Flow volume loop full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Flow-Volume Loop (FVL) - Complete Answer for MD Exam (15 Marks)
1. Definition
A flow-volume loop (FVL) is a graphic representation that plots the flow rate (L/sec) on the Y-axis against the volume (L) on the X-axis, generated during a complete forced respiratory maneuver - forced expiration from total lung capacity (TLC) down to residual volume (RV), followed by a forced inspiration back to TLC. The loop encompasses both the expiratory and inspiratory limbs of the forced vital capacity maneuver.
- Barash's Clinical Anesthesia, p. 1137
2. How the Loop is Performed
The subject:
- Inhales maximally to TLC
- Exhales as forcefully and completely as possible to RV
- Immediately inhales as forcefully as possible back to TLC
In spontaneously breathing individuals, forced expiration precedes inhalation to vital capacity. In mechanical ventilation, the loop is typically inverted.
3. Axes and Orientation
| Axis | What it represents |
|---|---|
| Y-axis (above zero line) | Expiratory flow (L/sec) |
| Y-axis (below zero line) | Inspiratory flow (L/sec) |
| X-axis (left) | TLC (high volume) |
| X-axis (right) | RV (low volume / end expiration) |
The tidal volume loop sits as a small loop nestled within the larger maximal FVL, centered around FRC.
4. Normal Flow-Volume Loop
Normal FVL (Barash's Clinical Anesthesia):
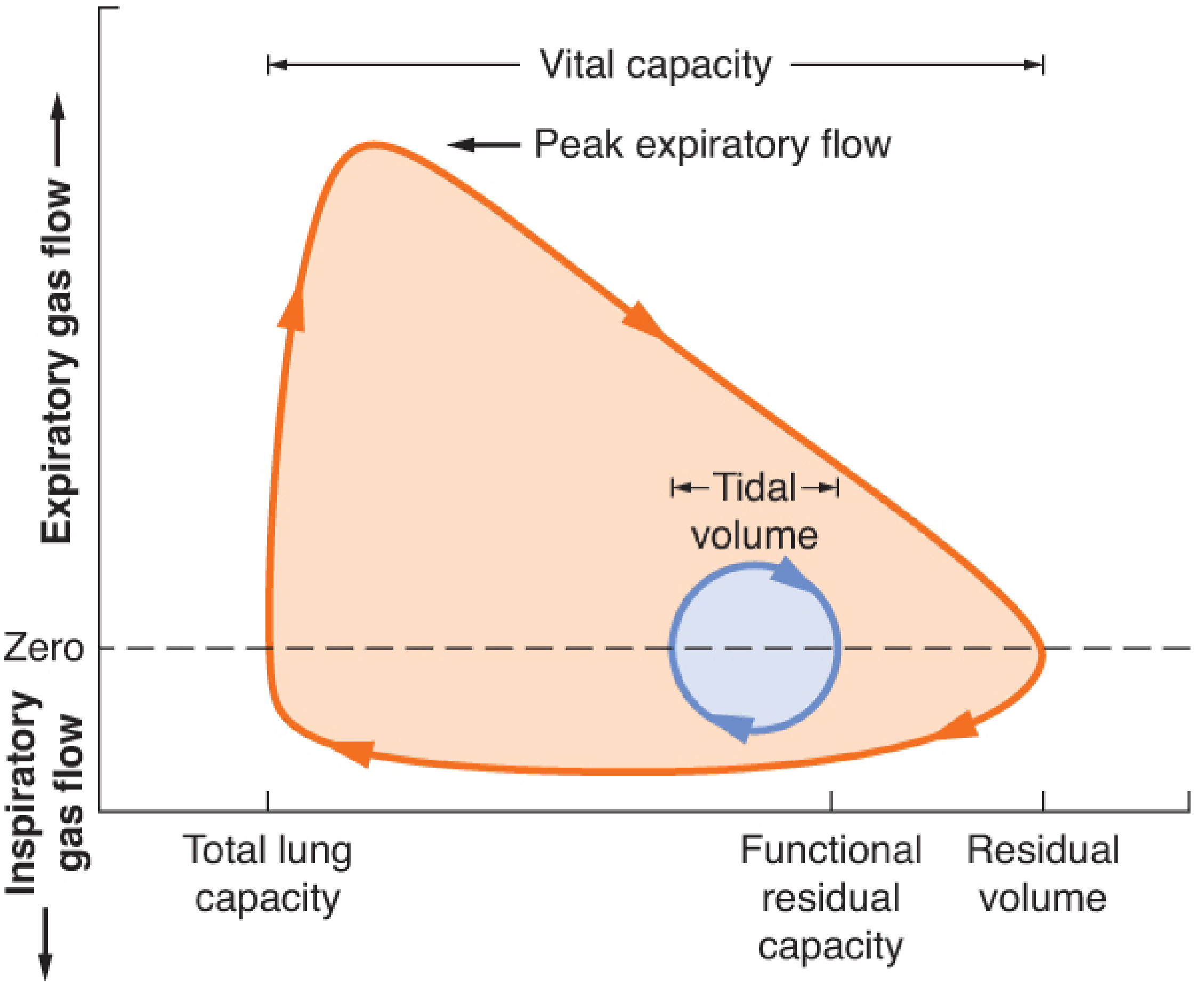
Key features of the normal loop:
- Expiratory limb: Rapid rise to Peak Expiratory Flow (PEF) early in expiration, then a gradual, nearly linear decline to RV. The descending slope after PEF is roughly linear (effort-independent portion).
- Inspiratory limb: Smooth, symmetric dome-shaped curve below the zero line - relatively effort-independent throughout and relatively symmetric.
- Expiration is effort-dependent at high lung volumes (the initial peak) and effort-independent at lower lung volumes (the descending limb, governed by elastic recoil and airway resistance).
- The slope of the expiratory loop after PEF is nearly linear in a normal adult.
5. Key Measurements Derived from the FVL
| Parameter | Definition |
|---|---|
| FVC | Forced Vital Capacity - total volume exhaled |
| FEV₁ | Forced expiratory volume in 1 second |
| FEV₁/FVC ratio | Key discriminator of obstructive vs restrictive |
| PEF (PEFR) | Peak expiratory flow rate |
| FEF 25-75% | Mean forced expiratory flow at mid-lung volumes - sensitive marker of small airway disease |
| FEF50% / FIF50% | Ratio of expiratory to inspiratory flow at 50% of FVC - used in upper airway obstruction |
| FEV₁/PEFR | If >8 mL/L/min, suggests upper airway obstruction |
6. Pathological Patterns
A. Obstructive Ventilatory Defect (e.g., COPD, Asthma, Emphysema)
- FEV₁/FVC reduced (below lower limit of normal)
- FEV₁ reduced, FVC normal or reduced
- Expiratory limb shows upward concavity ("scooped out" / curvilinear pattern) - reduced flows at lower lung volumes
- Inspiratory limb remains relatively normal in shape
- In emphysema: small airway obstruction and poor elastic recoil cause reduced flow at lower lung volumes with relatively preserved flows at higher volumes
- "Negative effort dependence" may occur: tidal breathing flows exceed maximal effort flows due to airway collapse at high expiratory pressures - seen in emphysema, cystic fibrosis, bronchiolitis obliterans
(Murray & Nadel's Textbook of Respiratory Medicine)
B. Restrictive Ventilatory Defect (e.g., Pulmonary Fibrosis, Obesity, Chest Wall Disease)
- FEV₁/FVC ratio normal or elevated
- Both FVC and FEV₁ reduced proportionally
- Loop is narrow and tall - a "steep and vertically oriented" curve
- Reduced TLC confirmed on lung volumes
- FVL shape may look qualitatively normal but simply compressed along the volume axis
(Murray & Nadel's Textbook of Respiratory Medicine)
C. Asthma (Reversible Obstruction)
Flow-volume loops in asthma (Murray & Nadel's):
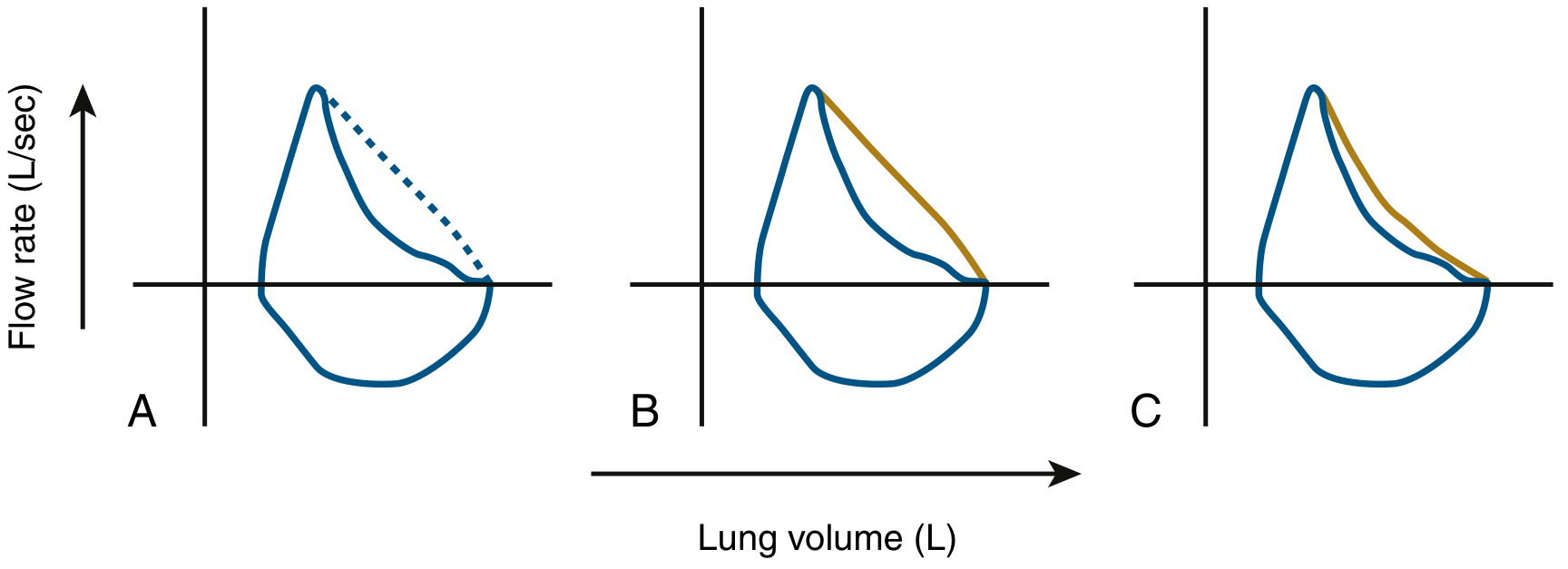
- (A) Scooped expiratory limb compared to predicted normal (dashed line)
- (B) Complete reversal of scooping after bronchodilator
- (C) Incomplete reversal post-bronchodilator
In acute severe asthma: TLC and RV both increase (air trapping); the loop shrinks markedly and shifts leftward. As the exacerbation resolves, FEV₁ and PEFR improve together while FEF 25-75% (MMEFR) lags behind.
7. Upper Airway Obstruction Patterns
This is the most high-yield and distinctive use of the FVL. Three patterns are recognized:
Schematic FVLs in four pathologic conditions (Fishman's Pulmonary Diseases):
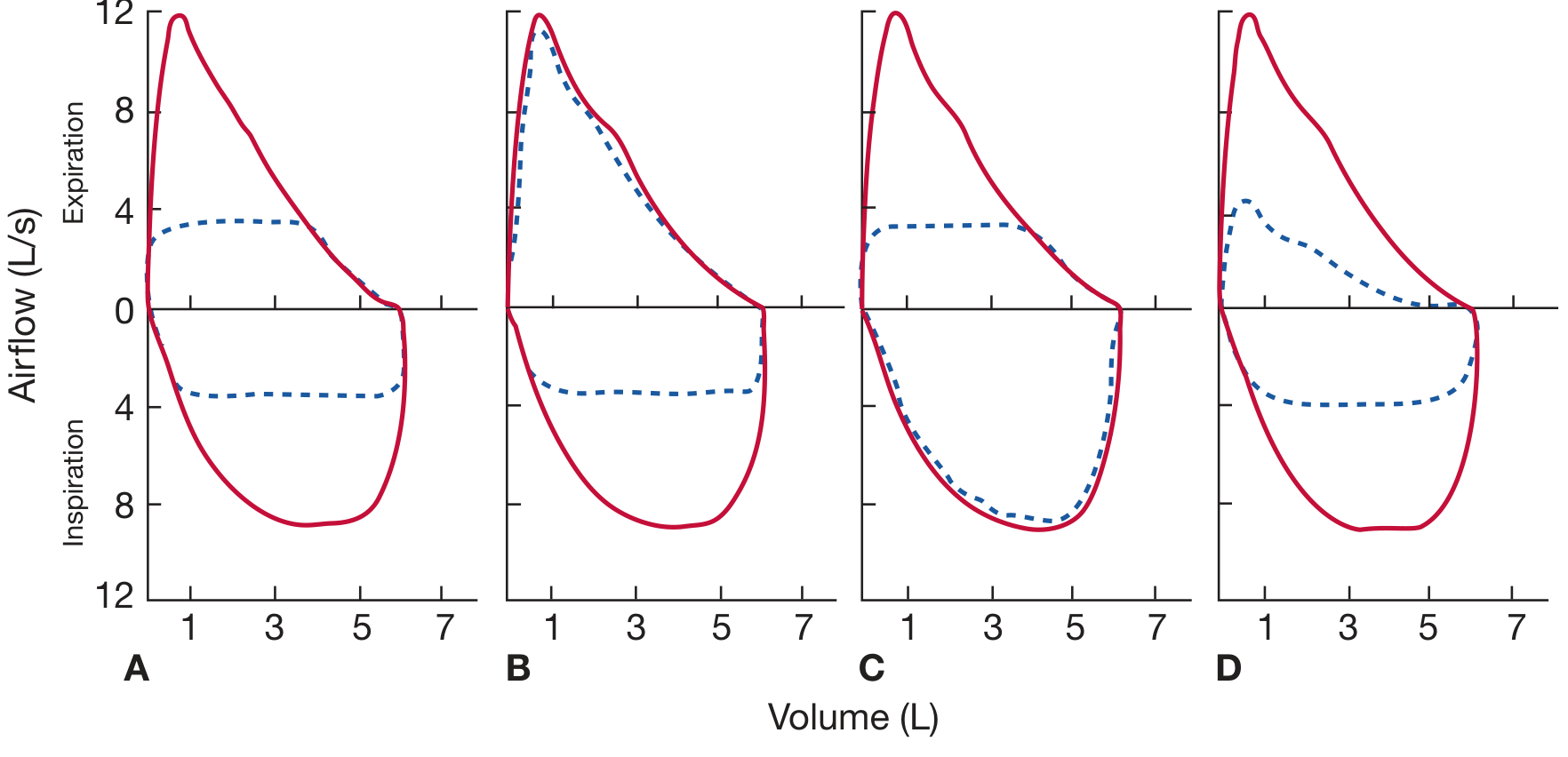
| Type | Location | Mechanism | FVL Pattern |
|---|---|---|---|
| Fixed obstruction | Extra- or intrathoracic (e.g., tracheal scar post-tracheotomy) | Rigid fixed lesion - geometry unchanged by respiration | Both inspiratory AND expiratory limbs truncated/flattened equally |
| Variable extrathoracic obstruction | Above the thoracic inlet (e.g., vocal cord paralysis, laryngeal tumour) | During forced inspiration, intratracheal pressure < atmospheric, causing collapse at lesion site | Inspiratory limb flattened; expiratory limb normal |
| Variable intrathoracic obstruction | Below the thoracic inlet within chest (e.g., tracheal tumour, tracheomalacia) | During forced expiration, pleural pressure exceeds intratracheal pressure at lesion, causing obstruction | Expiratory limb flattened; inspiratory limb normal |
(Fishman's Pulmonary Diseases and Disorders)
Key distinguishing point: In COPD/obstructive disease, the expiratory limb shows a gradual taper retaining its normal configuration (early peak then gradual decline), whereas in variable intrathoracic obstruction the expiratory limb is flat throughout.
Clues from routine PFTs suggesting upper airway obstruction:
- FEV₁/PEFR > 8 mL/L/min
- FEF₅₀%/FIF₅₀% ≥ 1 (normally FIF₅₀% > FEF₅₀%)
- FIF₅₀% < 100 L/min
- FEV₁/FEV₀.₅ ≥ 1.5
8. FVL in Exercise Testing (CPET)
Plotting exercise tidal flow-volume loops (extFVLs) within the maximal flow-volume loop (MFVL) provides information about ventilatory constraints during exercise:
- Encroachment of VT on the expiratory limb of the MFVL = expiratory flow limitation
- Increased end-expiratory lung volume relative to rest = dynamic hyperinflation
- Encroachment of tidal inspiratory flow on the inspiratory limb of MFVL = inspiratory muscle capacity is approaching maximum
This is particularly studied in COPD, heart failure, and elite athletes.
(Fishman's Pulmonary Diseases and Disorders)
9. FVL in Neuromuscular Diseases
In motor neuron disease (ALS, Parkinson's): Flow-volume loops may show:
- Oscillations ("sawtooth pattern") on the inspiratory limb - due to vocal cord or upper airway tremor
- Inspiratory flow limitation
- Rounded peak of the mid-expiratory curve
- Reduced PEF and delayed appearance of PEF
- In Parkinson's disease: rhythmic oscillations superimposed on both expiratory and inspiratory limbs reflecting upper airway rigidity
(Fishman's Pulmonary Diseases and Disorders)
10. Clinical Utility and Limitations
Indications:
- Diagnosis of obstructive vs. restrictive vs. mixed lung disease
- Pre-operative pulmonary evaluation
- Upper airway obstruction (though largely replaced by CT/MRI for anatomic lesions)
- Monitoring response to bronchodilator therapy
- Assessing ventilatory limitation in exercise testing
- Diagnosis and follow-up of asthma, COPD, IPF
Configuration is the most informative part of the test - more so than individual numbers alone.
Limitations:
- Requires patient effort and cooperation
- At least 3 acceptable maneuvers required (ATS/ERS criteria)
- Two largest FVC and FEV₁ values must be within 150 mL
- FVL alone has low sensitivity for restrictive disease (TLC measurement needed for confirmation - spirometry falsely identifies restriction in ~58% of loops suggesting restrictive defect)
- CT/MRI have largely replaced FVL for anatomic upper airway assessment
Summary Table: FVL Patterns at a Glance
| Condition | PEF | FEV₁/FVC | Expiratory Limb | Inspiratory Limb |
|---|---|---|---|---|
| Normal | Normal | >0.70 | Gradual linear decline | Smooth dome |
| Obstructive (COPD/Asthma) | Reduced | Reduced | Concave upward (scooped) | Normal |
| Restrictive | Normal/reduced | Normal/elevated | Narrow, tall - normal shape | Normal |
| Fixed upper airway obstruction | Reduced | Variable | Flat / truncated | Flat / truncated |
| Variable extrathoracic obstruction | Normal | Variable | Normal | Flattened |
| Variable intrathoracic obstruction | Normal | Variable | Flattened | Normal |
Sources: Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Barash's Clinical Anesthesia, 9e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.