Bleeding polyposis septum
Reading File
Finding Sources
Finding Sources
Searching PubMed
nasal septum polyposis bleeding
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a thorough summary of bleeding nasal polyposis / septum (i.e., epistaxis in the context of nasal polyps and septal pathology), drawn from the medical library:
Bleeding Nasal Polyposis and Septal Bleeding (Epistaxis)
Anatomy of the Septal Blood Supply
The nasal septum receives blood from three arterial systems that anastomose at Kiesselbach's area (also called Little's area) on the anteroinferior septum:
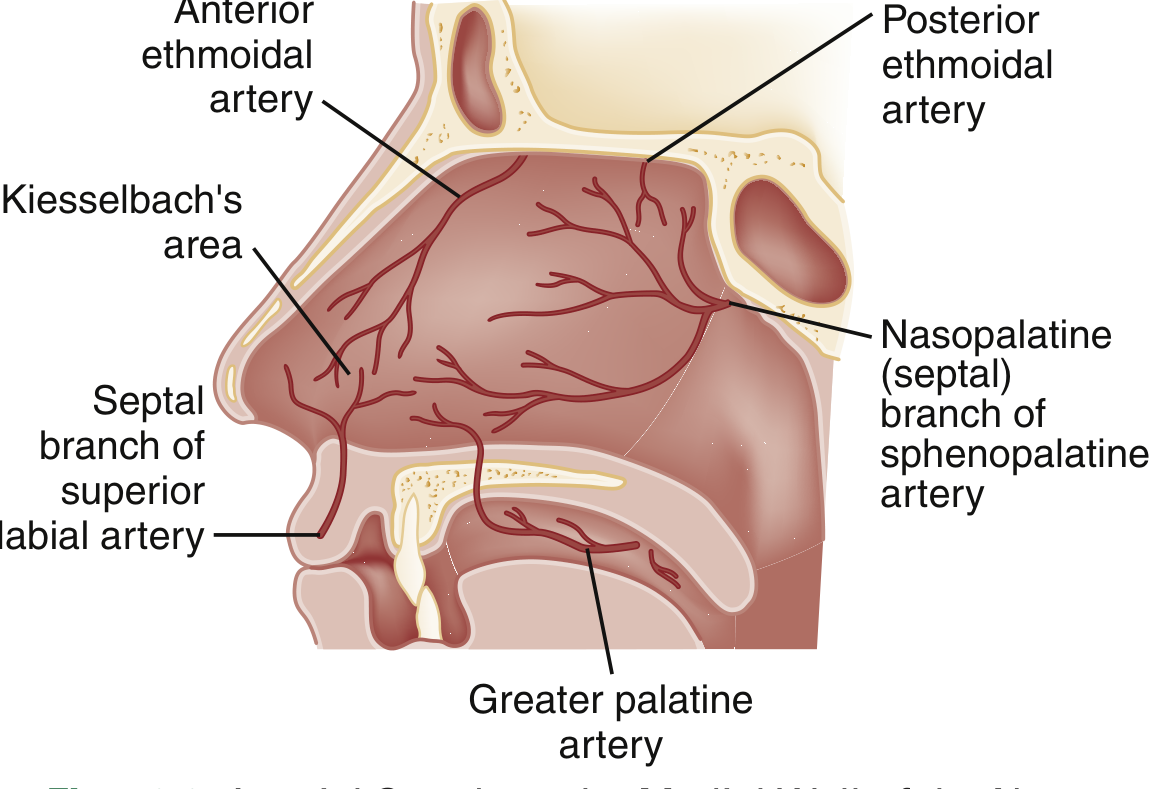
- Sphenopalatine artery - supplies the posterior and inferior septum (responsible for most severe posterior epistaxis)
- Anterior and posterior ethmoidal arteries (from the ophthalmic branch of the internal carotid) - supply the superior mucosa
- Superior labial branch of the facial artery - supplies the anterior mucosal septum
~90% of all nosebleeds are anterior, arising from Kiesselbach's plexus on the anteroinferior septum. Posterior epistaxis accounts for ~10% and is more severe, mostly in older adults.
Causes of Bleeding in Nasal Polyposis / Septal Disease
Nasal polyps themselves are listed as a direct cause of epistaxis. A deviated nasal septum also predisposes to bleeding - "Bleeding is not unusual on either side of a deviated nasal septum" (Pfenninger & Fowler's Procedures for Primary Care).
Key predisposing and associated causes include:
| Category | Examples |
|---|---|
| Structural | Nasal polyps, deviated septum, nasal foreign body |
| Inflammatory/Infectious | URI (mucosal vasodilation), allergies, rhinosinusitis |
| Vascular | Hereditary hemorrhagic telangiectasia (HHT/Osler-Weber-Rendu), telangiectasias |
| Neoplastic | Juvenile nasopharyngeal angiofibroma (adolescent boys with recurrent epistaxis + obstruction), malignancy |
| Medications | Anticoagulants (warfarin, heparin), antiplatelets (aspirin, clopidogrel), intranasal corticosteroids (can cause epistaxis/perforation), cocaine |
| Systemic | Coagulopathies, hepatic disease, hematologic malignancy, vitamin K deficiency |
| Environmental | Dry air, low humidity, cold weather |
Special note: Adolescent boys with recurrent epistaxis AND nasal obstruction should be evaluated for juvenile nasopharyngeal angiofibroma - a benign but locally aggressive tumor.
Clinical Assessment
- Vital signs and airway - rare but possible compromise in severe bleeding
- History - timing, frequency, laterality, trauma, medications (anticoagulants are a major risk factor for recurrence), comorbidities
- Hypertension - commonly elevated during epistaxis due to anxiety; no proven causal relationship, but may be associated with persistent bleeding
- Physical exam - have the patient blow the nose, then compress the cartilaginous nose for 10-15 min; examine with nasal speculum opened vertically (not laterally, to avoid obscuring the septum); oxymetazoline 0.05% (2 sprays) before pressure optimizes hemostasis and exam
Imaging and labs are not routinely indicated. Reserve coagulation studies for patients on anticoagulants, severe hemorrhage, or significant underlying conditions (liver disease, hematologic malignancy).
Management - Step-by-Step
Step 1: First Aid / Pressure
- Bilateral compression of the cartilaginous septum for 10-15 minutes
- 2 sprays oxymetazoline 0.05% into the affected naris before pressure
- A nose clip is superior to manual pressure alone
Step 2: Identify and cauterize the source
- Apply topical anesthetic: 2% lidocaine + vasoconstrictive agent (e.g., 4% lidocaine + phenylephrine)
- Silver nitrate cautery - first-line if bleeding site is visible; effective with low re-bleeding rate
- Cauterize from periphery to center, superior to inferior
- Limit contact to <15 seconds to avoid septal damage
- Do NOT apply bilaterally to the septum - may devascularize the septum and cause necrosis
Step 3: Topical hemostatic agents
- Absorbable gelatin sponge (Gelfoam)
- Absorbable knitted fabric (Surgicel)
- Topical tranexamic acid (500 mg IV solution applied to a nasal pledget or atomized) - moderate-quality evidence supports reduction in bleeding at 10 minutes and re-bleeding at 7-10 days; superior to anterior nasal packing in antiplatelet drug users
Step 4: Anterior nasal packing
- Polyvinyl acetal tampons (e.g., Merocel) or inflatable nasal balloons (e.g., Rapid Rhino - coated in procoagulant)
- Inserted along the floor of the nose, inflated with air
- For uncontrolled anterior bleeding: insert a second tampon into the opposite naris
Step 5: Posterior packing (if anterior packing fails)
- Double balloon catheter device - posterior balloon inflated first, seated by pulling anteriorly, then anterior balloon inflated slowly
- Alternative: Foley catheter into nasopharynx with 5-7 mL water in balloon, pulled anteriorly
Step 6: Specialist intervention
- Surgical ligation - traditional choice for intractable bleeding
- Endovascular embolization - success rate >80%; preferred in chronic coagulopathies and anticoagulated patients who cannot interrupt therapy
Key Considerations for Polyp-Associated Bleeding
- Nasal polyps are a recognized cause of epistaxis (listed in Box 58.6 of Rosen's Emergency Medicine)
- Polyps cause mucosal fragility and increased vascularity - any trauma or inflammation can trigger bleeding
- In HHT (hereditary hemorrhagic telangiectasia), recurrent septal bleeding is a hallmark; treatments include estrogen therapy, tamoxifen, thalidomide, and dermoplasty of the bleeding nasal septum
- Intranasal corticosteroids (used to treat nasal polyposis) can themselves cause epistaxis and, rarely, septal perforation
- Always consider malignancy (inverted papilloma, squamous cell carcinoma, lymphoma) when bleeding polyps are present, especially if unilateral or recurrent
Sources: Rosen's Emergency Medicine, 9e | Textbook of Family Medicine, 9e | Pfenninger & Fowler's Procedures for Primary Care, 3e | Andrews' Diseases of the Skin | Cummings Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.