What is headache?
Reading File
Finding Sources
Searching the Web
headache definition classification types overview
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of headache drawn from leading medical textbooks:
Headache
Definition
A headache is pain or discomfort felt anywhere in the region of the head or upper neck. It is one of the most common neurological complaints encountered in clinical practice. The clinician's first goal is to determine whether the headache is primary (head pain is the only identifiable disease) or secondary (a symptom caused by another underlying condition).
- Adams and Victor's Principles of Neurology, 12th Ed.
Classification (ICHD-3)
The International Headache Society (IHS) released the third edition of the International Classification of Headache Disorders (ICHD-3), organizing headaches into three broad groups:
1. Primary Headache Disorders
Head pain is itself the condition - no underlying structural or metabolic cause.
| Type | Key Features |
|---|---|
| Migraine (with or without aura) | Recurrent, often unilateral, pulsating, 4-72 hours; nausea, photophobia, phonophobia |
| Tension-type headache | Bilateral, pressing/tightening (non-pulsating), mild-moderate; no nausea |
| Cluster headache | Strictly unilateral periorbital pain, excruciating; autonomic features (lacrimation, nasal congestion); mainly young adult males |
| Other primary headaches | Cough headache, exercise headache, hypnic headache, etc. |
Over 90% of patients presenting to primary care with headache have one of these four primary disorders.
2. Secondary Headache Disorders
Headache attributed to another condition. Major categories include:
-
Head trauma (within 7 days)
-
Intracranial disorders (hemorrhage - subarachnoid, subdural)
-
Infections (meningitis, fever, sinusitis, viral illness)
-
Metabolic disorders (hypertension, hypothyroidism, hypoxia/hypercapnia, fasting, dialysis)
-
Substance use or withdrawal (caffeine, alcohol, medications)
-
Disorders of the cranium or face (cranial neuralgias, neck/eye/ear/sinus/dental problems)
-
Kaplan & Sadock's Comprehensive Textbook of Psychiatry
3. Cranial Neuralgias and Facial Pain
Includes trigeminal neuralgia and other nerve-related pain syndromes.
Pathophysiology
- Migraine: Involves the trigeminovascular system - activation of trigeminal nerve fibers around cranial blood vessels releases neuropeptides (notably calcitonin gene-related peptide, CGRP), causing neurogenic inflammation and sensitization. Cortical spreading depression underlies the aura.
- Tension-type: Less well understood. Increased myofascial tenderness, particularly in the chronic form. Central sensitization may play a role.
- Cluster headache: Inferior posterior hypothalamic activation is demonstrated on PET and fMRI at onset. The trigeminovascular complex and cranial autonomic system are co-activated. - Goldman-Cecil Medicine
Red Flags (Danger Signs Requiring Imaging)
The following features require urgent investigation (MRI preferred):
-
Thunderclap headache - sudden onset, peak pain within 1 minute (suspect subarachnoid hemorrhage)
-
New-onset severe headache with no prior headache history
-
Progressive worsening in frequency or severity
-
"Worst headache of my life"
-
Headache always localized to one side
-
Fever, altered mental status, or focal neurological deficit
-
Headache in a cancer patient
-
New onset after age 50 (consider giant cell arteritis)
-
Provoked by sexual activity
-
Bradley and Daroff's Neurology in Clinical Practice
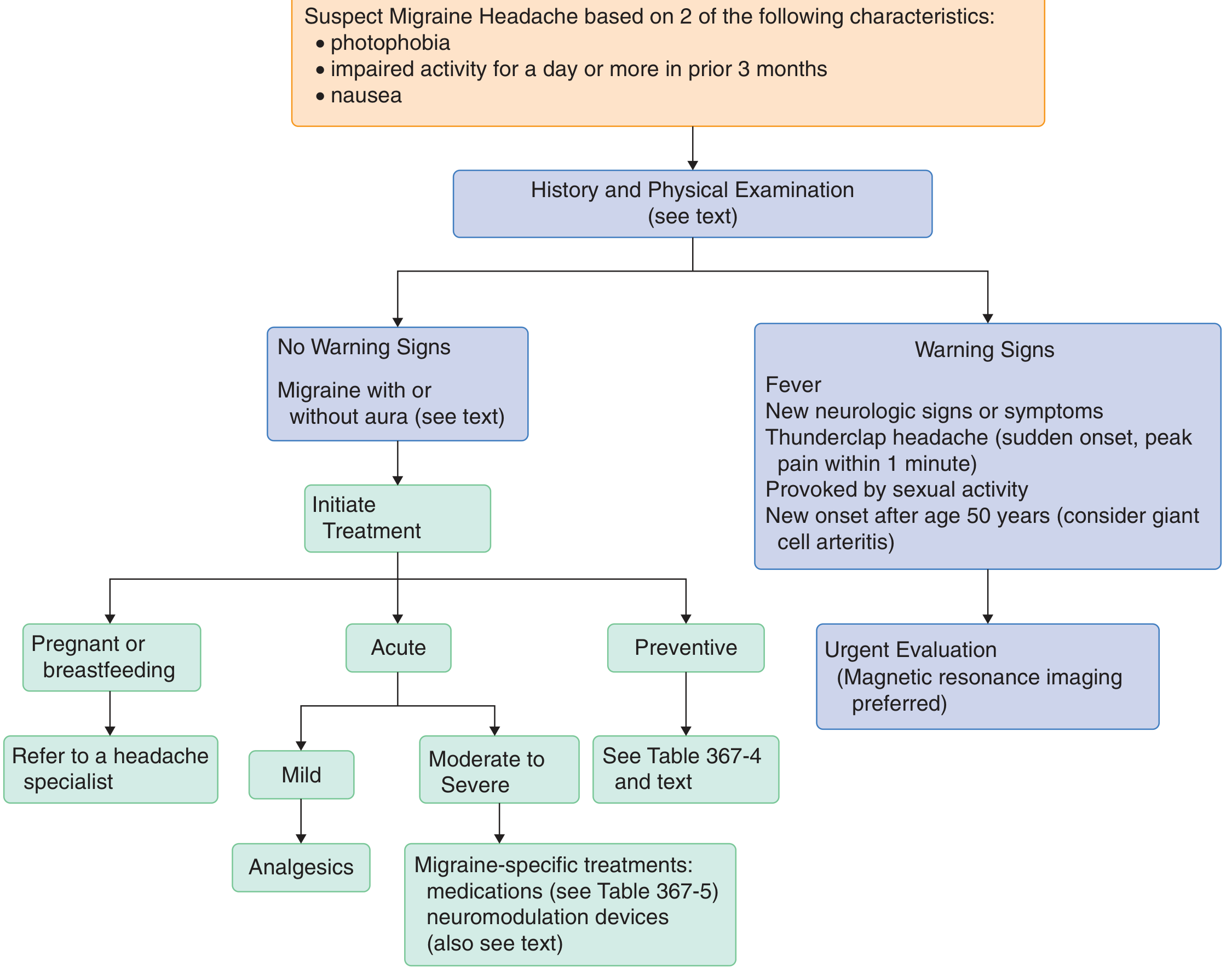
Diagnostic Approach - Migraine Flowchart
The following flowchart (from Goldman-Cecil Medicine) guides evaluation when migraine is suspected:
Treatment Summary
Migraine - Acute
- Mild attacks: Acetaminophen (650-1000 mg) or NSAIDs (ibuprofen 400-600 mg, naproxen 500-825 mg, aspirin 250-1000 mg)
- Moderate-severe: Triptans (e.g., sumatriptan), dihydroergotamine, or CGRP receptor antagonists (rimegepant 75 mg, ubrogepant 50-100 mg)
- Very severe/refractory: IV/IM dihydroergotamine, ketorolac, prochlorperazine, metoclopramide
- Opioids should be a last resort only
Migraine - Preventive
Indicated when attacks are frequent or disabling: propranolol, amitriptyline, topiramate, valproate (avoid in women of childbearing potential), CGRP monoclonal antibodies (newer agents)
Tension-type Headache
- Episodic: Acetaminophen or NSAIDs
- Chronic: Amitriptyline (10-100 mg), nortriptyline, physical therapy, acupuncture, behavioral therapy
- Caution: analgesic use >3 days/week can cause medication-overuse headache
Cluster Headache
-
Acute: 100% oxygen (high-flow), sumatriptan injection
-
Preventive: verapamil, corticosteroids, lithium (for prolonged episodes)
-
Goldman-Cecil Medicine; Bradley and Daroff's Neurology
Key takeaway: Most headaches are primary (benign) and manageable. The priority in any headache evaluation is to identify secondary causes - especially those requiring emergency intervention - using a careful history, examination, and selective imaging guided by red flags.
This is a shared conversation. Sign in to Orris to start your own chat.