Surfactant, hb oxygen dissociation curve , functional residual volume, vital capacity, transport of gases, neural regulation of respiration From guyton only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is the complete Guyton-based coverage of all six topics:
Respiratory Physiology — Guyton & Hall
1. SURFACTANT, SURFACE TENSION, AND COLLAPSE OF THE ALVEOLI
Principle of Surface Tension
Water molecules at the alveolar air-fluid interface have a strong mutual attraction, causing the surface to contract. This tends to force air out of the alveoli and collapse them — producing what is called the surface tension elastic force of the lung.
What Is Surfactant?
Surfactant is a surface-active agent that greatly reduces the surface tension of water lining the alveoli. It is secreted by type II alveolar epithelial cells, which constitute ~10% of the alveolar surface area. These cells contain lipid inclusions that are secreted as surfactant.
Surfactant is a complex mixture of:
- Dipalmitoyl phosphatidylcholine (DPPC) — the most important phospholipid
- Surfactant apoproteins
- Calcium ions
DPPC does not dissolve uniformly in the alveolar fluid; part of its molecule remains on the surface, reducing surface tension to 5–30 dynes/cm (vs. 72 dynes/cm for pure water; 50 dynes/cm for alveolar fluid without surfactant).
Pressure Due to Surface Tension (LaPlace's Law)
Pressure = 2 × Surface tension / Radius of alveolus
For an average alveolus (radius ~100 µm) with normal surfactant → ~4 cm H₂O
Without surfactant → ~18 cm H₂O (4.5× greater)
Key point: The smaller the alveolus, the greater the pressure from surface tension. Surfactant prevents small alveoli from collapsing into large ones — it stabilises all alveoli equally by reducing surface tension proportionally more in small alveoli (where surfactant molecules are more compressed and more effective).
2. FUNCTIONAL RESIDUAL CAPACITY (FRC)
Definition
FRC = Expiratory Reserve Volume (ERV) + Residual Volume (RV)
It is the volume of air remaining in the lungs at the end of normal quiet expiration — normally ~2300 mL.
Lung Volumes & Capacities (Summary)
| Capacity | Components | Normal Value |
|---|---|---|
| Inspiratory Capacity (IC) | TV + IRV | ~3500 mL |
| Functional Residual Capacity (FRC) | ERV + RV | ~2300 mL |
| Vital Capacity (VC) | IRV + TV + ERV | ~4600 mL |
| Total Lung Capacity (TLC) | VC + RV | ~5800 mL |
Key equations:
- FRC = ERV + RV
- TLC = IC + FRC
All values are ~20–30% less in women than men, and greater in athletic individuals.
Measurement of FRC — Helium Dilution Method
FRC cannot be measured directly by spirometry (residual volume cannot be expired). The helium dilution method is used:
- A spirometer of known volume is filled with air + helium at known concentration
- The subject expires normally, then begins breathing from the spirometer
- Helium becomes diluted by the FRC gases
FRC = (C_He / C_fHe − 1) × V_spir
Where C_He = initial [He], C_fHe = final [He], V_spir = initial spirometer volume.
3. VITAL CAPACITY
Definition
VC = IRV + Tidal Volume + ERV
The maximum amount of air a person can expel after maximum inspiration — normally ~4600 mL.
Forced Expiratory Vital Capacity (FVC / FEV)
In clinical practice, the forced expiratory vital capacity (FVC) is measured — the person inspires maximally, then expires as forcefully and rapidly as possible into a spirometer.
- FEV₁ (forced expiratory volume in 1 second): normally ~80% of the FVC
- In obstructive disease (e.g., asthma, emphysema): FEV₁/FVC ratio is reduced
- In restrictive disease: both FVC and FEV₁ fall, but ratio may be normal
4. TRANSPORT OF GASES
Transport of Oxygen (O₂)
97% of O₂ is transported bound to hemoglobin in RBCs. Only 3% is dissolved in plasma.
O₂-Hemoglobin Dissociation Curve
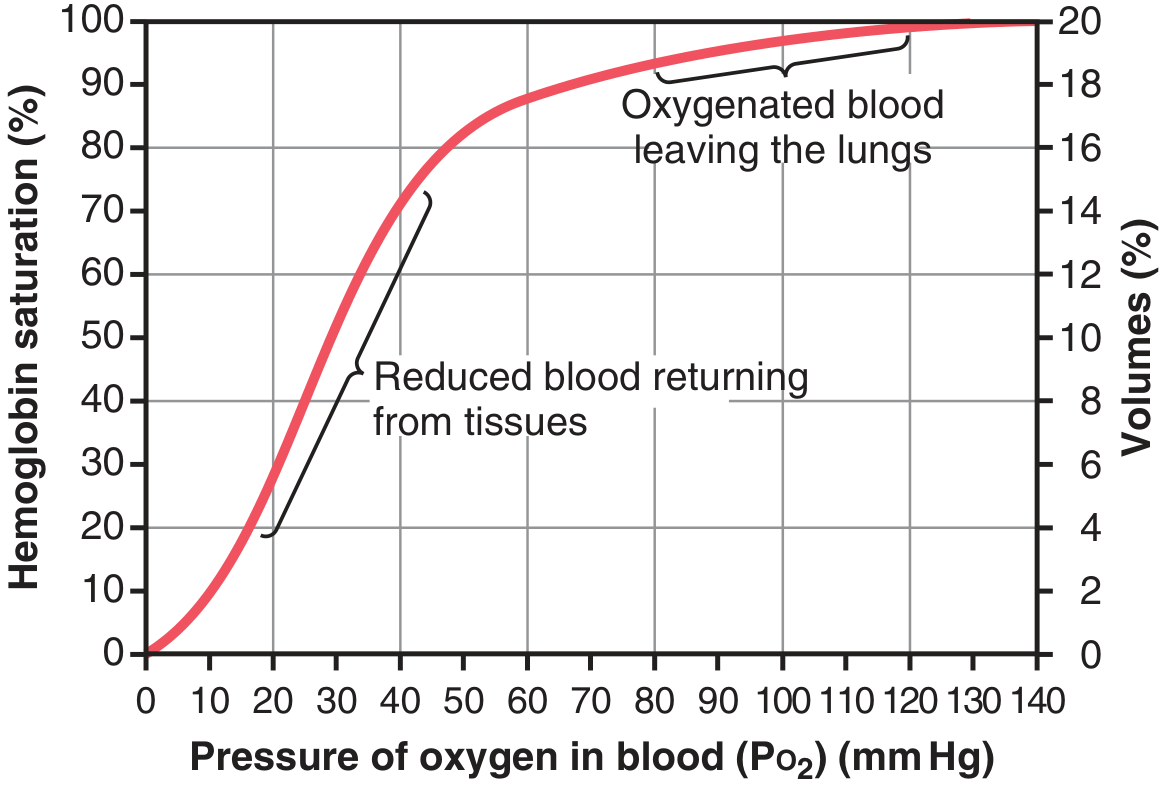
(Figure 41.8 — Guyton & Hall)
Key values:
- Systemic arterial blood: PO₂ ~95 mmHg → saturation 97% → O₂ content ~19.4 mL/100 mL
- Venous blood returning from tissues: PO₂ ~40 mmHg → saturation 75% → O₂ content ~14.4 mL/100 mL
- O₂ delivered to tissues per 100 mL = 19.4 – 14.4 = ~5 mL/100 mL blood
- Hemoglobin capacity: 15 g/dL × 1.34 mL/g = ~20 mL O₂/100 mL blood (oxygen-carrying capacity)
Shifts in the Dissociation Curve
Rightward shift (↓ affinity, ↑ O₂ release to tissues):
- ↑ CO₂
- ↓ pH (acidosis) — Bohr effect
- ↑ Temperature
- ↑ 2,3-BPG (biphosphoglycerate)
Leftward shift (↑ affinity, ↑ O₂ loading in lungs):
- ↓ CO₂, ↑ pH, ↓ temperature, ↓ BPG
Bohr Effect: In tissues, CO₂ and H⁺ shift the curve rightward → O₂ is released. In lungs, CO₂ leaves blood → curve shifts leftward → O₂ is loaded. This doubles O₂ delivery efficiency.
BPG Effect: In chronic hypoxia, ↑ BPG shifts curve rightward → O₂ released at up to 10 mmHg higher tissue PO₂ → important adaptation to hypoxia.
During exercise: CO₂, H⁺, and temperature all rise in muscle capillaries → massive rightward shift → O₂ released even when 70% has already been removed.
Transport of CO₂
CO₂ is transported by 3 mechanisms:
| Mechanism | % of Total |
|---|---|
| As bicarbonate ion (HCO₃⁻) in plasma | ~70% |
| As carbaminohemoglobin (CO₂Hb) | ~23% |
| Dissolved in plasma | ~7% |
Bicarbonate Transport (Chloride Shift)
In tissue capillaries:
- CO₂ enters RBCs → carbonic anhydrase (5000× faster) catalyses: CO₂ + H₂O → H₂CO₃
- H₂CO₃ → H⁺ + HCO₃⁻
- H⁺ is buffered by hemoglobin
- HCO₃⁻ diffuses out into plasma
- Cl⁻ enters RBC to maintain electrical neutrality → Chloride Shift (Hamburger shift)
This is reversed in the lungs.
Haldane Effect
When O₂ binds hemoglobin in the lungs (oxygenation), CO₂ is displaced from hemoglobin and released into alveoli. This doubles the amount of CO₂ released in the lungs — complementing the Bohr effect.
Respiratory Exchange Ratio (R)
- Normal: R = 0.825 (mixed diet)
- Carbohydrates only: R = 1.00
- Fats only: R = 0.70
5. NEURAL REGULATION OF RESPIRATION
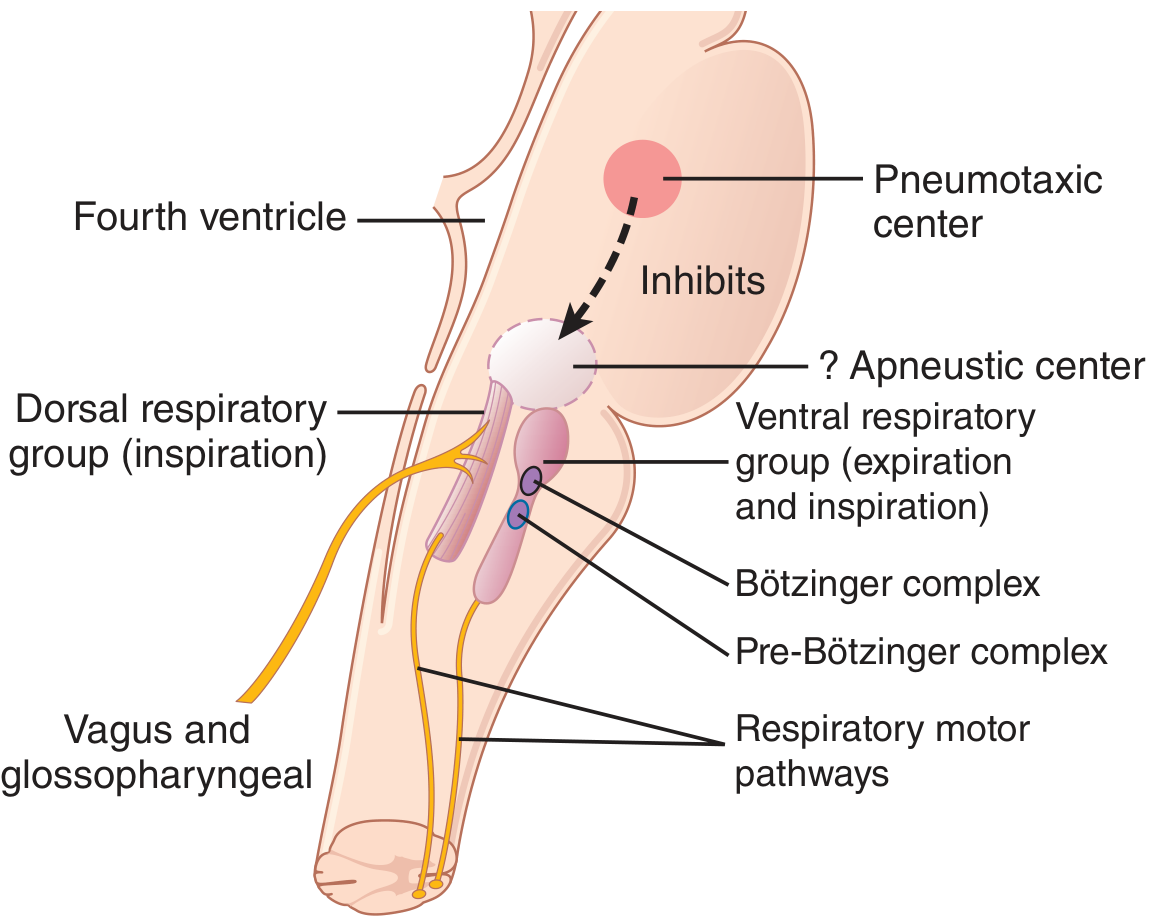
(Figure 42.1 — Guyton & Hall)
The Respiratory Center
Located bilaterally in the medulla oblongata and pons, divided into three groups:
1. Dorsal Respiratory Group (DRG) — Medulla
- Located in the nucleus tractus solitarius (NTS)
- Primarily responsible for inspiration and the basic rhythm of respiration
- Receives sensory input from peripheral chemoreceptors, baroreceptors, and lung receptors via vagus and glossopharyngeal nerves
- Generates the inspiratory ramp signal: starts weakly, builds steadily over ~2 seconds, then cuts off abruptly → elastic recoil produces expiration
Pre-Bötzinger Complex: A small region in the rostral ventral respiratory group with spontaneously firing pacemaker neurons. Critical for generating the basic rhythm — its removal eliminates respiratory rhythm generation.
2. Ventral Respiratory Group (VRG) — Medulla
- Contains both inspiratory and expiratory neurons
- Quiescent during normal quiet breathing
- Activated during forced breathing (exercise) when extra respiratory effort is needed
- Expiratory neurons actively contract abdominal and internal intercostal muscles during forced expiration
3. Pneumotaxic Center — Upper Pons
- Located in the nucleus parabrachialis
- Inhibits inspiration — limits the duration of the inspiratory ramp signal
- When strong: shortens inspiration → ↑ respiratory rate
- When weak: allows prolonged inspiration → slower rate but deeper breaths
- Works together with the apneustic center (lower pons): apneustic center tries to sustain inspiration; pneumotaxic center cuts it off
Chemical Control of Respiration
CO₂ and H⁺ — Direct Central Control
The chemosensitive area (retrotrapezoid nucleus), lying 0.2 mm beneath the ventral medullary surface, is highly sensitive to:
- H⁺ ions — direct stimulation (but H⁺ crosses blood-brain barrier poorly)
- CO₂ — crosses BBB freely → reacts with water → forms H⁺ → stimulates chemosensitive neurons
CO₂ is the primary driver of respiration. A small rise in PCO₂ (35–75 mmHg range) causes a massive increase in ventilation. pH changes in the normal range (7.3–7.5) have <10% the effect of CO₂.
Important: The stimulatory effect of chronic CO₂ elevation attenuates over 1–2 days as kidneys raise plasma HCO₃⁻, which diffuses into CSF and buffers H⁺ → reduced drive (basis of CO₂ retention in COPD).
O₂ — Peripheral Chemoreceptors
O₂ has virtually no direct effect on the central respiratory center. It acts via peripheral chemoreceptors:
- Carotid bodies (at bifurcation of common carotid arteries) — afferents via Hering nerve → glossopharyngeal nerve → DRG
- Aortic bodies (along aortic arch) — afferents via vagus → DRG
- Chemoreceptor cells = glomus cells (O₂-sensitive; respond through K⁺ channel inhibition)
- Strongly stimulated when PO₂ falls below 60 mm Hg (on the steep part of the Hb dissociation curve)
Regulation During Exercise
At the onset of exercise:
- Ventilation increases almost immediately — before any blood gas changes
- This is due to collateral nerve impulses from the motor cortex to the respiratory center (neurogenic drive)
- CO₂ and H⁺ serve as fine-tuning mechanisms to match ventilation precisely to metabolic demands
- The neurogenic signal shifts the entire ventilatory response curve upward, maintaining arterial PCO₂ at ~40 mmHg even during heavy exercise
All content sourced from: Guyton and Hall Textbook of Medical Physiology (Guyton & Hall, 9780443111013), Chapters 38, 41, 42
Haemoglobin oxygen dissociation curve from guyton
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.