Status epilepticus
Reading File
Finding Sources
Searching PubMed
"status epilepticus"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Status Epilepticus
Definition
Status epilepticus (SE) is a neurological emergency defined as:
- A single seizure lasting ≥5 minutes, or
- Two or more seizures without recovery of consciousness between them
The traditional 30-minute threshold has been replaced in practice by 5 minutes for generalized tonic-clonic seizures and 10 minutes for focal impaired awareness seizures, because seizures that last longer than 5 minutes rarely terminate spontaneously and are less drug-responsive. Permanent neuronal injury is not likely unless SE persists for >30 minutes (convulsive) or >60 minutes (focal impaired awareness).
- Tintinalli's Emergency Medicine, p. 1198
- Goldman-Cecil Medicine, p. 76
Types
| Type | Key Features |
|---|---|
| Generalized convulsive SE | Bilateral rhythmic limb jerking, impaired consciousness - the most dangerous form |
| Nonconvulsive SE (NCSE) | Coma, fluctuating mental status, subtle motor signs (twitching, blinking, eye deviation), or unexplained stupor - NO overt motor activity; diagnosed by EEG |
| Absence SE | Typical, atypical, or myoclonic forms |
| Focal SE | With or without impaired consciousness; may have focal motor/sensory features |
| NCSE in coma | Often follows treatment of convulsive SE; requires continuous EEG to detect |
- Katzung's Basic and Clinical Pharmacology, p. 677
Pathophysiology
After 5 minutes of continuous seizure activity, profound changes occur:
- GABA receptor downregulation - decreased expression and internalization of GABA-A receptors
- Glutamate/NMDA receptor upregulation - dramatically lowers the seizure threshold
- Blood-brain barrier disruption - potassium and albumin (both hyperexcitatory) enter the CNS
- After 20 minutes: hypotension, hypoxia, metabolic acidosis, hyperthermia, hypoglycemia, cardiac dysrhythmias, and pulmonary edema frequently develop
This hyperexcitatory milieu explains why standard antiseizure therapies become progressively less effective the longer seizures persist.
- Tintinalli's Emergency Medicine, p. 1198
Common Causes
- Subtherapeutic antiepileptic drug levels (most common in known epileptics)
- Acute stroke or cerebrovascular disease
- CNS infection / encephalitis (autoimmune encephalitis is a leading cause in one large study)
- Traumatic brain injury
- Anoxia/hypoxia
- Metabolic abnormalities (hypoglycemia, hyponatremia, hypocalcemia)
- Alcohol or drug intoxication/withdrawal
- ~50% remain cryptogenic even after detailed evaluation
Management - Time-Based Protocol
The goal is seizure control within 30 minutes of presentation. ABCs, IV access, monitoring, and drug treatment proceed simultaneously.
Immediate (0-5 min): Supportive Care
- IV/IO access (large-bore), cardiac monitor, pulse oximetry, end-tidal capnography
- Oxygen; airway positioning; suction available
- Check point-of-care glucose; correct hypoglycemia
- Send labs: glucose, electrolytes, calcium, magnesium, CBC, LFTs, RFTs, AED levels, toxicology
- Use normal saline (phenytoin is incompatible with glucose-containing solutions)
- Treat hyperthermia with antipyretics and cooling
Phase 1 - First-Line: Benzodiazepines (target: 5-10 min)
Benzodiazepines terminate SE in ~70% of patients. Delays >10 minutes in initiating them are associated with higher mortality, longer seizure duration, and more complications.
| Drug | Route | Dose |
|---|---|---|
| Lorazepam (IV) | IV | 0.1 mg/kg at 2 mg/min (up to 2 mg, repeat once) |
| Diazepam (IV) | IV | 5-10 mg bolus at 5 mg/min (up to 10-20 mg) |
| Midazolam (IM) | IM | 10 mg (prehospital preferred; shown non-inferior to IV lorazepam) |
| Midazolam (IN/buccal) | Intranasal/buccal | If IV/IO cannot be obtained within 1-2 min |
| Clonazepam | IV | 1 mg bolus at 0.5 mg/min (used outside USA) |
Lorazepam vs. Diazepam: Lorazepam is less lipophilic, redistributes less rapidly to peripheral fat, and has a longer effective CNS duration. Despite the pharmacokinetic advantage, clinical data do not conclusively favor one over the other.
A second benzodiazepine dose should only be given after 5 minutes of continued seizure following the first dose.
Phase 2 - Second-Line: Established SE (10-30 min)
If seizures continue 5 minutes after the second benzodiazepine dose, load a second-line agent. All three options below are approximately equally effective (~45-50% seizure cessation after benzodiazepine failure):
| Drug | Dose | Rate | Notes |
|---|---|---|---|
| Fosphenytoin | 15-20 mg PE/kg | 150 mg PE/min IV | Water-soluble; can be given IM; less cardiotoxic and less sclerosing than phenytoin; 3x faster infusion |
| Phenytoin | 20 mg/kg | 50 mg/min IV | Must use normal saline; cardiac monitoring required |
| Valproate | 30-40 mg/kg | 5 mg/kg/min IV | Contraindicated with liver disease, thrombocytopenia, suspected metabolic disease |
| Levetiracetam | 30-60 mg/kg (2000-4000 mg) | Over 10 min | Favorable adverse-effect profile; may have improved efficacy vs. phenytoin in some trials |
| Lacosamide | IV loading | Standard | ECG monitoring needed (PR interval prolongation, arrhythmia risk) |
| Phenobarbital | 10 mg/kg | 100 mg/min | Highly effective but causes severe sedation, respiratory depression, and hypotension |
Phase 3 - Refractory SE: ICU (>30 min after Phase 1 + 2 failure)
Refractory SE requires ICU admission, endotracheal intubation, and continuous EEG monitoring (especially if paralyzed). Use continuous IV infusion of anesthetic agents:
| Agent | Dose |
|---|---|
| Midazolam | Load 0.2 mg/kg; infusion 0.05-2 mg/kg/h |
| Propofol | 1 mg/kg IV, then 1-10 mg/kg/h |
| Ketamine | 2.2-5 mg/kg/h (NMDA antagonist; useful in highly refractory cases; preferred if intubating due to antiseizure properties) |
| Pentobarbital | 0.5-3 mg/kg/h |
| Thiopental | 3-5 mg/kg/h |
Note on intubation: If intubating, use a short-acting neuromuscular blocker (e.g., succinylcholine) to allow monitoring of ongoing seizure activity, and select a sedative with antiepileptic activity (propofol or ketamine). Arrange continuous EEG after paralytic use.
Therapeutic hypothermia is not beneficial in SE.
Treatment Flowchart
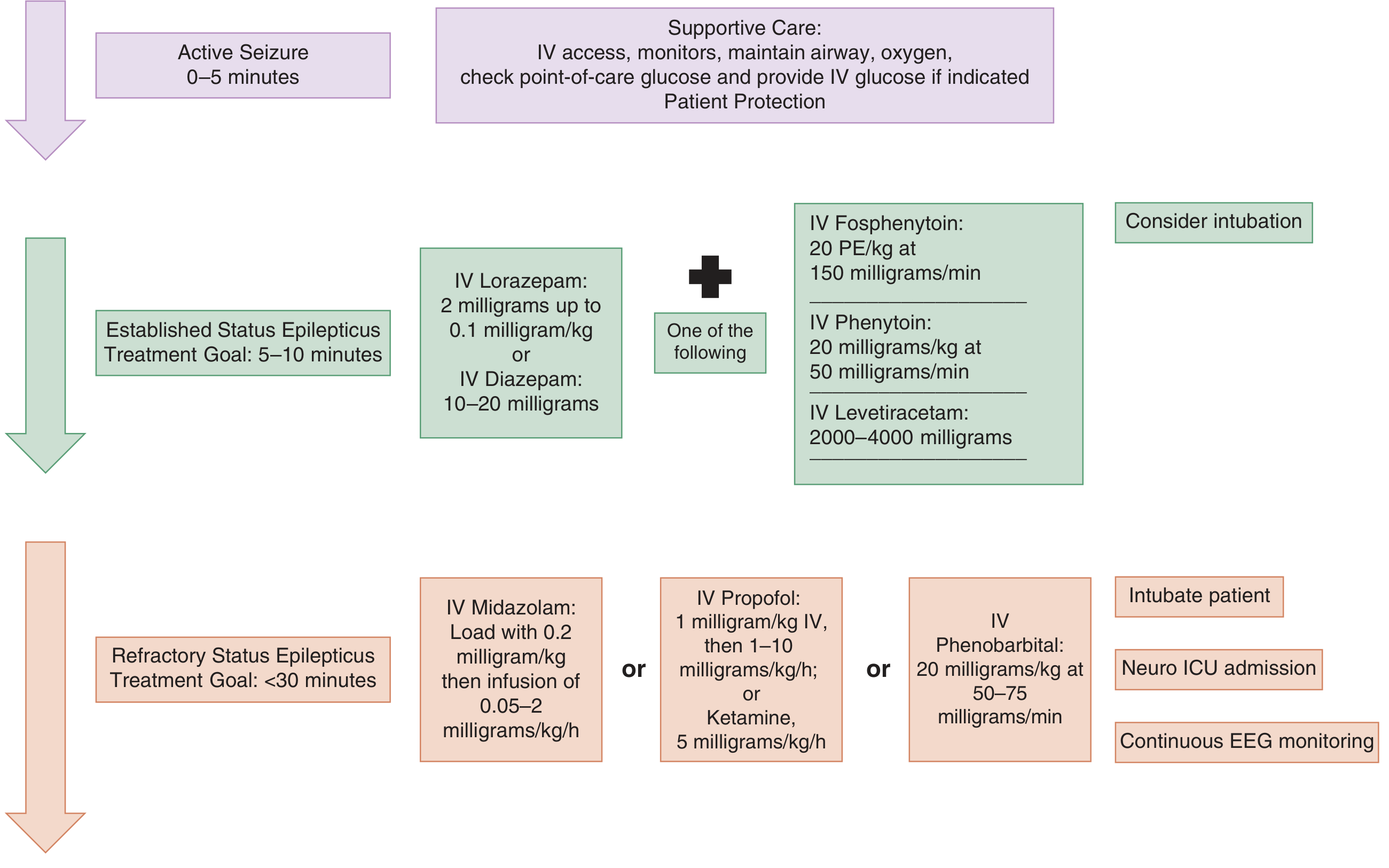
From Tintinalli's Emergency Medicine - Management of active seizures and status epilepticus
Nonconvulsive SE - Special Considerations
- Clinically subtle: prolonged postictal state, twitching/blinking, eye deviation, fluctuating consciousness, unexplained coma
- Diagnosis requires EEG
- Less urgency than convulsive SE; therapy can be started more cautiously with lower initial doses
- High suspicion warranted after convulsive SE appears to stop clinically (may evolve to NCSE)
Pediatric Dosing (Diazepam as example)
| Age | IV Dose |
|---|---|
| Neonate | 0.1-0.3 mg/kg/dose Q15-30 min; max total 2 mg |
| Child 1 mo - <5 yr | 0.2-0.5 mg/dose Q2-5 min; max total 5 mg |
| Child ≥5 yr | 1 mg/dose Q2-5 min; max total 10 mg |
| Adult | 5-10 mg/dose Q10-15 min; max 30 mg per 8-hr period |
- Harriet Lane Handbook, p. 1108
Recent Evidence (2024-2026)
A 2026 systematic review in J Neurol (PMID 41838218) evaluated brivaracetam as an emerging option for SE. A 2024 meta-analysis in Epilepsia (PMID 38881333) confirmed ketamine has meaningful evidence supporting its use in pediatric refractory SE. These agents may expand the armamentarium but are not yet first- or second-line in major guidelines.
Key Mnemonics:
- "5 is the new 30": treat at 5 minutes, not 30
- "BZD → Second-line → ICU anesthesia": three-phase escalation
- "NCSE hides": always consider EEG in unexplained coma or prolonged postictal state
This is a shared conversation. Sign in to Orris to start your own chat.