
photo-1784094129700.jpg
Answers
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Q1. Lacrimal Apparatus - Diagram & Diseases
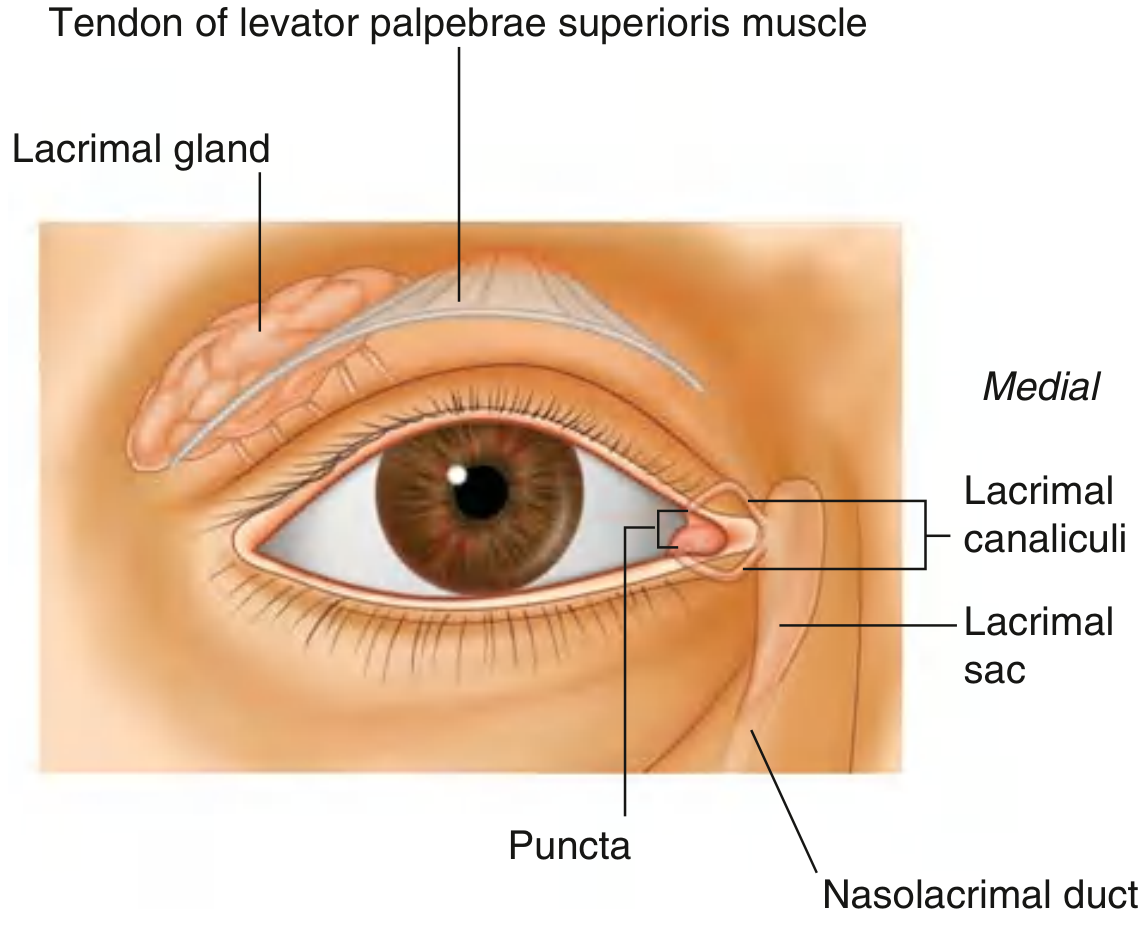
Diagram of the Lacrimal Apparatus
Anterior View:
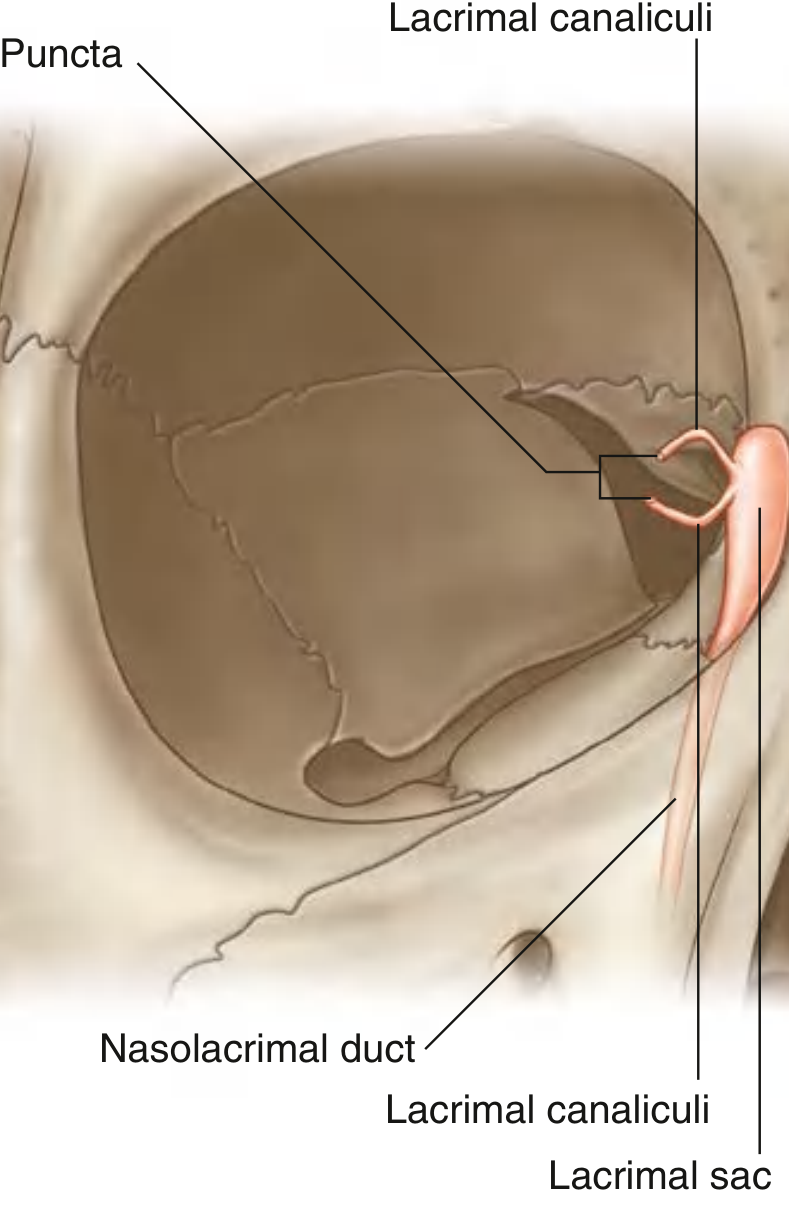
Medial view (Lacrimal Sac detail):
Components of the Lacrimal Apparatus
The lacrimal apparatus is involved in the production, movement, and drainage of fluid from the surface of the eyeball. It consists of:
| Component | Description |
|---|---|
| Lacrimal gland | Situated anteriorly in the superolateral orbit; divided into orbital part (larger, in lacrimal fossa of frontal bone) and palpebral part (smaller, below levator palpebrae superioris) |
| Lacrimal ducts | Numerous ducts empty secretions into the lateral superior conjunctival fornix |
| Lacrimal lake | Fluid accumulates medially at the medial canthus |
| Lacrimal puncta | Openings (one on each eyelid margin) through which fluid enters the canaliculi |
| Lacrimal canaliculi | Upper and lower canaliculi carry tears medially to the lacrimal sac |
| Lacrimal sac | Lies between anterior and posterior lacrimal crests; tears drawn in during blinking by the lacrimal part of orbicularis oculi |
| Nasolacrimal duct | Drains tears from the lacrimal sac into the inferior meatus of the nasal cavity |
Flow of tears: Lacrimal gland → conjunctival fornix → across ocular surface (lateral to medial) → lacrimal lake → puncta → canaliculi → lacrimal sac → nasolacrimal duct → inferior nasal meatus
(Gray's Anatomy for Students, p. 1072)
Diseases of the Lacrimal Apparatus
1. Dacryoadenitis
- Acute: Inflammation of the lacrimal gland; caused by viral (mumps, EBV, herpes) or bacterial infection. Presents with pain, swelling, and tenderness in the superolateral orbit with an S-shaped ptosis.
- Chronic: Associated with sarcoidosis, lymphoma, Sjogren syndrome, or tuberculosis.
2. Dacryocystitis
- Inflammation of the lacrimal sac, most often due to obstruction of the nasolacrimal duct.
- Acute: Red, painful swelling at the medial canthus; may form an abscess. Causative organisms: Staphylococcus aureus, Streptococcus pneumoniae.
- Chronic: Persistent epiphora (watering eye), mucopurulent discharge; regurgitation on pressure over the sac is diagnostic.
- Treatment: Acute - antibiotics + incision/drainage; Chronic - dacryocystorhinostomy (DCR).
3. Epiphora (Watery Eye)
- Excessive tearing due to either overproduction or impaired drainage (punctal eversion, canalicular block, nasolacrimal duct obstruction).
4. Nasolacrimal Duct Obstruction (NLDO)
- Congenital NLDO: Most common in neonates; due to failure of canalization of the valve of Hasner at the lower end. Presents with sticky/watery eye. Most resolve spontaneously. Probing is curative if persistent.
- Acquired NLDO: Age-related fibrosis or secondary to trauma, infection (chlamydial), tumors.
5. Canaliculitis
- Infection of the lacrimal canaliculus; usually caused by Actinomyces israelii (filamentous organism).
- Presents with medial lid swelling, foamy/purulent discharge, pouting of the punctum.
6. Dry Eye Syndrome (Keratoconjunctivitis Sicca)
- Deficiency of the aqueous layer of the tear film due to lacrimal gland dysfunction.
- Associated with Sjogren syndrome, rheumatoid arthritis, post-radiation.
Q2. Examination of Eyelid & Diseases of Eyelid
Examination of the Eyelid
A. History: Duration, symptoms (itching, burning, discharge, pain, mass), previous treatments.
B. General Inspection
- Position: Look for ptosis (drooping), ectropion (eversion), entropion (inversion), lagophthalmos (inability to close)
- Lid skin: Redness, crusting, scaling, masses, lesions
- Lid margins: Position of lashes (trichiasis/distichiasis), meibomian gland orifices, punctal position
C. Systematic Eyelid Examination
- Upper eyelid: Check for ptosis - measure palpebral fissure height (normal ~9-10 mm), levator function (normal >12 mm excursion)
- Lower eyelid: Check for ectropion (outward turn), entropion (inward turn)
- Eyelashes: Trichiasis (misdirected lashes rubbing cornea), madarosis (loss of lashes)
- Eyelid margin: Blepharitis - anterior (at lash base) or posterior (meibomian gland dysfunction)
- Tarsal conjunctiva: Evert upper lid to inspect for follicles, papillae, foreign bodies, scarring
- Meibomian glands: Palpate for chalazion; express secretions - clear (normal) vs. toothpaste-like (MGD)
- Skin: Look for vesicles (herpes), erythema, indurated mass (BCC, SCC)
Eversion of the upper eyelid:
- Patient looks down; grasp lashes; press cotton bud on upper tarsal fold; fold lid over the bud.
- Allows examination of tarsal conjunctiva, papillae, follicles.
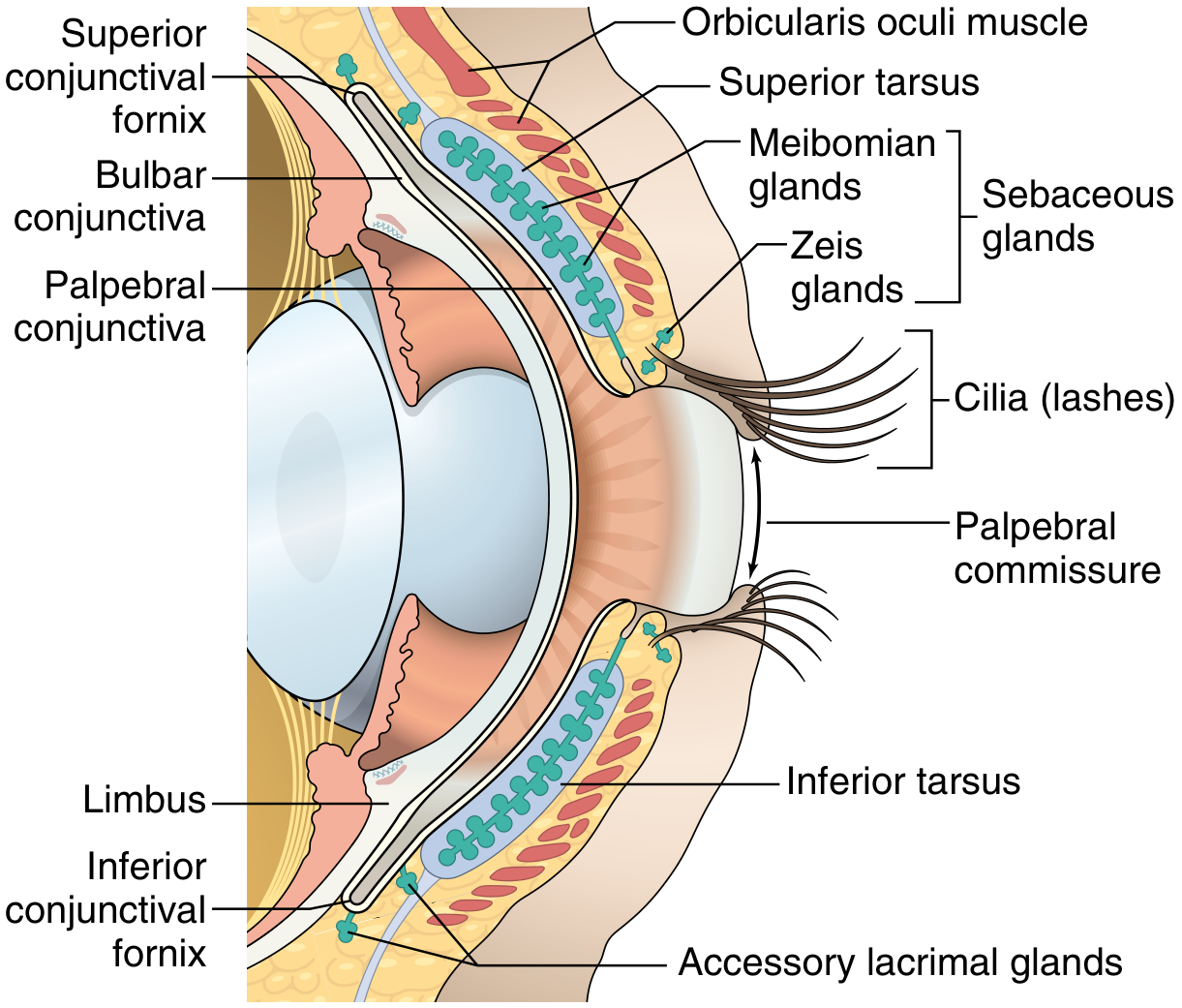
Diagram - Anatomy of the Eyelid & Conjunctiva:
Diseases of the Eyelid
Inflammatory Conditions
| Disease | Features |
|---|---|
| Blepharitis | Chronic lid margin inflammation; Anterior (staphylococcal/seborrhoeic): scales/crusts at lash bases; Posterior (meibomian gland dysfunction): thickened, plugged gland orifices; frothy tear film |
| Stye (External Hordeolum) | Acute staphylococcal infection of Zeis or Moll glands; painful red swelling at lid margin near a lash |
| Chalazion (Internal Hordeolum) | Chronic sterile lipogranuloma from obstruction of a Meibomian gland ductule. Firm, painless nodule away from the lid margin. Biopsy to exclude sebaceous carcinoma if recurrent |
| Cellulitis | Pre-septal (anterior to orbital septum) vs. orbital (posterior); pre-septal often from local skin trauma; orbital presents with proptosis, restricted EOM, pain on movement - requires urgent IV antibiotics |
Lid Malpositions
| Condition | Description |
|---|---|
| Ptosis | Drooping of upper eyelid. Congenital (levator dysgenesis), myogenic (myasthenia gravis, CPEO), neurogenic (CNIII palsy, Horner syndrome), aponeurotic (age-related). Tested by measuring levator function and MRD (margin reflex distance) |
| Entropion | Inward turning of the lid margin; lashes abrade the cornea. Most common in elderly (involutional). Also cicatricial (post-trachoma), congenital. Causes corneal ulceration if untreated |
| Ectropion | Outward turning of the lid margin; leads to epiphora and exposure keratopathy. Most common in elderly (involutional). Also cicatricial, paralytic (CN VII palsy), or mechanical |
| Lagophthalmos | Inability to fully close the eyelid; exposure keratitis results. Cause: CN VII palsy, proptosis |
| Trichiasis | Misdirected eyelashes rubbing the cornea; causes irritation, corneal scarring. Treatment: epilation, cryotherapy, laser |
Eyelid Neoplasms
| Tumour | Key Features |
|---|---|
| Basal Cell Carcinoma (BCC) | Most common eyelid malignancy; predilection for lower lid and medial canthus. Pearly rolled edges, central ulceration ("rodent ulcer"). Locally invasive but rarely metastasizes |
| Sebaceous Carcinoma | Arises from Meibomian glands; may mimic chronic blepharitis or chalazion ("masquerade syndrome"). Pagetoid spread. High mortality if missed (22%). Biopsy any recurrent chalazion |
| Squamous Cell Carcinoma | Less common; solar-damaged skin; can metastasize |
| Melanoma | Very rare in eyelid skin |
| Kaposi Sarcoma | Purple lesion in AIDS patients |
Other Notable Conditions
- Dermatochalasis: Redundant, baggy eyelid skin due to aging; may cause superior visual field loss
- Blepharospasm: Involuntary forceful contraction of orbicularis oculi; treated with botulinum toxin (Botox)
- Xanthelasma: Yellow lipid plaques on medial eyelid skin; associated with hyperlipidaemia
- Herpes Zoster Ophthalmicus: Involvement of tip of nose (Hutchinson sign) indicates nasociliary nerve involvement and high risk of ocular complications; treat with systemic aciclovir
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1206; Textbook of Family Medicine, p. 368)
Q3. Examination of Conjunctiva & Diseases of Conjunctiva
Examination of the Conjunctiva
Anatomy: The conjunctiva is a transparent mucous membrane divided into:
- Palpebral conjunctiva: Lines the inner surface of upper and lower lids; firmly attached to tarsal plates; vertically oriented blood vessels
- Fornical conjunctiva: Loose and redundant; forms upper and lower fornices
- Bulbar conjunctiva: Covers anterior sclera; continuous with corneal epithelium at the limbus; contains palisades of Vogt (corneal stem cell reservoir)
- Plica semilunaris: Nasal fold; medial to which lies the caruncle (modified cutaneous tissue)
Steps in Conjunctival Examination:
- Inspect bulbar conjunctiva: Look for injection (hyperaemia), chemosis (oedema), haemorrhage, follicles, papillae, symblepharon, pterygium, pinguecula
- Inspect lower palpebral conjunctiva: Pull down lower lid; look for follicles, papillae, discharge, foreign body
- Evert upper eyelid: Inspect upper tarsal conjunctiva - follicles (e.g., viral, chlamydia) vs. papillae (e.g., allergic, GPC)
- Classify discharge: Watery (viral), mucoid (allergic), mucopurulent (bacterial), purulent (gonococcal)
- Staining: Rose Bengal or lissamine green highlights devitalized epithelium; fluorescein shows corneal epithelial defects
- Conjunctival swab/scraping: For culture and cytology (intracytoplasmic inclusions in chlamydial infection; multinucleate giant cells in viral)
Key Signs:
- Follicles: Lymphoid aggregates (no central vessels); seen in viral/chlamydial conjunctivitis; lower fornix predominantly
- Papillae: Vascular tufts with fibrous septa (central vessels); seen in bacterial, allergic, GPC; cobblestone papillae in vernal keratoconjunctivitis
- Chemosis: Conjunctival oedema; seen in severe allergic or bacterial conjunctivitis
- Symblepharon: Adhesion between palpebral and bulbar conjunctiva; seen in cicatricial pemphigoid, Stevens-Johnson syndrome
Diseases of the Conjunctiva
1. Conjunctivitis (Classification)
By aetiology:
| Type | Features | Discharge | Treatment |
|---|---|---|---|
| Bacterial (Staph, Strep, H. influenzae) | Acute onset; bilateral; papillae; mucopurulent discharge; lids glued in morning | Mucopurulent | Topical antibiotics (chloramphenicol, moxifloxacin) |
| Gonococcal (N. gonorrhoeae) | Hyperacute, profuse purulent discharge, marked chemosis; can perforate cornea in 24h | Copious purulent | IV ceftriaxone + topical |
| Chlamydial (Trachoma / inclusion) | Most common cause of preventable blindness worldwide (Trachoma). Follicles on upper tarsal plate, pannus, Herbert pits at limbus. Graded by WHO (TF, TI, TS, TT, CO) | Mucopurulent | Oral azithromycin single dose |
| Viral (Adenovirus most common) | Highly contagious; follicles; watery discharge; pre-auricular lymphadenopathy; pseudomembranes in severe epidemic keratoconjunctivitis (EKC) | Watery | Supportive; cold compresses |
| Neonatal (Ophthalmia Neonatorum) | Within first 28 days of life. Gonococcal (day 1-3), Chlamydial (day 5-14), Chemical (silver nitrate, day 1) | - | As per aetiology; prophylaxis at birth |
| Allergic (Seasonal/Perennial) | Bilateral; intense itching; papillae; ropy mucoid discharge; chemosis | Mucoid/ropy | Antihistamines, mast cell stabilizers |
| Vernal Keratoconjunctivitis (VKC) | Seasonal; young males; giant cobblestone papillae on upper tarsal plate; shield ulcer; Horner-Trantas dots at limbus | Ropy mucoid | Topical steroids, cyclosporine |
| Atopic Keratoconjunctivitis (AKC) | Perennial; older adults; associated with atopic dermatitis; can cause severe scarring | - | Topical steroids, immunomodulators |
2. Cicatricial Conditions
- Ocular Cicatricial Pemphigoid: Autoimmune; progressive scarring; symblepharon, forniceal shortening, dry eye, corneal opacification. Treatment: systemic dapsone, azathioprine, or mycophenolate mofetil
- Stevens-Johnson Syndrome / Toxic Epidermal Necrolysis: Drug-induced (sulfonamides, anticonvulsants); bilateral acute conjunctivitis progressing to severe scarring, symblepharon, corneal opacification. Conjunctival membranes form acutely
- Trachoma: Leading infectious cause of blindness; caused by Chlamydia trachomatis serovars A-C; transmitted by flies and direct contact
3. Degenerative Conditions
| Condition | Description |
|---|---|
| Pterygium | Wing-shaped fibrovascular growth from bulbar conjunctiva encroaching onto the cornea; usually nasal; associated with UV exposure; causes astigmatism and vision obstruction |
| Pinguecula | Yellowish-white conjunctival deposit of elastotic degeneration lateral/medial to the limbus; does not invade the cornea |
| Conjunctivochalasis | Redundant loose bulbar conjunctiva; causes epiphora and irritation in elderly |
| Concretions | Calcium deposits in palpebral conjunctiva; common in elderly; cause foreign body sensation |
4. Subconjunctival Haemorrhage
- Bright red, flat, well-demarcated bleed beneath the bulbar conjunctiva
- Causes: straining, coughing, Valsalva, trauma, anticoagulants, hypertension
- Usually resolves in 1-2 weeks without treatment; investigate BP and coagulation if recurrent
5. Tumours of the Conjunctiva
- Squamous cell carcinoma / CIN (Ocular Surface Squamous Neoplasia): Most common conjunctival malignancy; at limbus; associated with HPV and UV exposure
- Melanoma: From PAM (Primary Acquired Melanosis) with atypia; aggressive; poor prognosis
- Lymphoma: Usually MALT type; pink "salmon patch" appearance
- Kaposi Sarcoma: In HIV/AIDS patients
Sources: Gray's Anatomy for Students; Kanski's Clinical Ophthalmology 10th ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.