARDS guideline is the current standard.
Berlin Definition of ARDS (Diagnostic Criteria)
| Criterion | Requirement |
|---|---|
| Timing | Onset within 1 week of known clinical insult or new/worsening respiratory symptoms |
| Chest Imaging | Bilateral opacities not fully explained by lobar/lung collapse, effusions, or nodules |
| Origin of Edema | Respiratory failure not fully explained by cardiac failure or fluid overload |
| Oxygenation | PaO₂/FiO₂ ≤ 300 mmHg with PEEP ≥ 5 cmH₂O |
Severity Classification
| Severity | PaO₂/FiO₂ Ratio |
|---|---|
| Mild | 200–300 mmHg |
| Moderate | 100–200 mmHg |
| Severe | ≤ 100 mmHg |
ATS 2024 Guideline: The 5 Core Recommendations
1. Systemic Corticosteroids ✅
- Recommendation: Suggest using corticosteroids for patients with ARDS.
- Rationale: Meta-analyses of RCTs (including DEXA-ARDS, LaSRS, and others) show reductions in mortality, duration of mechanical ventilation, and ICU length of stay.
- Practical considerations:
- Most evidence supports methylprednisolone or dexamethasone
- Commonly used regimens: dexamethasone 20 mg/day × 5 days → 10 mg/day × 5 days; or methylprednisolone 1 mg/kg/day
- Caution: Risk of hyperglycemia, secondary infections, ICU-acquired weakness; avoid in patients with active uncontrolled infections
- Benefit appears greatest in early, moderate-to-severe ARDS (not late fibroproliferative phase)
2. Venovenous ECMO (VV-ECMO) ✅ (selected patients)
- Recommendation: Suggest using VV-ECMO in selected patients with severe ARDS.
- Key trials: CESAR (2009) and EOLIA (2018) — EOLIA showed no statistically significant 60-day mortality benefit, but high crossover rate (28%) confounded results; Bayesian analysis supported benefit.
- Patient selection criteria:
- Reversible etiology of respiratory failure
- Severe hypoxemia: PaO₂/FiO₂ < 80 mmHg or hypercapnia (pH < 7.25 with PaCO₂ > 60 mmHg)
- Failure of conventional therapies (lung-protective ventilation, high PEEP, prone positioning, NMBAs)
- Early phase of ARDS (< 7 days of mechanical ventilation)
- Few risk factors for futility
- Implementation: Should be delivered at high-volume ECMO centers with multidisciplinary teams; as part of a comprehensive care package including lung-protective ventilation and prone positioning.
3. Neuromuscular Blocking Agents (NMBAs) ✅ (early severe ARDS)
- Recommendation: Suggest using neuromuscular blockers in patients with early severe ARDS.
- Key trials: ACURASYS (2010) showed benefit; ROSE trial (2019) showed no mortality benefit with routine NMBA — however, ROSE used lighter sedation in control arm.
- Rationale: NMBAs may reduce patient self-inflicted lung injury (P-SILI), reduce dyssynchrony, facilitate lung-protective ventilation, and reduce oxygen consumption.
- Timing: "Early" = within first 48 hours of severe ARDS onset.
- Caution: ICU-acquired weakness risk; should not be used routinely in moderate ARDS without specific indication.
- Notable divergence from ESICM 2023: ESICM recommends against routine NMBA use in moderate-to-severe ARDS not due to COVID-19; ATS conditionally supports use in early severe ARDS.
4. Higher PEEP (without LRMs) ✅ in moderate-to-severe ARDS
- Recommendation: Suggest using higher PEEP as opposed to lower PEEP in patients with moderate to severe ARDS.
- Key evidence: Meta-analyses of ALVEOLI, LOV, and ExPress trials showed mortality benefit in moderate-to-severe ARDS subgroup.
- Implementation: Higher PEEP strategies (e.g., PEEP ≥ 10–15 cmH₂O depending on FiO₂) are preferred; PEEP/FiO₂ tables from ARDSnet can guide titration.
- Important caveat: Higher PEEP should be used without accompanying prolonged lung recruitment maneuvers (see below).
5. Against Prolonged Lung Recruitment Maneuvers (LRMs) ❌
- Recommendation: Recommend against using prolonged lung recruitment maneuvers in patients with moderate to severe ARDS.
- Key evidence: ART trial (2017) — high-pressure prolonged recruitment maneuvers (sustained inflation at 45 cmH₂O for 1 minute) significantly increased mortality compared to PEEP titration alone.
- Important distinction: This strong recommendation is specifically against prolonged LRMs (sustained high-pressure maneuvers); brief LRMs may have insufficient evidence to make a firm recommendation.
Foundational Ventilation Strategies (from 2017 Guideline, still current)
| Strategy | Recommendation |
|---|---|
| Low tidal volume | 6 mL/kg ideal body weight (IBW); strong recommendation |
| Plateau pressure | ≤ 30 cmH₂O; strong recommendation |
| Prone positioning | ≥ 12 hours/day in severe ARDS (PaO₂/FiO₂ < 150); strong recommendation |
| High-flow nasal cannula (HFNC) | Consider before intubation in mild-to-moderate ARDS |
| Driving pressure | Target < 15 cmH₂O |
Summary Table: ATS 2024 ARDS Recommendations
| Intervention | Recommendation | Strength | Certainty |
|---|---|---|---|
| Corticosteroids | FOR | Conditional | Moderate |
| VV-ECMO (severe, selected) | FOR | Conditional | Low |
| NMBAs (early severe ARDS) | FOR | Conditional | Low |
| Higher PEEP (moderate-severe) | FOR (without LRMs) | Conditional | Low–Moderate |
| Prolonged LRMs | AGAINST | Strong | Moderate |
Clinical Approach to ARDS Management
- Identify and treat the underlying cause (sepsis, pneumonia, aspiration, etc.)
- Respiratory support: HFNC → NIV → intubation based on severity
- Lung-protective MV: TV 6 mL/kg IBW, plateau ≤ 30 cmH₂O, driving pressure < 15 cmH₂O
- Higher PEEP (no prolonged LRMs) in moderate-to-severe
- Prone positioning ≥ 12 h/day in severe ARDS
- NMBAs in early severe ARDS (first 48 h)
- Corticosteroids — suggest use across ARDS severity
- Conservative fluid strategy after initial resuscitation
- VV-ECMO — consider in selected severe refractory ARDS at expert centers
Causes of ARDS Berlin diagnostic criteria for ARDS Diagnosis of acute respiratory distress syndrome in emergency Ventilator management of ARDS Awake proning in ARDS INVESTIGATIONS and Management of ARDS
"awake prone positioning" AND "acute respiratory distress syndrome"
ARDS emergency diagnosis investigations chest X-ray CT ABG management 2024
ARDS chest X-ray bilateral infiltrates acute respiratory distress syndrome
ARDS: Complete Clinical Review
1. CAUSES OF ARDS
Direct (Pulmonary) Causes
| Cause | Key Points |
|---|---|
| Aspiration of gastric contents | Most common direct cause; chemical pneumonitis |
| Bacterial pneumonia (diffuse) | Legionella, Gram-negatives, S. pneumoniae |
| Viral pneumonia | Influenza, SARS-CoV-2 (COVID-19), MERS |
| Chest trauma / lung contusion | Direct mechanical parenchymal injury |
| Near drowning | |
| Pneumocystis jiroveci (PJP) | Immunocompromised hosts |
| Toxic inhalations | Smoke, chlorine, ammonia, crack cocaine |
| Diffuse fungal pneumonias | Candida, Cryptococcus |
| Miliary tuberculosis |
Indirect (Systemic/Extrapulmonary) Causes
| Cause | Key Points |
|---|---|
| Severe sepsis / septic shock | Most common overall cause; inflammatory mediators damage alveolar-capillary membrane |
| Acute pancreatitis | Lipase + inflammatory mediators reach lung via circulation |
| Multiple trauma + fat emboli | Long-bone fractures → fat emboli → pulmonary capillary injury |
| Transfusion (TRALI) | Leading cause of transfusion-related morbidity/mortality |
| Toxic ingestions | Aspirin, tricyclic antidepressants, opioids |
| Post-cardiopulmonary bypass | |
| Primary graft failure (lung transplant) | |
| Diffuse alveolar hemorrhage | Vasculitis (Goodpasture, ANCA), post-BMT |
| Acute eosinophilic pneumonia | |
| Lupus pneumonitis |
Risk Factors for Developing ARDS (Given an Underlying Cause)
- Chronic alcohol abuse
- Hypoproteinemia
- Advanced age
- High injury severity score (ISS) or APACHE score
- Multiple blood transfusions
- Cigarette smoking
- Blood group A
- Protective: Diabetes mellitus, pre-hospital antiplatelet therapy
Fishman's Pulmonary Diseases and Disorders, Table 141-4
2. BERLIN DIAGNOSTIC CRITERIA FOR ARDS (2012)
4 Required Criteria (ALL must be met)
| Criterion | Requirement |
|---|---|
| Timing | Onset within 1 week of a known clinical insult or new/worsening respiratory symptoms |
| Chest Imaging | Bilateral opacities not fully explained by pleural effusions, lobar/lung collapse, or nodules |
| Origin of Edema | Respiratory failure not fully explained by cardiac failure or fluid overload |
| Oxygenation | PaO₂/FiO₂ ≤ 300 mmHg with PEEP or CPAP ≥ 5 cmH₂O |
Severity Stratification
| Severity | PaO₂/FiO₂ | PEEP | Hospital Mortality |
|---|---|---|---|
| Mild | 200–300 mmHg | ≥ 5 cmH₂O | ~27% |
| Moderate | 100–200 mmHg | ≥ 5 cmH₂O | ~32% |
| Severe | ≤ 100 mmHg | ≥ 5 cmH₂O | ~45% |
2024 Global Definition Update (Matthay et al., AJRCCM 2024): Expanded to include non-intubated patients on HFNC/NIV; lung ultrasound accepted for imaging criterion; SpO₂/FiO₂ ≤ 315 can replace PaO₂/FiO₂ when ABG unavailable.
Fishman's Pulmonary Diseases, Tables 141-1B; Tintinalli's Emergency Medicine, Table 29B-1
3. DIAGNOSIS OF ARDS IN THE EMERGENCY DEPARTMENT
Clinical Features
- Acute-onset dyspnea and tachypnea
- Hypoxemia refractory to supplemental O₂ (hallmark)
- Diffuse bilateral crackles on auscultation
- Tachycardia, cyanosis
- Fever, cough (if infectious etiology)
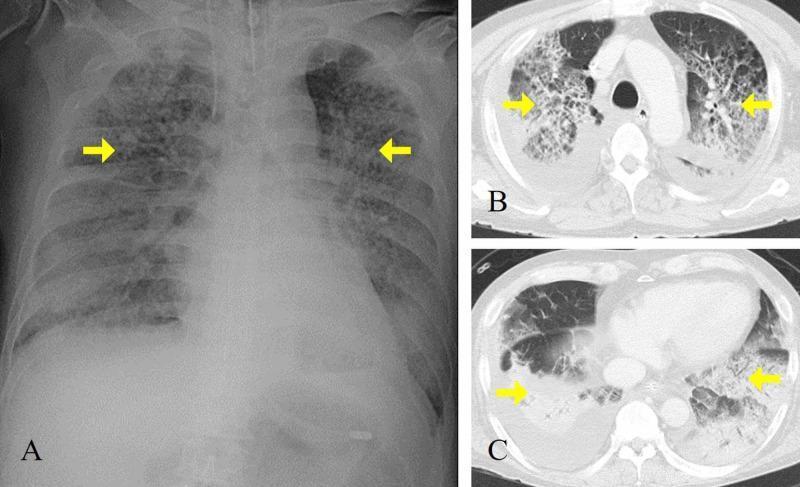
Emergency Diagnostic Approach
- Bilateral alveolar opacities obscuring vascular markings
- "Bat-wing" or "white-out" pattern
- Differentiates from cardiogenic edema: No Kerley B lines, no cardiomegaly, no upper lobe diversion (though overlap can occur)
- Calculate PaO₂/FiO₂ ratio (requires known FiO₂)
- Confirms severity and diagnosis
- Early ARDS: hypoxemia + hypocapnia (hyperventilation); Late/severe: hypercapnia + metabolic acidosis
- BNP/NT-proBNP: Low or normal favors ARDS; markedly elevated favors cardiogenic edema
- Echocardiography (POCUS): Assess LV function, wall motion abnormalities, valvular disease
- Clinical: No orthopnea/PND, no peripheral edema pattern, not responsive to diuretics
ED Chest Imaging: ARDS Appearance
Differential Diagnosis in the ED
| Condition | Differentiating Feature |
|---|---|
| Cardiogenic pulmonary edema | Elevated BNP, cardiomegaly, bilateral effusions, Kerley B lines, responds to diuretics |
| Bilateral pneumonia | May coexist; positive cultures/PCR |
| Diffuse alveolar hemorrhage | Hemoptysis, hemosiderin-laden macrophages on BAL |
| Acute eosinophilic pneumonia | Peripheral eosinophilia, BAL eosinophilia |
| Cryptogenic organizing pneumonia | Subacute, peripheral consolidation pattern |
4. INVESTIGATIONS IN ARDS
Bedside / Immediate
| Investigation | Purpose |
|---|---|
| Arterial Blood Gas (ABG) | P/F ratio, ventilation status, acid-base |
| Continuous SpO₂ | Oxygenation monitoring |
| Chest X-ray | Berlin imaging criterion |
| ECG | Exclude cardiac cause, arrhythmias |
| POCUS (lung + cardiac) | B-lines, consolidation; LV/RV function |
Laboratory
| Test | Purpose |
|---|---|
| FBC / CBC | Leukocytosis, thrombocytopenia (sepsis/DIC) |
| Metabolic panel (U&E, LFTs, Cr) | Multiorgan failure monitoring |
| Lactate | Tissue hypoperfusion severity |
| Coagulation (PT, APTT, fibrinogen, D-dimer) | DIC screen |
| Blood cultures × 2 | Bacteremia/sepsis source |
| Troponin + BNP/NT-proBNP | Exclude cardiogenic cause |
| CRP, Procalcitonin | Infection/inflammatory markers |
| LDH, Ferritin | Elevated in ARDS; severity markers |
| Serum albumin | Hypoproteinemia = ARDS risk factor |
| Sputum culture + sensitivity | Causative organisms |
| Amylase/Lipase | If pancreatitis suspected |
| Respiratory PCR panel | Influenza A/B, SARS-CoV-2, RSV |
| Electrolytes (Mg²⁺, PO₄³⁻, Ca²⁺) | ICU management, arrhythmia prevention |
Targeted / Advanced
| Investigation | Indication |
|---|---|
| CT chest | Complications (pneumothorax, effusions, fibrosis); atypical features; barotrauma |
| Echocardiography (formal) | LV dysfunction, valvular disease, pulmonary hypertension, RV failure |
| Bronchoscopy + BAL | Identify infection, DAH, eosinophilic pneumonia; culture if VAP suspected |
| HIV serology | PJP risk |
| ANCA, anti-GBM antibodies | Vasculitis/Goodpasture syndrome |
| Urine Legionella antigen | If Legionella pneumonia suspected |
| Thyroid function | If amiodarone toxicity or thyroid disease considered |
5. VENTILATOR MANAGEMENT OF ARDS
Overall Goals
- Maintain SpO₂ 88–95% (PaO₂ 55–80 mmHg) — avoid excessive hyperoxia
- Prevent VILI (volutrauma, barotrauma, atelectrauma, biotrauma)
- Allow permissive hypercapnia if needed for safe low-volume ventilation
Lung-Protective Ventilation (ARDSNet ARMA Protocol)
| Parameter | Target |
|---|---|
| Mode | Volume Control (VC-AC) preferred |
| Tidal Volume | 6 mL/kg PBW (can reduce to 4 mL/kg if Pplat > 30) |
| Plateau Pressure (Pplat) | ≤ 30 cmH₂O |
| Driving Pressure | < 15 cmH₂O (Pplat − PEEP) |
| PEEP | Higher PEEP strategy (titrate per PEEP/FiO₂ table); ≥ 5 cmH₂O minimum |
| FiO₂ | Titrate to SpO₂ 88–95%; avoid prolonged high FiO₂ (toxicity risk) |
| Respiratory Rate | 6–35 breaths/min |
| pH Target | 7.30–7.45; accept down to 7.20 with permissive hypercapnia |
| I:E Ratio | Conventional 1:2 |
ARMA Trial Result: Low TV (6 mL/kg) vs Traditional (12 mL/kg) → mortality 31% vs 39.8% (p=0.007) — Fishman's Pulmonary Diseases, Table 141-10
Calculating Predicted Body Weight (PBW)
- Male: 50 + 2.3 × (height in inches − 60)
- Female: 45.5 + 2.3 × (height in inches − 60)
Use PBW, NOT actual body weight — critical in obese patients
PEEP/FiO₂ Table (ARDSNet Higher PEEP Table for Moderate-Severe ARDS)
| FiO₂ | 0.3 | 0.4 | 0.5 | 0.6 | 0.7 | 0.8 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|---|---|
| PEEP (cmH₂O) | 5 | 8–10 | 10 | 10–14 | 14 | 14–18 | 16–18 | 18–24 |
Lung Recruitment Maneuvers (LRMs)
- Strong recommendation AGAINST prolonged LRMs (ATS 2024)
- ART Trial (2017): Sustained inflation at 45 cmH₂O → significantly increased 28-day mortality
- Brief, step-wise LRMs: insufficient evidence; may be used with caution in selected cases
Permissive Hypercapnia
- Allow PaCO₂ to rise to maintain safe low TV ventilation
- Accept pH ≥ 7.20–7.25
| Contraindication |
|---|
| Raised intracranial pressure (trauma, mass lesion) |
| Acute cerebrovascular disease / stroke |
| Acute myocardial ischemia |
| Severe pulmonary hypertension / RV failure |
| Severe uncorrected metabolic acidosis |
| Pregnancy |
| Sickle cell disease |
| Tricyclic antidepressant overdose |
Mechanisms of VILI (and Prevention)
| Mechanism | Cause | Prevention |
|---|---|---|
| Volutrauma | Alveolar overdistension (high TV) | TV 6 mL/kg PBW |
| Barotrauma | Excess airway pressure → pneumothorax, pneumomediastinum | Pplat ≤ 30 cmH₂O |
| Atelectrauma | Repetitive alveolar opening/closing | Adequate PEEP |
| Biotrauma | Cytokine release → remote organ injury | All of the above |
6. PRONE POSITIONING (INTUBATED) IN ARDS
Mechanisms
- Homogenizes distribution of tidal volumes (recruits collapsed dorsal lung)
- Reduces V/Q mismatch and intrapulmonary shunt
- Reduces pleural pressure gradient
- Facilitates secretion drainage
PROSEVA Trial (2013)
- Population: Severe ARDS (PaO₂/FiO₂ < 150 mmHg), early (< 36 h), on lung-protective MV
- Intervention: Prone ≥ 16 h/day vs supine
- 28-day mortality: 16% vs 32.8% (p<0.001); 90-day mortality: 23.6% vs 41%
ATS 2017 / Current Recommendation
- Strong recommendation for prone positioning ≥ 12–16 hours/day in severe ARDS (PaO₂/FiO₂ < 150 mmHg)
- Initiate early (within 36 hours of MV)
- Continue until hypoxemia resolves
Complications of Prone Positioning
- Pressure ulcers (face, chest, knees)
- Endotracheal tube displacement/obstruction
- Central line/arterial line dislodgement
- Facial edema
- Temporary hemodynamic instability during turning
7. AWAKE PRONE POSITIONING IN ARDS
Definition
Physiologic Rationale
- Same V/Q redistribution as intubated proning
- Prevents "sinus" pattern lung injury (dorsal collapse in supine position)
- Reduces work of breathing over time
- May reduce risk of patient self-inflicted lung injury (P-SILI)
- Potential to avoid/delay intubation
Evidence
| Study | Finding |
|---|---|
| Graziani et al. Meta-analysis 2024 [PMID 37796372] | Awake proning in COVID-related ARDS → reduced intubation rates; improved oxygenation |
| Freire et al. SR/MA 2024 [PMID 38712558] | Improved oxygenation but no significant effect on mortality or ICU LOS in unventilated severe COVID-19 |
| Othman et al. RCT 2023 [PMID 35909384] | Significant improvement in SpO₂ and RR in non-intubated COVID ARDS |
| CATS Trial, PROF Trial (2021–2022) | Awake proning improved oxygenation; no clear reduction in intubation in general ARDS |
Key limitation: Most evidence is from COVID-19 ARDS. Benefit in general non-COVID ARDS is less clear. Should not delay necessary intubation.
Practical Protocol
| Step | Details |
|---|---|
| Patient selection | Cooperative, awake, spontaneously breathing; SpO₂ < 94% on ≥4 L/min O₂ or HFNC; no immediate intubation criteria |
| Positioning | Full prone or 3/4 prone; head turned to one side; pillow under chest and pelvis |
| Duration | ≥ 3–4 hours per session; target ≥ 8–16 hours/day cumulative if tolerated |
| Support device | Continue HFNC/NIV/supplemental O₂ during proning |
| Monitoring | SpO₂, RR, work of breathing (accessory muscle use), comfort |
| Response check | SpO₂ improvement ≥ 3–5%; PaO₂/FiO₂ improvement |
| Non-responders | Reassess for intubation; do not persist if worsening |
Contraindications to Awake Proning
- Altered consciousness / uncooperative
- Immediate intubation criteria (GCS < 13, hemodynamic instability, impending arrest)
- Facial/thoracic trauma
- Recent abdominal surgery
- Hemoptysis
- Pregnancy
- Severe claustrophobia or agitation
- Morbid obesity (relative)
8. COMPLETE MANAGEMENT SUMMARY
ARDS Suspected → Confirm Berlin Criteria
↓
1. TREAT UNDERLYING CAUSE
Sepsis → broad-spectrum antibiotics + source control
Pneumonia → antivirals/antibiotics
Aspiration → supportive; antibiotics if secondary infection
Pancreatitis → supportive; fluids
↓
2. RESPIRATORY SUPPORT (escalate based on severity)
Mild ARDS → HFNC (target SpO₂ 92–96%) ± Awake Proning
Moderate/Severe → Intubation + Mechanical Ventilation
↓
3. LUNG-PROTECTIVE VENTILATION
TV: 6 mL/kg PBW | Pplat ≤ 30 | Driving pressure < 15
Higher PEEP (without prolonged LRMs)
Permissive hypercapnia if needed
↓
4. PRONE POSITIONING ≥16 h/day (if PaO₂/FiO₂ < 150)
↓
5. NMBAs — if early severe ARDS (first 48h), dyssynchrony
↓
6. CORTICOSTEROIDS — suggest use (conditional)
↓
7. CONSERVATIVE FLUID MANAGEMENT (post-resuscitation)
↓
8. VV-ECMO — refractory severe ARDS, ECMO-capable centre
ATS 2024 Recommendations Summary
| Intervention | Recommendation | Strength | Evidence |
|---|---|---|---|
| Corticosteroids | FOR | Conditional | Moderate |
| VV-ECMO (severe, selected) | FOR | Conditional | Low |
| NMBAs (early severe) | FOR | Conditional | Low |
| Higher PEEP (mod-severe) | FOR (no LRMs) | Conditional | Low–Moderate |
| Prolonged LRMs | AGAINST | Strong | Moderate |
Give a complete definition of ards according to berlins criteria
Berlin definition ARDS 2012 complete criteria JAMA Ranieri full text
Berlin Definition of ARDS (2012) — Complete
Background
Conceptual (Pathophysiological) Definition
"ARDS is an acute, diffuse, inflammatory lung injury leading to increased pulmonary vascular permeability, increased lung weight, and loss of aerated lung tissue — characterized by hypoxemia and bilateral radiographic opacities, associated with increased venous admixture (shunting), increased physiological dead space, and decreased lung compliance." — ARDS Definition Task Force, JAMA 2012
The 4 Diagnostic Criteria (ALL must be present)
Criterion 1 — TIMING
Acute onset within 1 week of a known clinical insult, OR new or worsening respiratory symptoms
- "Acute" is operationally defined as ≤ 7 days from the triggering event
- Most cases occur within 72 hours of the precipitating cause
- This replaces the vague AECC term "acutely"
Criterion 2 — CHEST IMAGING
Bilateral opacities on chest radiograph or CT — not fully explained by effusions, lobar/lung collapse, or nodules
- Opacities must be bilateral (involving both lung fields)
- They must be consistent with pulmonary edema in appearance
- They cannot be fully attributed to:
- Pleural effusions
- Lobar or whole-lung atelectasis/collapse
- Nodules/masses
- CT chest is acceptable if CXR is technically inadequate
- Note: The 2024 Global Definition update also accepts lung ultrasound (bilateral B-lines / consolidation)
Criterion 3 — ORIGIN OF EDEMA
Respiratory failure not fully explained by cardiac failure or fluid overload
- Excludes cardiogenic (hydrostatic) pulmonary edema as the primary cause
- No longer requires a pulmonary artery wedge pressure (PCWP) ≤ 18 mmHg (removed from Berlin definition)
- If no identifiable ARDS risk factor is present, objective assessment is required (e.g., echocardiography) to exclude hydrostatic/cardiogenic edema
Criterion 4 — OXYGENATION
PaO₂/FiO₂ ratio ≤ 300 mmHg with PEEP or CPAP ≥ 5 cmH₂O
- Must be measured with the patient receiving at minimum PEEP or CPAP ≥ 5 cmH₂O
- This requirement was added because PEEP level significantly affects the P/F ratio — accounting for it removes variability in diagnosis
- The oxygenation criterion then determines severity
Severity Stratification (Based on PaO₂/FiO₂ on PEEP ≥ 5 cmH₂O)
| Severity | PaO₂/FiO₂ Ratio | Observed Hospital Mortality |
|---|---|---|
| Mild | > 200 and ≤ 300 mmHg | ~27% |
| Moderate | > 100 and ≤ 200 mmHg | ~32% |
| Severe | ≤ 100 mmHg | ~45% |
Important: The Berlin definition abolished the category of "Acute Lung Injury (ALI)." What was previously ALI (PaO₂/FiO₂ ≤300 but >200) is now Mild ARDS. ALI is an obsolete term.
Complete Berlin Definition Table
| Variable | Criteria |
|---|---|
| Timing | Within 1 week of a known clinical insult or new/worsening respiratory symptoms |
| Chest Imaging | Bilateral opacities — not fully explained by effusions, lobar/lung collapse, or nodules |
| Origin of Edema | Not fully explained by cardiac failure or fluid overload; objective assessment (e.g., echo) needed if no ARDS risk factor present |
| Oxygenation (Mild) | 200 < PaO₂/FiO₂ ≤ 300 mmHg on PEEP/CPAP ≥ 5 cmH₂O |
| Oxygenation (Moderate) | 100 < PaO₂/FiO₂ ≤ 200 mmHg on PEEP/CPAP ≥ 5 cmH₂O |
| Oxygenation (Severe) | PaO₂/FiO₂ ≤ 100 mmHg on PEEP/CPAP ≥ 5 cmH₂O |
Key Improvements Over the 1994 AECC Definition
| Issue in AECC | How Berlin Addressed It |
|---|---|
| "Acute onset" was undefined | Operationally defined as < 1 week |
| CXR criterion was vague | Specified bilateral opacities not explained by collapse, effusions, or nodules |
| PCWP ≤ 18 mmHg was inaccurate and impractical | Removed PCWP requirement; replaced with clinical exclusion ± echocardiography |
| No severity categories | Added 3 severity levels (mild, moderate, severe) with validated mortality correlation |
| P/F ratio not standardized for PEEP | Required PEEP ≥ 5 cmH₂O when measuring P/F ratio |
| Term "ALI" caused confusion | ALI abolished — now called "Mild ARDS" |
Important Notes on Applying the Criteria
-
PEEP requirement: The P/F ratio must be obtained while the patient is on PEEP/CPAP ≥ 5 cmH₂O. A patient breathing room air or on minimal oxygen may not meet the oxygenation criterion even if hypoxemic — they need to be formally tested.
-
Not a diagnosis of exclusion per se, but cardiac failure must be ruled out. If no clear ARDS risk factor exists, echocardiography is required to confirm non-cardiogenic etiology.
-
Severity is dynamic — a patient can transition between severity categories as the disease progresses or responds to treatment. Severity at 24 hours after diagnosis carries stronger prognostic value than at initial presentation.
-
Histological correlation: The Berlin definition has imperfect concordance with diffuse alveolar damage (DAD) on autopsy — DAD is confirmed in ~45% of mild, ~72% of moderate, and ~58% of severe ARDS cases, indicating the clinical definition is broader than pure DAD.
Latest tb drug regimens
"tuberculosis" AND "treatment regimen"
WHO 2022 2023 2024 tuberculosis treatment guidelines latest drug regimens rifampicin pretomanid bedaquiline
WHO 2024 tuberculosis treatment guidelines drug susceptible TB MDR-TB XDR-TB regimens BPaLM 6-month short course
https://pmc.ncbi.nlm.nih.gov/articles/PMC11755361
Latest TB Drug Regimens
- ATS/CDC/ERS/IDSA 2025 Updated Clinical Practice Guideline (Ann Am Thorac Soc, 2025 — PMC11755361)
- WHO Consolidated Guidelines Module 4: DR-TB Treatment (2022 update)
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
PART 1: LATENT TB INFECTION (LTBI) — Preventive Therapy
| Regimen | Drugs | Duration | Frequency | Notes |
|---|---|---|---|---|
| 3HP ⭐ (Preferred) | Isoniazid (H) + Rifapentine (P) | 3 months | Once weekly | Regimen of choice for children >2 yrs and all adults including HIV+; DOT or self-administered both acceptable |
| 4R | Rifampin (R) alone | 4 months | Daily | Preferred alternative; excellent tolerability |
| 3HR | Isoniazid + Rifampin | 3 months | Daily | Acceptable alternative |
| 1HP | Isoniazid + Rifapentine | 1 month | Daily | For HIV+ individuals; noninferior to 9H (2020 WHO guideline) |
| 6H / 9H | Isoniazid alone | 6–9 months | Daily or twice weekly | Acceptable; less preferred due to longer duration and hepatotoxicity risk |
⚠️ Rifampin + Pyrazinamide (2RZ) for 2 months is NO longer recommended — unacceptable rates of hepatotoxicity and death. Caution with rifamycin-based LTBI regimens in HIV+ patients due to drug interactions with ART.
Harrison's 22e, 2025 | Lippincott Pharmacology
PART 2: ACTIVE DRUG-SUSCEPTIBLE TB (DS-TB)
Standard 6-Month Regimen (Gold Standard)
| Phase | Drugs | Duration | Frequency |
|---|---|---|---|
| Intensive Phase | Hisoniazid + Rifampin + Pyrazinamide + Ethambutol | 2 months | Daily (preferred) or 3×/week |
| Continuation Phase | Hisoniazid + Rifampin | 4 months | Daily, 5 days/week, or 3×/week |
| Total | 6 months |
- Cavitary disease on CXR AND positive sputum culture at 2 months
- 2-month course of pyrazinamide not completed
- HIV-infected, not receiving ART
- Delayed culture conversion (positive cultures beyond 2 months)
- TB meningitis (continuation phase 10 months total; add dexamethasone)
- Bone/joint TB — some guidelines recommend 9 months total
NEW: 4-Month Regimen for DS-TB ⭐ (2022–2025 Update)
| Phase | Drugs | Duration |
|---|---|---|
| Intensive | Isoniazid + Rifapentine + Pyrazinamide + Moxifloxacin | 2 months (8 weeks) |
| Continuation | Isoniazid + Rifapentine + Moxifloxacin | 2 months (9 weeks) |
| Total | 4 months |
- Noninferior to 6-month standard in large multinational RCT
- Conditional recommendation by WHO and ATS/CDC/ERS/IDSA 2025
- Applicable to HIV+ patients with CD4 > 100
- Requires fluoroquinolone resistance testing before use in high-resistance settings
- Higher daily pill burden than standard regimen
Standard Drug Doses (Adults)
| Drug | Abbreviation | Daily Dose | Max Dose | Key Side Effects |
|---|---|---|---|---|
| Isoniazid | H | 5 mg/kg | 300 mg | Peripheral neuropathy (prevent with B₆), hepatotoxicity, lupus-like |
| Rifampin | R | 10 mg/kg | 600 mg | Hepatotoxicity, orange discolouration of fluids, drug interactions (CYP450 inducer), thrombocytopenia |
| Pyrazinamide | Z | 15–30 mg/kg | 2 g | Hepatotoxicity, hyperuricemia, arthralgia |
| Ethambutol | E | 15–25 mg/kg | 1.6 g | Optic neuritis (dose-dependent; monitor visual acuity), colour vision changes |
| Rifapentine | P | 1200 mg (≥50 kg) | 1200 mg | Similar to rifampin; less CYP induction |
| Moxifloxacin | M | 400 mg | 400 mg | QTc prolongation, hepatotoxicity |
PART 3: DRUG-RESISTANT TB (DR-TB)
Classification
| Type | Definition |
|---|---|
| RR-TB | Rifampin-resistant (with or without other resistance) |
| MDR-TB | Resistant to isoniazid AND rifampin |
| Pre-XDR-TB | MDR-TB + resistant to any fluoroquinolone |
| XDR-TB | MDR-TB + resistant to fluoroquinolone AND bedaquiline OR linezolid |
A. 6-Month BPaLM Regimen ⭐⭐ (WHO 2022 / ATS 2025 — STRONG Recommendation)
| Drug | Dose |
|---|---|
| Bedaquiline | 400 mg daily × 2 weeks → 200 mg 3×/week × 22 weeks |
| Pretomanid | 200 mg daily |
| Linezolid | 600 mg daily (can reduce to 300 mg if toxicity) |
| Moxifloxacin | 400 mg daily |
| Duration | 6 months (26 weeks) |
- Based on TB-PRACTECAL trial: 89% favourable outcome vs ~52% with standard regimens
- All-oral regimen; no injectables
- Strong recommendation by ATS/CDC/ERS/IDSA 2025 over ≥15-month regimens
- WHO 2022 recommendation for MDR/RR-TB and pre-XDR-TB aged ≥14 years without prior BPaL exposure
B. 6-Month BPaL Regimen ⭐⭐ (For Fluoroquinolone-Resistant / Pre-XDR-TB / XDR-TB)
| Drug | Dose |
|---|---|
| Bedaquiline | 400 mg daily × 2 weeks → 200 mg 3×/week × 22 weeks |
| Pretomanid | 200 mg daily |
| Linezolid | 600 mg daily (reduce to 300 mg if needed) |
| Duration | 6 months |
- Based on ZeNix and Nix-TB trials: 90% favourable outcome in XDR-TB (vs ~50% historical controls)
- FDA approved 2019; Strong recommendation in ATS 2025 guidelines
- ⚠️ Linezolid toxicity significant: peripheral neuropathy, myelosuppression, optic neuropathy in >60% of patients — dose reduction to 600→300 mg acceptable
C. 9-Month All-Oral Short Course ⭐ (WHO 2022)
| Phase | Drugs | Duration |
|---|---|---|
| Intensive | Bedaquiline + Levofloxacin/Moxifloxacin + Ethionamide + Ethambutol + Isoniazid (high-dose) + Pyrazinamide + Clofazimine | 4 months (6 if sputum-positive at month 4) |
| Continuation | Moxifloxacin + Clofazimine + Ethambutol + Pyrazinamide | 5 months |
| Total | 9 months |
- Replaced the old injectable-containing 9-month "Bangladesh" regimen
- All oral; shorter than previous 18–24 month regimens
- Conditional recommendation by WHO
D. Longer Individualized MDR-TB Regimen
| Priority Group | Drugs |
|---|---|
| Group A (include all if possible) | Levofloxacin or Moxifloxacin, Bedaquiline, Linezolid |
| Group B (add if needed) | Clofazimine, Cycloserine/Terizidone |
| Group C (use to complete if A+B insufficient) | Ethambutol, Delamanid, Pyrazinamide, Imipenem-Cilastatin, Amikacin (or Streptomycin), Ethionamide/Prothionamide, PAS |
- Regimen should contain at least 4 effective drugs in the intensive phase and at least 3 in the continuation phase
- Treat for 15–21 months after culture conversion (5–7 months intensive phase)
- Injectable aminoglycosides (amikacin, kanamycin) now downgraded to Group C — used only when no oral alternatives available due to ototoxicity/nephrotoxicity
E. Isoniazid Monoresistant TB
| Regimen | Duration |
|---|---|
| Rifampin + Ethambutol + Pyrazinamide + Moxifloxacin/Levofloxacin | 6 months daily |
| (Pyrazinamide may be stopped after 2 months if low disease burden) |
PART 4: TB + HIV CO-INFECTION
- Start ART within 2 weeks of TB treatment initiation if CD4 < 50/μL
- Start ART within 8–12 weeks of TB treatment if CD4 ≥ 50/μL
- Exception: TB meningitis — delay ART to reduce immune reconstitution inflammatory syndrome (IRIS) risk
- Rifampin-ART interactions: Rifampin is a strong CYP3A4 inducer — reduces levels of protease inhibitors, NNRTIs, integrase inhibitors
- Preferred ART with rifampin: efavirenz-based regimen or dolutegravir 50 mg twice daily
- Consider rifabutin (weaker inducer) instead of rifampin when using boosted PI regimens
PART 5: SPECIAL POPULATIONS
TB Meningitis
- Same 4-drug intensive phase (HRZE) for 2 months, then HR for 10 months (total 12 months)
- Add dexamethasone (0.4 mg/kg/day, tapering over 6–8 weeks) — reduces mortality
- Pyrazinamide penetrates CSF well; important component
Bone/Joint TB
- Standard 6-month HRZE/HR; some guidelines extend continuation phase to 7 months (total 9 months)
Pregnancy
- Standard HRZE/HR regimen; avoid streptomycin (ototoxicity to fetus)
- 3HP (isoniazid + rifapentine) NOT recommended in pregnancy
- Add pyridoxine (B₆) with isoniazid
Paediatric TB
- Same drug regimens as adults (weight-based dosing)
- Ethambutol: 20 mg/kg/day
- 3HP for LTBI approved for children >2 years
Summary: Regimen Quick Reference
| Category | Regimen | Duration |
|---|---|---|
| LTBI | 3HP (Isoniazid + Rifapentine) weekly | 3 months |
| LTBI | Rifampin daily | 4 months |
| DS-TB (Standard) | 2HRZE / 4HR | 6 months |
| DS-TB (New short course) | 2HPZM / 2HPM | 4 months |
| DS-TB (Cavitary/delayed) | 2HRZE / 7HR | 9 months |
| TB Meningitis | 2HRZE / 10HR + dexamethasone | 12 months |
| INH-monoresistant TB | 6 months REZM (Rifampin + EMB + PZA + Moxifloxacin) | 6 months |
| MDR/RR-TB (FQ-susceptible) ⭐ | BPaLM (Bedaquiline + Pretomanid + Linezolid + Moxifloxacin) | 6 months |
| Pre-XDR/XDR-TB (FQ-resistant) ⭐ | BPaL (Bedaquiline + Pretomanid + Linezolid) | 6 months |
| MDR-TB (9-month oral) | BDQ + FQ + Cfz + EMB + HHD + PZA + ETO | 9 months |
| XDR-TB (individualized) | Group A+B+C drugs (≥4 effective drugs) | 15–21 months |
- Daley CL et al. ATS/CDC/ERS/IDSA 2025 Updated TB Treatment Guideline. PMC11755361
- WHO Consolidated Guidelines Module 4: DR-TB Treatment, 2022 Update
- Harrison's Principles of Internal Medicine, 22nd ed., 2025
- Murray & Nadel's Textbook of Respiratory Medicine
- Nix-TB Trial (BPaL, NEJM 2020) | ZeNix Trial (NEJM 2022) | TB-PRACTECAL Trial (Lancet 2022) | Study 31/A5349 (NEJM 2021)