Effect of pregnancy on respiratory system full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have everything needed for a complete, exam-ready answer. Here it is:
Effect of Pregnancy on the Respiratory System
Introduction
Pregnancy induces significant anatomical, mechanical, and biochemical changes in the respiratory system. These adaptations serve two main purposes: meeting the increased metabolic demands of both mother and fetus, and accommodating the growing uterus. Understanding these changes is essential for managing respiratory disease in pregnancy and for obstetric anaesthesia.
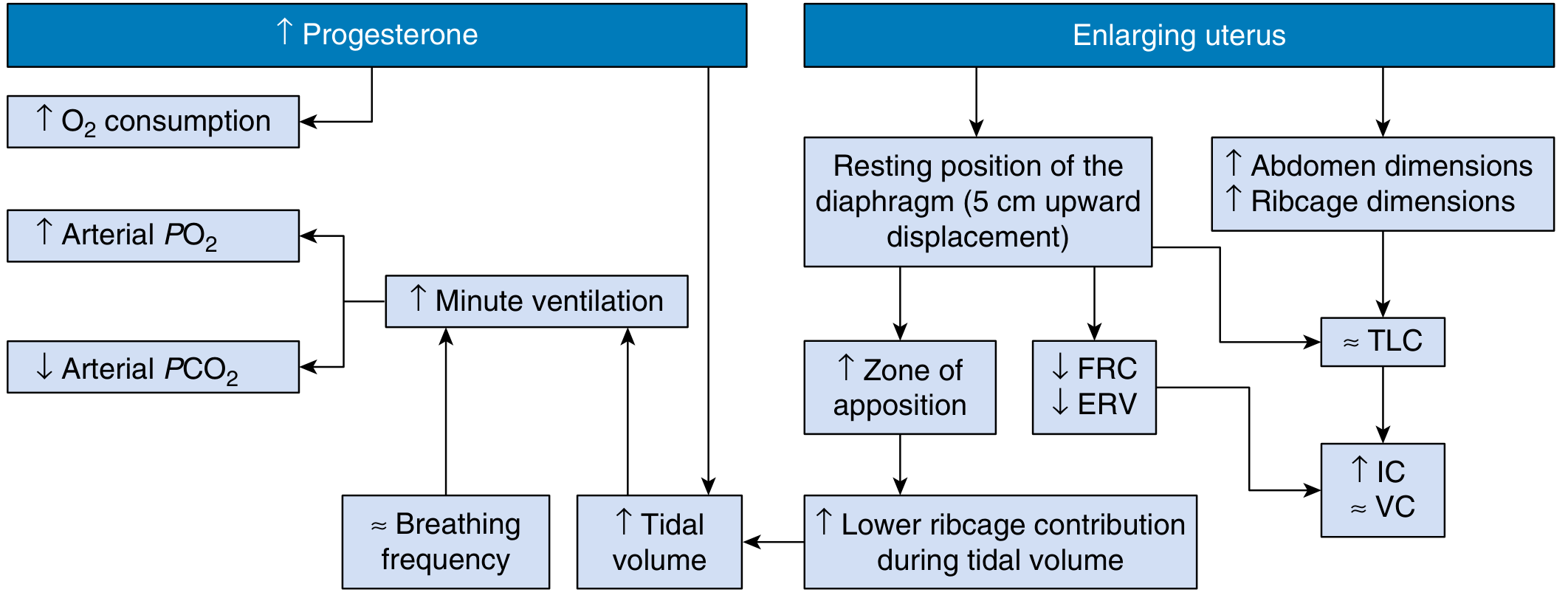
Figure: Biochemical (progesterone) and mechanical (enlarging uterus) pathways summarising pregnancy's effects on pulmonary function, ventilatory pattern, and gas exchange. (From Creasy & Resnik's Maternal-Fetal Medicine)
1. Anatomical Changes
Chest wall and diaphragm:
- The enlarging uterus displaces the diaphragm upward by approximately 4-5 cm
- The subcostal angle widens from 68 degrees to 103 degrees - this occurs early in pregnancy even before significant uterine enlargement, suggesting hormonal (relaxin) mediation
- The transverse diameter of the chest increases by approximately 2 cm
- Chest circumference increases by up to 5-7 cm
- Despite the upward displacement of the diaphragm at rest, diaphragmatic excursion during breathing is actually increased by ~1.5 cm
Upper airway:
- Mucosal hyperaemia and oedema of the nasal passages, oropharynx, and larynx occur due to oestrogen-mediated increased vascularity
- This produces nasal stuffiness ("rhinitis of pregnancy") and can cause difficult intubation
- Airway resistance actually decreases by ~35% due to progesterone-mediated smooth muscle relaxation
2. Lung Volumes and Capacities
| Parameter | Nonpregnant | Pregnant | Change |
|---|---|---|---|
| Total Lung Capacity (TLC) | 4200 mL | 4000 mL | -4% |
| Vital Capacity (VC) | 3200 mL | 3200 mL | No change |
| Inspiratory Capacity (IC) | 2500 mL | 2650 mL | +6% |
| Tidal Volume (TV) | 450 mL | 600 mL | +33 to 40% |
| Inspiratory Reserve Volume (IRV) | 2050 mL | 2050 mL | No change |
| Expiratory Reserve Volume (ERV) | 700 mL | 550 mL | -20% |
| Residual Volume (RV) | 1000 mL | 800 mL | -20% |
| Functional Residual Capacity (FRC) | 1700 mL | 1350 mL | -18 to 20% |
Key points:
- FRC decreases because both ERV and RV decrease - this is primarily due to upward displacement of the diaphragm
- Vital capacity is preserved despite the mechanical changes, because the increase in IC compensates for the decrease in ERV
- TLC decreases only slightly (-4%)
- The decrease in FRC is clinically important - it reduces the oxygen reserve and predisposes to rapid desaturation during apnoea (e.g., during intubation)
3. Ventilation Changes
Tidal Volume and Respiratory Rate:
- Tidal volume increases by 40-50% (from ~500 mL to ~700 mL)
- Respiratory rate remains unchanged early in pregnancy; rises by only ~10% late in pregnancy
- The result is a 50% increase in minute ventilation (from ~7.5 L/min to ~10.5 L/min)
Physiological dead space:
- Increases by approximately 60 mL in pregnancy, likely due to dilation of small airways
Mechanism:
- The primary driver is progesterone, which acts as a direct respiratory stimulant on the central respiratory centre
- Progesterone lowers the CO2 threshold of the respiratory centre and increases sensitivity to CO2: a rise of 1 mmHg in PaCO2 increases ventilation by 6 L/min in pregnancy vs. 1.5 L/min in the non-pregnant state
- An increase in basal metabolic rate also contributes
- Progesterone may also increase red blood cell carbonic anhydrase B levels, facilitating CO2 transfer independently of ventilation changes
- This hyperventilation begins as early as the first trimester
4. Gas Exchange Changes
Arterial Blood Gas (ABG) Changes in Pregnancy:
| Parameter | Non-pregnant | Pregnant | Change |
|---|---|---|---|
| pH | 7.40 | 7.44 (7.40-7.47) | Slightly alkaline |
| PaCO2 | 39 mmHg | 28-32 mmHg | -15% |
| PaO2 | ~95 mmHg | 101-104 mmHg | +10% |
| HCO3- | 24 mEq/L | 18-22 mEq/L | -15% |
Respiratory Alkalosis of Pregnancy:
- Increased minute ventilation causes a compensated respiratory alkalosis
- PaCO2 falls to 28-32 mmHg
- The kidneys compensate by excreting bicarbonate, reducing serum HCO3- to 18-22 mEq/L
- Arterial pH is mildly alkalotic at 7.44 (vs. 7.40 non-pregnant)
- This is a normal finding in pregnancy and should not be labelled pathological
Clinical implication: When interpreting ABGs in a pregnant woman, a PCO2 of 32 mmHg is NORMAL. A PCO2 of 40 mmHg in a pregnant woman suggests respiratory failure (she is unable to maintain the expected hyperventilation).
Oxygen Dissociation Curve:
- Respiratory alkalosis shifts the curve to the left - increases maternal Hb affinity for O2 (Bohr effect) - potentially reducing O2 release to the fetus
- This is compensated by an alkalosis-induced increase in 2,3-DPG in maternal erythrocytes, which shifts the curve back to the right, facilitating O2 transfer to the fetus
- Net result: efficient oxygen delivery to the fetus is maintained
5. Oxygen Consumption
- O2 consumption increases by 20-50% by term
- Due to: increased maternal metabolic demands + fetal requirements + increased cardiac work
- Oxygen delivery = Cardiac Output x Arterial Oxygen Content
- Despite the increased O2 demand, the hyperventilation of pregnancy increases PaO2 to 101-104 mmHg, maintaining adequate oxygen delivery
- At higher altitudes, even greater compensatory hyperventilation occurs
6. Airway Changes (Clinically Important)
- Mucosal oedema and capillary engorgement of the upper airway (due to oestrogen)
- Increased risk of nosebleeds (epistaxis)
- Nasal stuffiness throughout pregnancy
- In the third trimester, laryngeal oedema may make intubation more difficult - always use a smaller endotracheal tube (6.0-6.5 mm ID instead of standard 7.5-8.0 mm)
- These changes are exacerbated by pre-eclampsia
7. Dyspnoea of Pregnancy
- Up to 75% of pregnant women experience dyspnoea, usually beginning in the first or second trimester
- Paradoxically, dyspnoea appears before the mechanical effects of the uterus are significant, suggesting a neurochemical mechanism
- It may be due to heightened awareness of the increased ventilatory drive from progesterone
- FEV1 and FVC are unchanged - so spirometry is normal
- Dyspnoea that is severe, progressive, or associated with other symptoms warrants further evaluation
8. Summary Table of Respiratory Changes
| Parameter | Direction | Approximate Change |
|---|---|---|
| Tidal Volume | Increase | +40-50% |
| Respiratory Rate | No change / slight increase | 0 to +10% |
| Minute Ventilation | Increase | +50% |
| FRC | Decrease | -18-20% |
| ERV | Decrease | -20% |
| RV | Decrease | -20% |
| Vital Capacity | No change | 0 |
| TLC | Slight decrease | -4% |
| IC | Increase | +6% |
| IRV | No change | 0 |
| PaO2 | Increase | +10% |
| PaCO2 | Decrease | -15% (to 28-32 mmHg) |
| HCO3- | Decrease | -15% (to 18-22 mEq/L) |
| pH | Slight increase | 7.44 |
| O2 Consumption | Increase | +20-50% |
| Airway Resistance | Decrease | -35% |
9. Clinical Relevance (for MD Exams)
- Rapid desaturation during apnoea - reduced FRC = decreased O2 reserve. Always pre-oxygenate pregnant patients before intubation.
- Normal ABG in pregnancy = respiratory alkalosis. A "normal" PaCO2 of 40 mmHg = CO2 retention in pregnant patients.
- Difficult airway - mucosal oedema, increased Mallampati score, must plan for difficult intubation.
- Asthma management - pregnancy-induced hyperventilation means the expected PCO2 is lower; a rising PCO2 toward 40 mmHg in an asthmatic pregnant woman signals fatigue and impending respiratory failure.
- Spirometry is unaffected - FEV1 and FVC remain normal; useful for evaluating true airway disease in pregnancy.
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.