Pelvic oragn prolapse
Reading File
Finding Sources
Searching PubMed
"pelvic organ prolapse"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple textbooks. Let me compile the full answer.
Pelvic Organ Prolapse (POP)
Definition
Pelvic organ prolapse is the descent of one or more of the anterior vaginal wall, posterior vaginal wall, uterus (cervix), or apex of the vagina (vault or cuff scar after hysterectomy), correlated with symptoms. It represents progressive herniation of the pelvic organs through the urogenital diaphragm, most commonly producing vaginal bulge symptoms.
- Berek & Novak's Gynecology, p. 1594
Epidemiology
- Prevalence of at least one pelvic floor disorder in U.S. women is approximately 23.7%, more than doubling in women 80 years and older.
- The lifetime probability of surgical correction for POP is approximately 12.6% by age 80 (roughly 1 in 5 women will have surgery for POP or stress urinary incontinence).
- Annual POP procedure rates are projected to increase by 46% from 2010-2050, with up to one-third of the female population expected to have at least one pelvic floor disorder by 2050.
- Berek & Novak's Gynecology, pp. 1594-1595
Anatomy and Support Levels (DeLancey's Three Levels)
Pelvic organ support depends on the interaction between the levator ani muscles and the endopelvic fascia. Three levels of pelvic support are recognized:
| Level | Support Structures | Loss Results In |
|---|---|---|
| I | Uterosacral-cardinal ligament complex - suspends uterus/upper vagina to sacrum and lateral pelvic sidewall | Uterine/vaginal apical prolapse |
| II | Paravaginal attachments - lateral vaginal attachment to arcus tendineus fascia pelvis | Cystocele (anterior), rectocele (posterior) |
| III | Distal vaginal support - fusion to perineal body and urogenital diaphragm | Urethral hypermobility, distal rectocele, perineal descent |
The urogenital hiatus - kept closed by tonic levator ani activity - is the opening through which prolapse occurs. When levator tone is lost, the entire support burden shifts to the ligaments of the endopelvic fascia, which eventually fail.
- Campbell-Walsh-Wein Urology, pp. 3416-3417
Types of Prolapse
| Type | Compartment | Defect |
|---|---|---|
| Cystocele | Anterior | Bladder herniation through anterior vaginal wall |
| Urethrocele | Anterior | Urethral descent |
| Uterine prolapse | Apical | Descent of the uterus/cervix |
| Vaginal vault prolapse | Apical | Apex descends after hysterectomy |
| Enterocele | Posterior/apical | Peritoneal sac with bowel herniates between vaginal cuff and rectum; more common post-hysterectomy |
| Rectocele | Posterior | Herniation of rectal mucosa through defect in posterior vaginal wall fibromuscular layer |
| Perineal descent | Posterior | Perineum descends below ischial tuberosities during Valsalva; can progress to pudendal neuropathy |
- Berek & Novak's Gynecology, pp. 1664-1665
Pathophysiology
The etiology is multifactorial:
- Direct muscle trauma - Vaginal delivery causes visible levator ani defects in up to 20% of primiparous women on MRI; nearly absent after elective cesarean section.
- Denervation injury - Pudendal nerve and S3-S5 levator nerves are vulnerable during vaginal delivery. Evidence of neuropathy is found in 24-29% of primiparous women at 6 weeks to 6 months postpartum.
- Connective tissue failure - Altered collagen metabolism (ratio of type I:III collagen) underlies ligamentous failure. Connective tissue disorders (Ehlers-Danlos, Marfan syndrome) substantially increase POP risk.
- Aging - Progressive loss of smooth and striated muscle with increase in collagen/connective tissue; apoptotic changes in pelvic floor tissues occur with age.
- Chronic straining/increased intra-abdominal pressure - Worsens fascial stretching and ligament failure over time.
- Campbell-Walsh-Wein Urology, pp. 3415-3417
Clinical Features and Symptoms
Most specific symptom: A visible or palpable vaginal bulge.
Other symptoms include:
- Pelvic pressure or discomfort
- Sensation of incomplete bladder or bowel emptying
- Need to splint (digitate) the vaginal wall or perineum to urinate or defecate
- Low backache
- Urinary symptoms: frequency, nocturia, urgency (OAB), difficulty voiding
- Stress urinary incontinence (SUI): prevalence of SUI actually decreases as prolapse extends beyond the hymen (due to urethral kinking causing obstruction), creating "occult SUI" that may unmask after surgical repair
- Bowel symptoms (constipation, fecal incontinence) - weak correlation with prolapse severity; constipation alone without a bulge sensation rarely justifies surgery
- Sexual dysfunction - POP negatively affects body image and sexual function
Note: There is a much stronger correlation between symptoms (bulge, need to splint) and prolapse that extends beyond the hymen.
- Campbell-Walsh-Wein Urology, pp. 3405-3406
Staging / Grading
POP-Q System (Recommended)
The Pelvic Organ Prolapse Quantification (POP-Q) system, developed in 1993 and updated in 2002, is the current IUGA/ICS-recommended staging system. It uses the hymenal ring as a fixed reference point (zero), with negative values inside the introitus and positive values representing prolapse beyond the introitus.
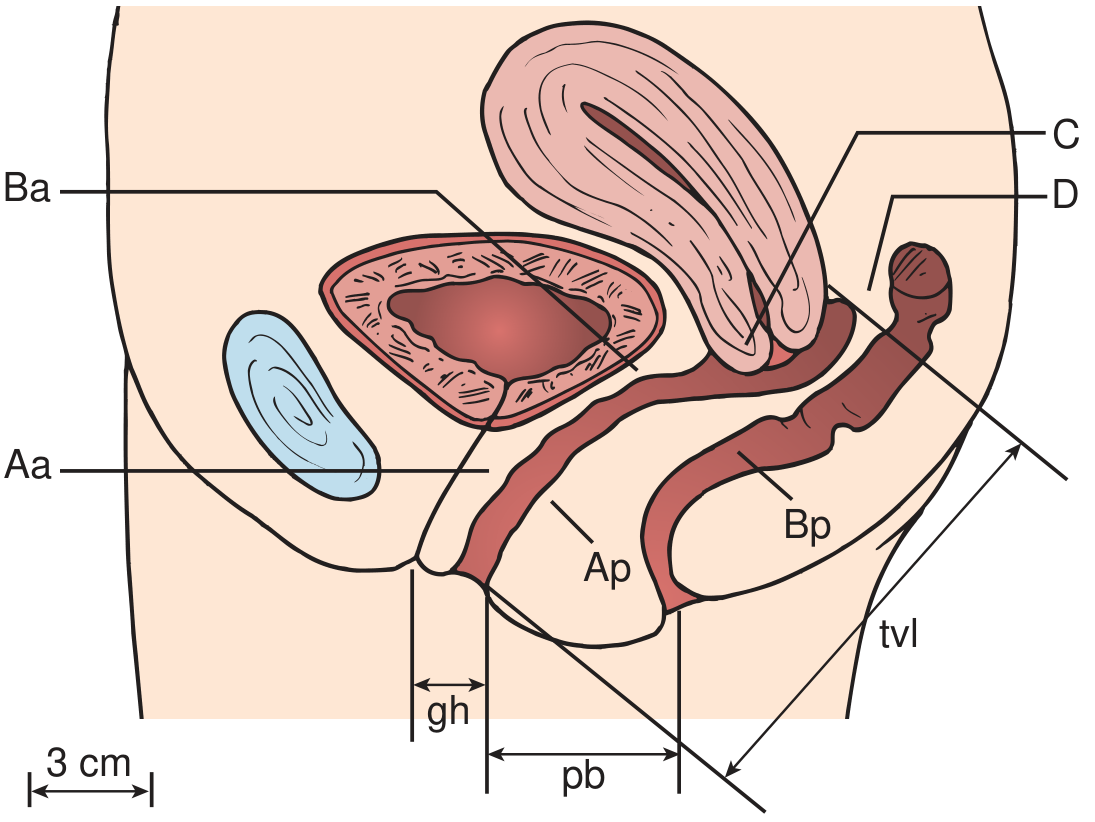
Nine measurement points:
| Point | Location | Normal Value |
|---|---|---|
| Aa | Anterior wall, 3 cm proximal to hymen (~ urethrovesical junction) | -3 cm |
| Ba | Most distal point of anterior wall prolapse | -3 cm |
| C | Leading edge of cervix or vaginal cuff | Variable |
| D | Posterior fornix (omitted after hysterectomy) | Variable |
| Ap | Posterior wall, 3 cm proximal to hymen | -3 cm |
| Bp | Most distal point of posterior wall prolapse | -3 cm |
| gh | Genital hiatus (urethral meatus to posterior hymenal ring) | - |
| pb | Perineal body (posterior gh to mid-anal opening) | - |
| tvl | Total vaginal length at rest | - |
POP-Q Stages:
| Stage | Description |
|---|---|
| 0 | No prolapse; all points at -3 cm or above |
| I | Leading edge > 1 cm above hymen (< -1) |
| II | Leading edge within 1 cm of hymen (-1 to +1) |
| III | Leading edge > 1 cm below hymen but < tvl - 2 |
| IV | Complete eversion (leading edge ≥ tvl - 2) |
Baden-Walker system (older): Uses four grades (0-3) relative to the hymen at six midline sites; less precise but still encountered clinically.
- Campbell-Walsh-Wein Urology, pp. 3406-3408
Evaluation
- History: Symptoms, prior deliveries, prior surgeries, bowel/bladder function, sexual activity, desire to preserve uterus
- Physical exam: Assess all three compartments (anterior, apical, posterior) with Valsalva/straining; assess levator ani and anal sphincter
- Urodynamics: Helpful pre-operatively, especially with prolapse reduction to identify occult SUI (urodynamic SUI during reduction predicts ~58% postoperative SUI risk if no anti-incontinence procedure performed)
- Pessary trial: Useful to confirm that symptoms are attributable to prolapse; improvement with pessary suggests surgical repair is likely to help
Treatment
1. Conservative / Non-surgical
- Pelvic floor muscle training (Kegel exercises): First-line for mild-to-moderate POP; strengthens the levator ani to partially compensate for structural defects.
- Lifestyle modification: Weight loss, avoidance of heavy lifting, treatment of chronic cough/constipation.
- Vaginal estrogen: Particularly in postmenopausal women; improves tissue quality and helps prevent pessary-related complications.
2. Mechanical Devices - Pessaries
Pessaries are an effective, reversible option for all grades of POP, especially useful in elderly or medically unfit patients.
-
Come in wide variety of shapes and sizes (ring, Gellhorn, cube, donut); must be individually fitted.
-
When correctly sized, the patient cannot feel it; too small = falls out; too large = discomfort or erosion.
-
Must be removed and cleaned periodically with inspection of tissue integrity.
-
Concomitant vaginal estrogen reduces erosion risk.
-
Factors associated with long-term success: age ≥72, careful fitting, clear patient instructions.
-
Successful pessary use improves quality of life and body image.
-
Campbell-Walsh-Wein Urology, p. 3860
3. Surgical Management
Surgery is individualized based on compartment(s) involved, patient's activity level, desire for future sexual function, and uterine preservation preference.
Vaginal Procedures
| Procedure | Indication | Notes |
|---|---|---|
| Anterior colporrhaphy | Anterior wall (cystocele) | Plication of pubocervical fascia |
| Paravaginal repair | Lateral cystocele defects | Reattaches vaginal wall to arcus tendineus |
| Posterior colporrhaphy | Posterior wall (rectocele) | Anatomic cure 76-96%; does NOT reliably treat constipation; dyspareunia in 7-26% (avoid levator plication) |
| Sacrospinous ligament fixation (SSLF) | Apical prolapse | Unilateral or bilateral; vaginal approach |
| Uterosacral ligament suspension | Apical prolapse | Vaginal or laparoscopic |
Abdominal Procedures
| Procedure | Notes |
|---|---|
| Abdominal sacrocolpopexy | Gold standard for apical vault prolapse; attaches vaginal apex to sacral promontory via mesh; can be open, laparoscopic, or robotic |
| Abdominal uterosacral suspension | For apical support |
| Sacral colpoperineopexy | For perineal descent with rectal prolapse; suture rectopexy may be added |
Obliterative Procedures
- Colpocleisis (LeFort or total colpectomy): For women who no longer desire vaginal intercourse; high success rates with low morbidity; suitable for elderly or high-risk patients.
Mesh Considerations
- Transvaginal mesh for anterior/posterior repair was associated with serious complications (erosion, dyspareunia, pain) - the FDA restricted its use in 2019.
- Abdominal/laparoscopic/robotic sacrocolpopexy with mesh remains the standard for apical prolapse.
Concomitant Anti-Incontinence Procedures
-
Women with occult SUI (demonstrated during prolapse reduction on urodynamics) should be counseled about adding a mid-urethral sling at time of prolapse repair.
-
Women with OAB symptoms often have improvement after prolapse repair (anterior repair reduced frequency by 33%, urge urinary incontinence by 49% in one study).
-
Berek & Novak's Gynecology, pp. 1073-1099; Campbell-Walsh-Wein Urology, pp. 3406-3410
Key Risk Factors Summary
- Vaginal delivery (most important modifiable risk factor)
- Advanced age
- Obesity and chronic increased intra-abdominal pressure
- Prior pelvic surgery (hysterectomy increases enterocele risk)
- Connective tissue disorders (Ehlers-Danlos, Marfan)
- Chronic straining (constipation, chronic cough)
- Ethnicity (White women have higher rates than African American; Hispanic and Asian women intermediate)
Recent Evidence (2024-2026)
- A 2024 systematic review and meta-analysis found reduced type III collagen RNA expression in women with POP vs. controls, supporting the role of connective tissue dysregulation in POP pathogenesis [PMID: 39352428].
- A 2025 Cochrane review examined perioperative interventions in POP surgery to optimize outcomes [PMID: 40693510].
- A 2025 meta-analysis found associations between hysterectomy and pelvic floor disorders including POP [PMID: 40120730].
Sources: Campbell-Walsh-Wein Urology (9th ed.) | Berek & Novak's Gynecology | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.