Explain pancreatitis
Reading File
Finding Sources
Searching PubMed
"pancreatitis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Pancreatitis
Pancreatitis is inflammation of the pancreas, ranging from mild self-limited disease to life-threatening multiorgan failure. It is the most common pancreatic disease worldwide and a leading GI cause of hospitalization in the United States.
Anatomy of the Pancreas
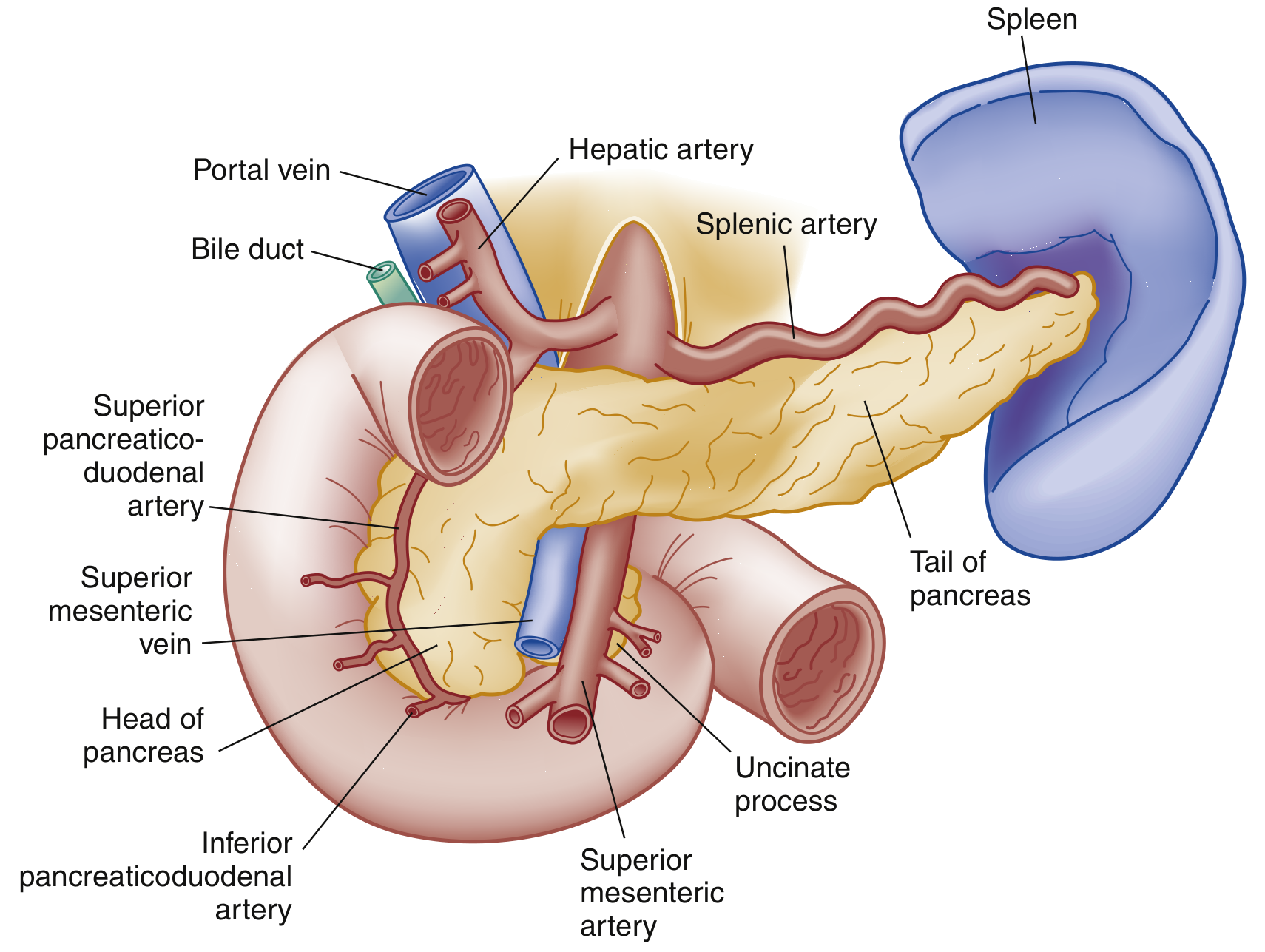
Pancreatic anatomy, anterior view - Rosen's Emergency Medicine
The pancreas is a retroperitoneal organ with three segments:
- Head - sits within the duodenal C-loop; the main pancreatic duct (duct of Wirsung) joins the common bile duct here to form the ampulla of Vater, draining via the sphincter of Oddi
- Body - traverses posterior to the stomach
- Tail - abuts the splenic hilum
Exocrine function: secretes digestive enzymes (e.g., trypsinogen, lipase, amylase) into the duodenum
Endocrine function: secretes insulin, glucagon, and somatostatin
Pathophysiology
Injury begins with an inciting event (gallstone obstruction, alcohol, drugs, etc.) that disrupts normal membrane trafficking in acinar cells. This triggers:
- Inappropriate activation of trypsinogen → trypsin within the gland
- Trypsin activates other digestive enzymes, causing autodigestion of pancreatic tissue
- Macrophage and neutrophil recruitment amplify destruction
- Cytokine release increases vascular permeability → edema, hemorrhage, and necrosis
- A heightened systemic inflammatory response can cause SIRS → sepsis → shock
- Bacteremia may occur via translocation of intestinal flora through a compromised gut barrier
- Extrapancreatic complications include pleural effusions, ARDS, and renal failure
- Rosen's Emergency Medicine, p. 1265
Causes
| Category | Examples |
|---|---|
| Toxic-Metabolic (most common) | Alcohol (25-35%), drugs, hypertriglyceridemia, hypercalcemia, uremia |
| Mechanical-Obstructive (most common) | Gallstones (40-70%), post-ERCP, pancreas divisum, ampullary tumors, trauma |
| Infectious | Viral (mumps, coxsackie, CMV, EBV, HIV); bacterial (TB, Mycoplasma, Salmonella); parasitic (Ascaris) |
| Vascular | Vasculitis, embolism, ischemia, hypercoagulability |
| Other | Idiopathic, hereditary/genetic (SPINK1, CFTR mutations), autoimmune, DKA |
Together, gallstones and alcohol account for ~65-80% of all adult cases.
- Rosen's Emergency Medicine, Box 77.1, p. 1266
Types
1. Acute Pancreatitis (AP)
Sudden inflammatory disease with enzymatic autodigestion. Most episodes are interstitial edematous (resolves within 1 week). Approximately 5-10% develop necrotizing pancreatitis, where the parenchyma and surrounding tissue undergo necrosis - this can remain sterile, liquefy, or become infected, with infected necrosis carrying significantly higher morbidity.
2. Chronic Pancreatitis (CP)
Progressive, permanent damage to pancreatic tissue, usually visible as calcifications on X-ray and CT. Leads to exocrine insufficiency (malabsorption, steatorrhea), endocrine insufficiency (diabetes), and a chronic pain syndrome. Often related to ongoing alcohol use. Many patients develop pseudocysts, ascites, fistulae, and mesenteric venous thrombosis.
- Textbook of Family Medicine, p. 1139
Clinical Features of Acute Pancreatitis
Symptoms:
- Persistent epigastric or LUQ pain radiating to the back, chest, or flanks
- Pain is moderate to severe; classically relieved by sitting forward or leaning ahead
- Nausea, vomiting, and anorexia (oral intake worsens pain)
Signs:
- Vital signs may be normal in mild disease; tachycardia and fever are common
- Jaundice suggests biliary obstruction (gallstone pancreatitis or tumor)
- Shallow respirations, basilar crackles (pulmonary complications)
- Epigastric tenderness with guarding; absent bowel sounds (ileus)
- Cullen sign - bluish periumbilical discoloration (hemoperitoneum) - rare but poor prognosis
- Grey Turner sign - reddish-brown flank discoloration (retroperitoneal bleeding) - rare but poor prognosis
Systemic complications:
-
Pulmonary: pleural effusions (in up to 50%, more often left-sided), atelectasis, ARDS
-
Cardiovascular: hypotension, shock from fluid shifts
-
Renal: failure from hypoperfusion and inflammatory mediators
-
Metabolic: hyperglycemia (decreased insulin), hypocalcemia (from low albumin/magnesium), coagulopathy/DIC
-
Rosen's Emergency Medicine, pp. 1265-1266
Diagnosis
Diagnosis requires at least 2 of 3 criteria (Atlanta criteria):
- Abdominal pain characteristic of acute pancreatitis
- Serum lipase or amylase ≥ 3× the upper limit of normal
- Characteristic findings on abdominal imaging
Laboratory:
- Lipase - preferred; more sensitive and specific than amylase; rises within hours, remains elevated for 1-2 weeks
- Amylase - less specific (also elevated in renal failure, salivary gland disease, cholecystitis, bowel obstruction); stays elevated for 3-5 days
- CBC (leukocytosis), metabolic panel (renal function, LFTs, calcium, glucose), lipid panel
- Note: normal enzyme levels do not exclude pancreatitis in alcohol-related cases
Imaging:
- CT abdomen with contrast - gold standard for severity assessment; shows peripancreatic fat stranding, fluid collections, and necrosis
- Ultrasound - first-line to detect gallstones as etiology; limited for pancreas visualization
- MRCP/MRI - useful to evaluate pancreatic/biliary ducts without radiation
- Plain films and chest X-ray are supportive (may show ileus, pleural effusions, "colon cut-off sign")
Severity Classification (Revised 2012 Atlanta Classification)
| Grade | Criteria |
|---|---|
| Mild | No organ failure; no local or systemic complications |
| Moderately Severe | Transient organ failure (<48 h) OR local/systemic complications |
| Severe | Persistent organ failure (>48 h); modified Marshall score ≥2 for respiratory, cardiovascular, or renal systems |
Note: severe classification cannot be assigned until 48 hours after presentation.
Scoring systems: Ranson criteria (uses admission + 48-hour labs to predict mortality), APACHE II, BISAP score, and CT Severity Index (CTSI) are all used.
- Rosen's Emergency Medicine, Box 77.4, p. 1268
Local Complications
| Setting | Complication | Timing |
|---|---|---|
| Interstitial edematous AP | Acute peripancreatic fluid collection | <4 weeks |
| Interstitial edematous AP | Pancreatic pseudocyst (well-defined wall) | >4 weeks |
| Necrotizing AP | Acute necrotic collection | <4 weeks |
| Necrotizing AP | Walled-off necrosis (well-defined wall) | >4 weeks |
Other late complications: splenic/portal vein thrombosis, GI bleeding, gastric outlet obstruction, bowel necrosis.
Management
Acute Pancreatitis
Supportive care is the cornerstone:
- Fluid resuscitation - aggressive IV hydration (Lactated Ringer's preferred); corrects hypovolemia, maintains pancreatic perfusion, and limits SIRS progression
- Analgesia - IV opioids for pain control (no evidence that any opioid worsens pancreatitis)
- NPO vs. early enteral nutrition (EN):
- Historical practice of NPO (to "rest the pancreas") is no longer standard
- Mild-moderate AP: oral diet should be offered as tolerated; EN considered only if diet cannot be advanced after 4 days
- Severe AP with SIRS/ICU admission: nasogastric (NG) or nasojejunal (NJ) tube feeding should be initiated within 24-36 hours
- Two meta-analyses show EN vs. parenteral nutrition (PN) provides a ~2-fold reduction in infectious complications and a ~2.5-fold reduction in mortality risk
- The AGA technical review of 12 RCTs confirms EN reduces infected peripancreatic necrosis (OR 0.28), single organ failure (OR 0.25), and multiorgan failure (OR 0.41)
- Antibiotics - NOT routinely indicated; reserved for confirmed infected necrosis or other bacterial complications
- ERCP with sphincterotomy - indicated within 24-48 hours for gallstone pancreatitis with concurrent cholangitis or biliary obstruction
Chronic Pancreatitis
-
Pain management: analgesics, antioxidants (selenium, ascorbic acid, β-carotene, vitamin E - evidence mixed), nerve blocks, ERCP, or surgery for selected patients
-
Exocrine insufficiency: pancreatic enzyme replacement with each meal
-
Endocrine insufficiency: insulin therapy for diabetes
-
Alcohol abstinence - essential; continued use drives recurrent attacks
-
Jejunal feeding can improve weight and reduce pain in malnourished patients
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 2935-2941
Differential Diagnosis
Acute pancreatitis must be distinguished from:
- Abdominal: peptic ulcer disease, acute cholecystitis/cholangitis, bowel obstruction, mesenteric ischemia, perforated viscus, ruptured AAA, ectopic pregnancy
- Cardiopulmonary: myocardial infarction, pneumonia, pericarditis
- Systemic: DKA, sickle cell crisis
Key Points
- Gallstones and alcohol together cause ~65-80% of cases
- Lipase is preferred over amylase (more sensitive and specific)
- Atlanta 2012 classifies severity as mild/moderately severe/severe based on organ failure duration
- Early enteral nutrition in severe AP is strongly preferred over parenteral nutrition
- Antibiotics are NOT routinely given - only for infected necrosis
- Chronic pancreatitis causes irreversible damage, malabsorption, and diabetes
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 77
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.