Shaft of humerus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
I now have enough material to write a thorough, well-illustrated answer. Let me compile everything.
Shaft of the Humerus
Gross Anatomy
The shaft (diaphysis) of the humerus extends from just below the surgical neck superiorly to the supraepicondylar ridges inferiorly. In cross-section it is roughly triangular, with:
- 3 borders: anterior, medial, lateral
- 3 surfaces: anterolateral, anteromedial, posterior
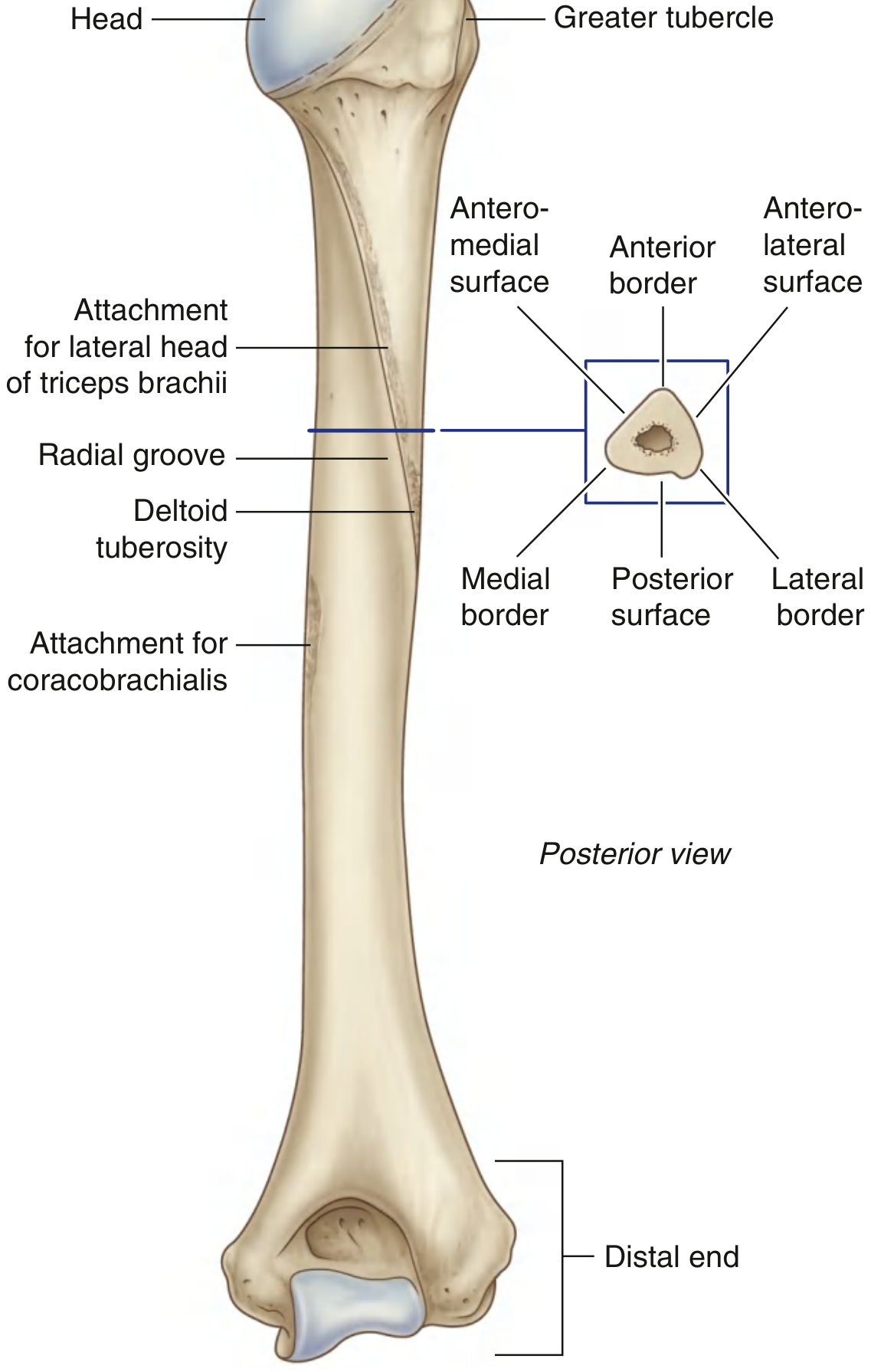
Key Surface Markings
| Feature | Location | Significance |
|---|---|---|
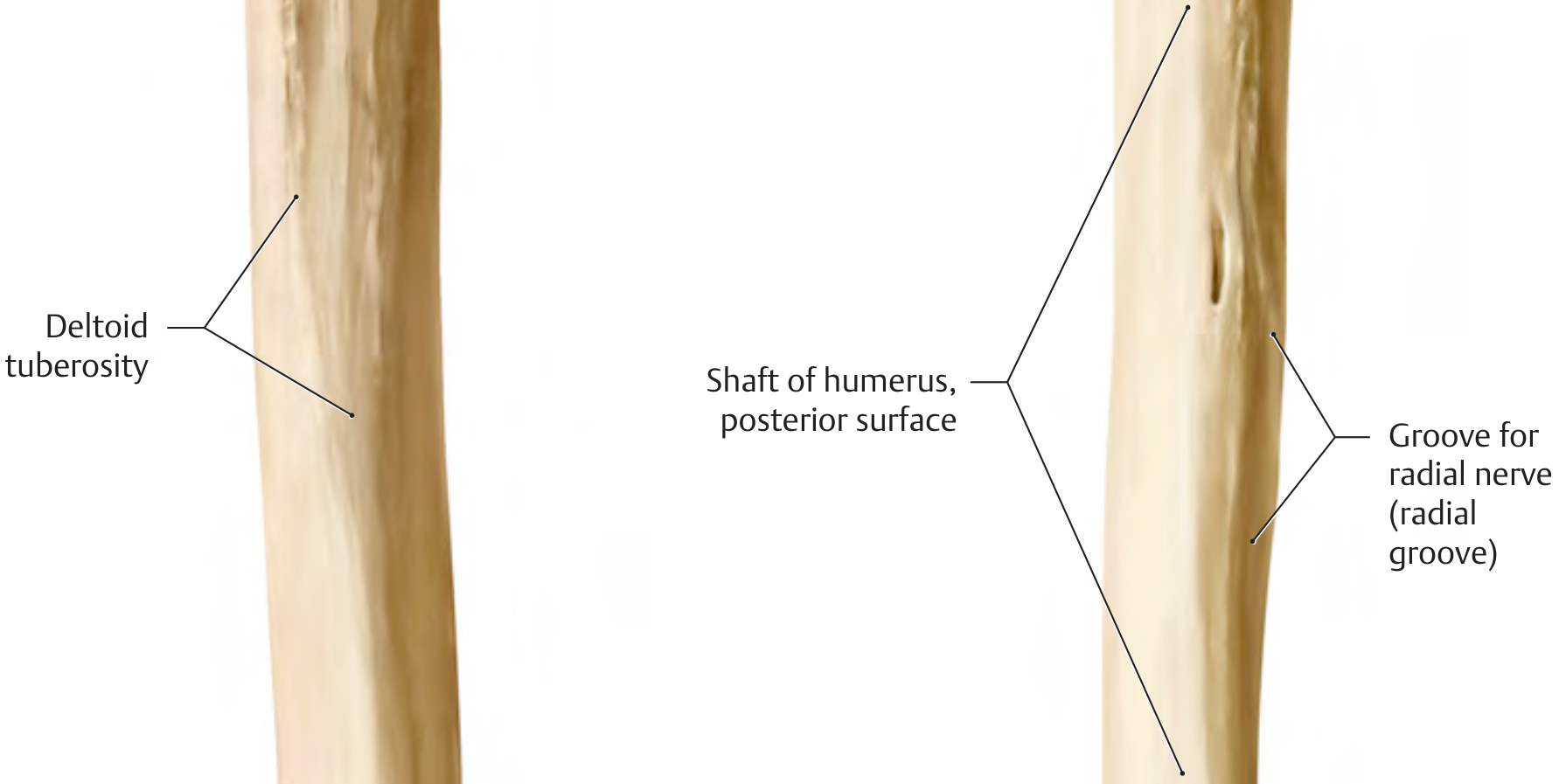
| Deltoid tuberosity | Middle of anterolateral surface | Insertion of deltoid muscle |
| Radial groove (spiral groove) | Posterior surface, runs obliquely | Contains radial nerve + profunda brachii artery |
| Attachment for lateral head of triceps | Superior posterior surface | Begins just below surgical neck, runs to deltoid tuberosity |
| Attachment for coracobrachialis | Middle of medial border | Thin elongated roughening |
| Medial & lateral borders | Give rise distally | Expand into medial/lateral supraepicondylar ridges |
Important Relations
Radial Groove
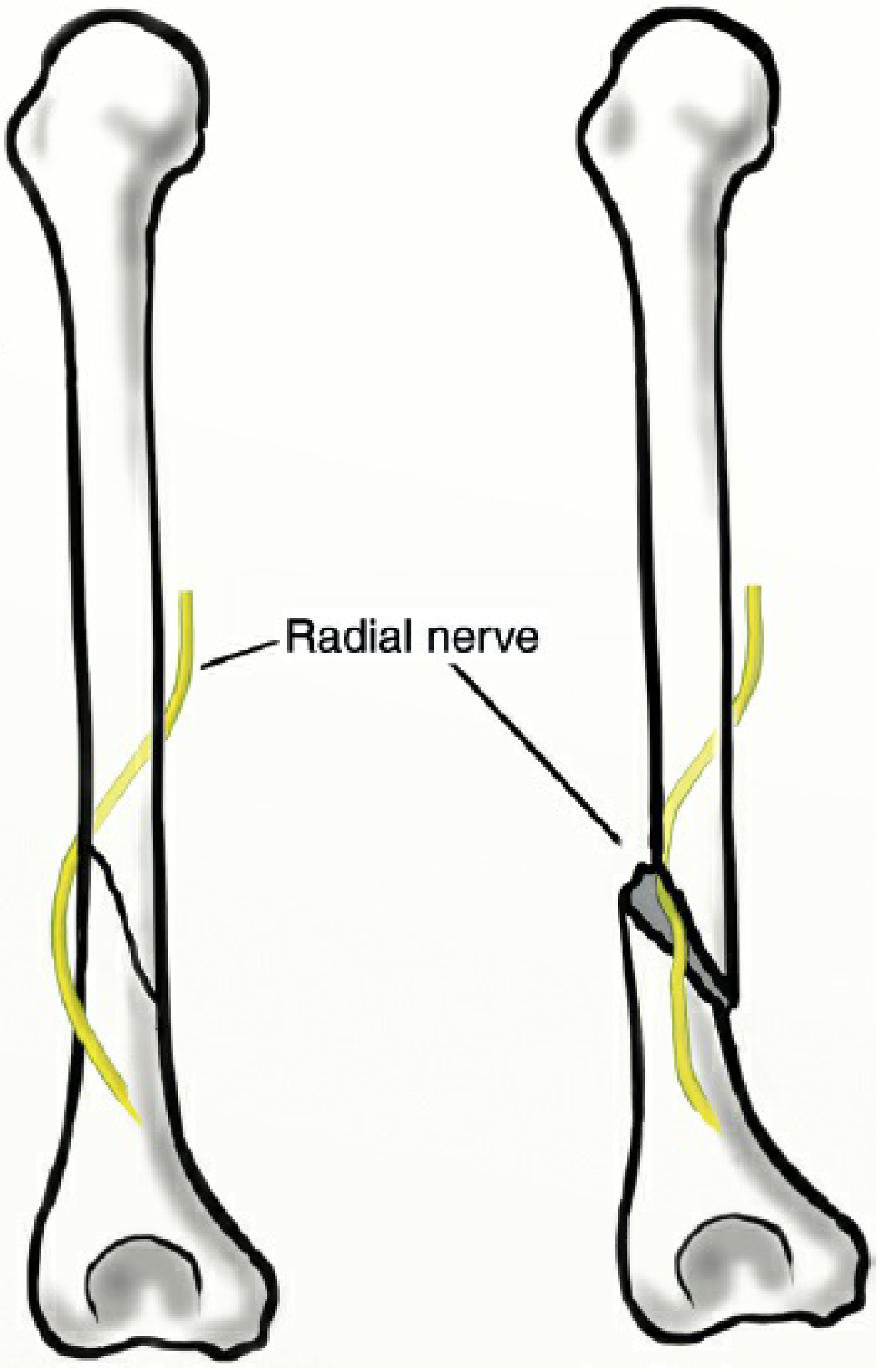
The radial groove (spiral groove) runs diagonally down the posterior surface, parallel to the posterior margin of the deltoid tuberosity. It lodges:
- Radial nerve (posterior cord of brachial plexus, C5-C8, T1)
- Profunda brachii artery (deep brachial artery)
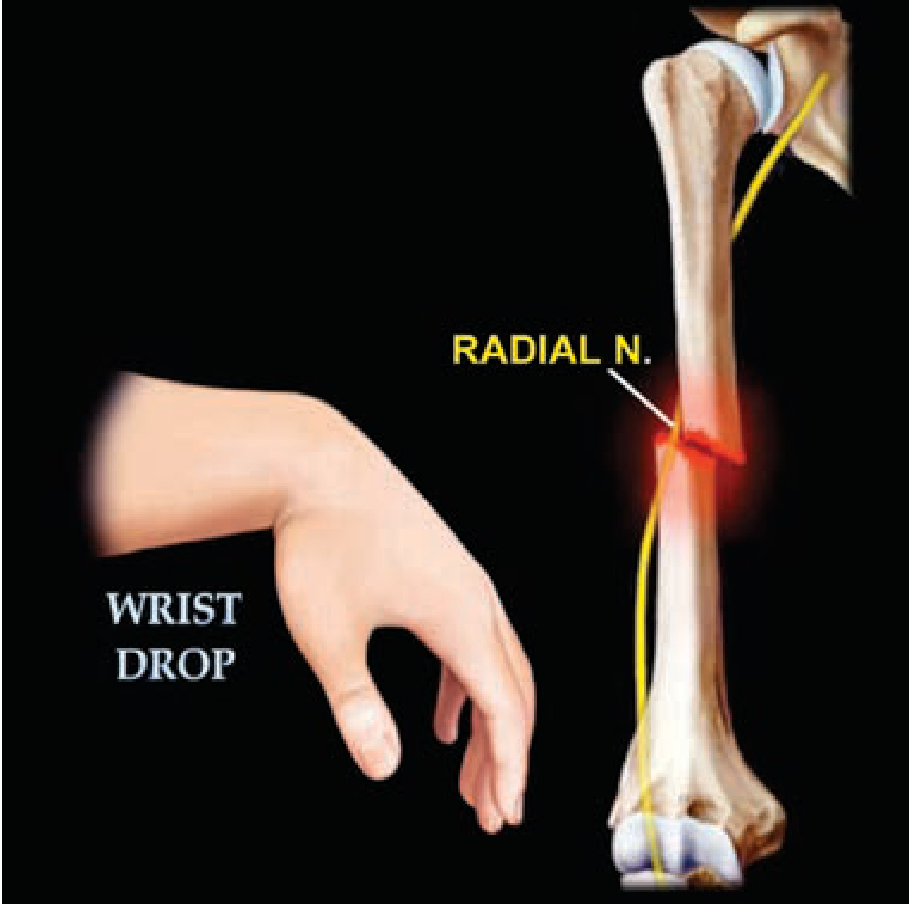
The nerve winds from the posterior compartment to the anterior compartment of the arm here, making it vulnerable in mid-shaft fractures.
Intermuscular Septa
The medial and lateral intermuscular septa attach to the corresponding borders of the shaft and divide the arm into anterior (flexor) and posterior (extensor) compartments.
Muscle Attachments (Summary)
| Muscle | Attachment |
|---|---|
| Deltoid | Inserts into deltoid tuberosity (anterolateral shaft, middle) |
| Coracobrachialis | Inserts on medial border, middle third |
| Lateral head of triceps | Originates from posterior surface above radial groove |
| Medial head of triceps | Originates from posterior surface below radial groove |
| Brachialis | Originates from distal half of anterior surface |
| Pectoralis major | Inserts into lateral lip of bicipital groove (upper shaft) |
| Teres major | Inserts into medial lip of bicipital groove (upper shaft) |
| Latissimus dorsi | Inserts into floor of bicipital groove (upper shaft) |
Fracture Displacement Patterns
Displacement depends on the level of fracture relative to muscle attachments:
- Above pectoralis major insertion: proximal fragment abducted + externally rotated by rotator cuff; distal fragment pulled medially by pectoralis major
- Between pectoralis major and deltoid insertions: proximal fragment adducted by pectoralis major; distal fragment pulled laterally and superiorly by deltoid
- Below deltoid insertion: proximal fragment abducted by deltoid; distal fragment pulled superiorly by biceps and triceps
Clinical: Humeral Shaft Fractures
Mechanism
- Most common: direct blow, severe twist, or fall on outstretched hand
- Rare: abrupt muscle contraction (e.g., throwing a javelin or baseball)
- Most commonly fracture in the middle third, in a transverse pattern
Clinical Features
- Localized severe pain, arm swelling, inability to use the arm
- Bony crepitus with any manipulation in complete fractures
- Shortening or rotation depending on displacement
- Incomplete fractures show only tenderness and swelling without deformity
(Rosen's Emergency Medicine)
Holstein-Lewis Fracture
A spiral or oblique fracture of the distal third of the humeral shaft. Clinically important because the radial nerve is tethered as it pierces the lateral intermuscular septum at this level - making entrapment between fracture fragments far more likely than at other levels.
- Radial nerve palsy occurs in 5-10% of humeral shaft fractures overall, but up to 22% in distal-third fractures
- Up to 92% of radial nerve palsies in closed fractures resolve with 3-4 months of observation
Treatment
Non-operative (preferred for most closed fractures)
- Acceptable if: <20° anterior angulation, <30° valgus/varus, <3 cm shortening
- Coaptation ("sugar-tong") splint + sling-and-swathe initially
- Replaced by a functional brace at 10-14 days
- Hanging cast for grossly displaced or spiral fractures
- Radial nerve palsy alone is NOT an indication for surgery - observe for 3-4 months
Operative Indications (ORIF)
- Polytrauma - facilitates early mobilization
- Gross mobility at 6 weeks (predicts nonunion)
- Floating elbow
- Pathologic fracture
- Open fracture
- Secondary (post-manipulation) radial nerve palsy - controversial
Fixation Options
| Method | Notes |
|---|---|
| Plate (gold standard) | Proximal 2/3 - anterolateral approach (lowest radial nerve palsy risk); Distal half - posterior approach; Lateral approach has highest nerve palsy risk |
| IM nail | Consider for pathologic or segmental fractures; causes more shoulder pain; risk to radial nerve (lateral-to-medial distal locking screw) and musculocutaneous nerve (AP screw) |
(Miller's Review of Orthopaedics 9th Ed; Rosen's Emergency Medicine)
Radial Nerve Palsy - Recovery Milestones
Recovery follows a proximal-to-distal pattern:
- Brachioradialis - first to return
- Extensor carpi radialis longus (wrist extension in radial deviation)
- Extensor pollicis longus and extensor indicis proprius - last to return
(Miller's Review of Orthopaedics 9th Ed)
Shaft of humerus fracture
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the best sources. Let me compile the full, well-organized answer.
Fractures of the Shaft of the Humerus
Epidemiology
- Account for 1-2% of all fractures and 13-14% of all humeral fractures
- Bimodal age distribution:
- Young males: high-energy trauma (e.g., road traffic accidents, sports)
- Elderly females: low-energy fall from standing height
- After age 60, fractures are more common in women following a simple ground-level fall
- Annual incidence: 10-20 per 100,000 population
- Location: Middle third most common (47-64%), followed by proximal third (15-30%), then distal third (11-35%)
(Rockwood & Green's Fractures in Adults, 10th ed., 2025)
Mechanism of Injury
| Mechanism | Fracture Pattern |
|---|---|
| Direct blow to the arm | Transverse or comminuted |
| Indirect twisting force (fall, sports) | Spiral or oblique |
| Fall on outstretched hand | Oblique |
| Abrupt muscle contraction (throwing) | Spiral (rare) |
| Pathologic bone (metastasis, cyst) | Any pattern, often minor trauma |
Classification
By Location
- Proximal third - typically oblique
- Middle third - typically transverse (most common)
- Distal third - often oblique/spiral; highest risk of radial nerve injury
AO/OTA Classification
- Type A: Simple (A1 = spiral, A2 = oblique ≥30°, A3 = transverse <30°)
- Type B: Wedge (B1 = spiral wedge, B2 = bending wedge, B3 = fragmented wedge)
- Type C: Complex/comminuted (C1 = spiral, C2 = segmental, C3 = irregular)
Displacement Patterns (Depend on Level Relative to Muscle Insertions)
| Fracture Level | Proximal Fragment | Distal Fragment |
|---|---|---|
| Above pectoralis major | Abducted + ER (rotator cuff) | Medial (pect. major) |
| Between pect. major & deltoid | Adducted (pect. major) | Lateral + superior (deltoid) |
| Below deltoid | Abducted (deltoid) | Superior (biceps + triceps) |
Clinical Features
- Severe, localized arm pain; arm hangs useless
- Swelling and ecchymosis over the arm
- Visible deformity - shortening or rotational malalignment in displaced fractures
- Bony crepitus with the slightest manipulation (complete fractures)
- Incomplete fractures: local tenderness + swelling without deformity
- Always examine radial nerve - check wrist and finger extension before and after any manipulation or splinting
Associated Injuries
Radial Nerve Palsy (Most Important Complication)
- Occurs in 10-12% of closed humeral shaft fractures overall
- Up to 22% with distal-third fractures
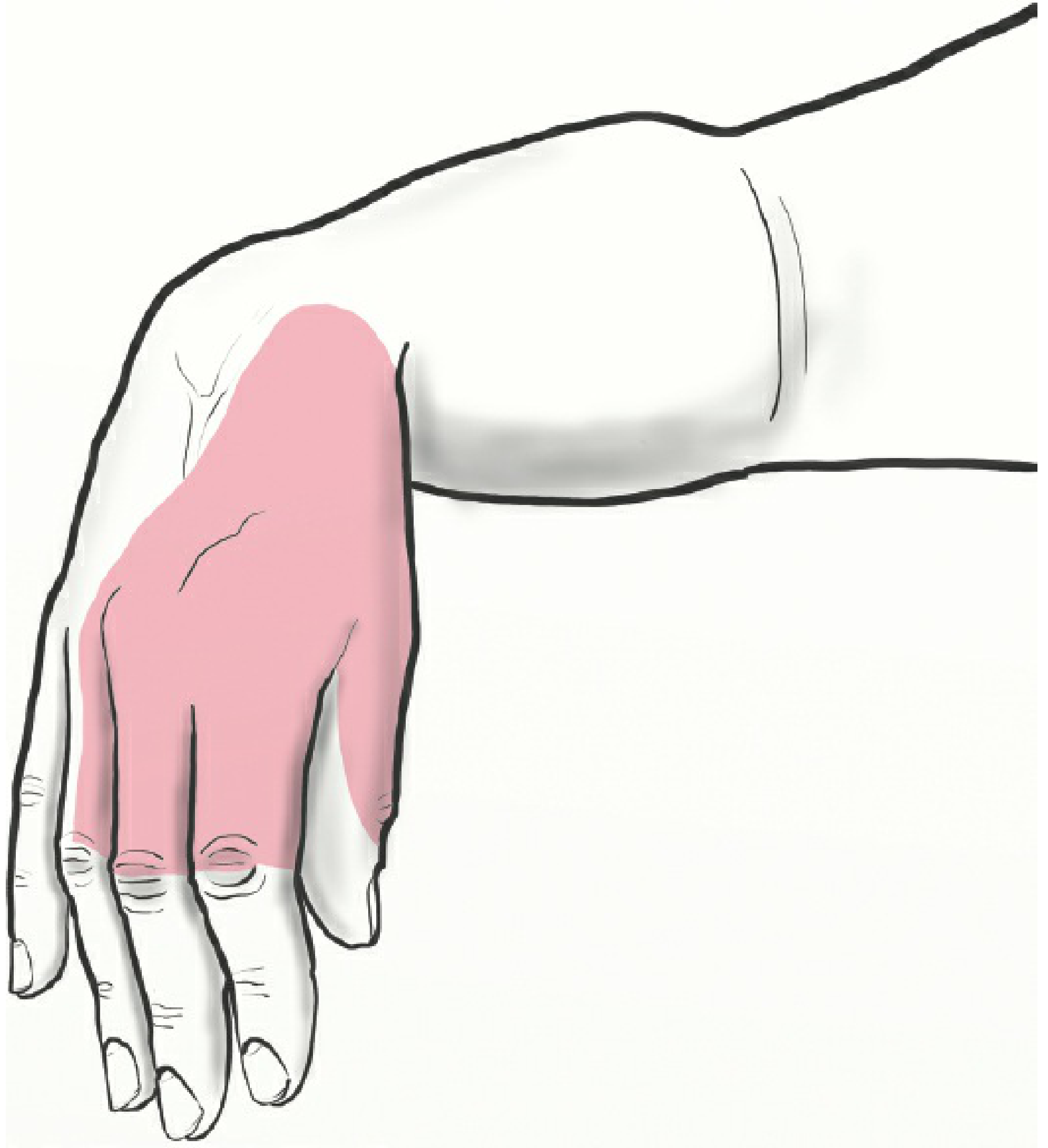
Clinical picture of radial nerve palsy:
- Wrist drop (inability to dorsiflex wrist and digits)
- Numbness over dorsoradial hand and dorsal aspect of radial 3.5 digits
Holstein-Lewis Fracture
A spiral fracture of the distal third where the distal fragment deviates radially, tethering the radial nerve as it pierces the lateral intermuscular septum. The nerve is at high risk of entrapment between the fracture fragments. First described by Holstein and Lewis in 1963.
Vascular Injury
- Brachial artery injury is uncommon but can occur, particularly with high-energy trauma or open fractures
- Always check distal pulses
Brachial Plexus Injury
- Can be associated, especially with high-energy trauma
Investigations
- X-rays: AP + lateral views of the entire humerus including the shoulder and elbow joints (mandatory)
- Look for pathologic features: cortical thinning, abnormal osteoblastic/osteoclastic activity - consider bone metastasis (humerus is a common site)
- CT: Useful for complex or comminuted fractures or pre-operative planning
- MRI/bone scan: If pathologic fracture is suspected
- EMG/nerve conduction: Baseline and to monitor recovery of radial nerve palsy at 3-4 weeks, then serially
Treatment
Acceptable Alignment (for Non-operative Management)
- < 20° anterior angulation
- < 30° varus/valgus angulation
- < 3 cm shortening
Non-operative Treatment (First-Line for Most Closed Fractures)
Most isolated closed humeral shaft fractures heal with conservative management.
| Method | Indication | Notes |
|---|---|---|
| Coaptation ("sugar-tong") splint + sling-and-swathe | Initial immobilization for all fractures | Placed from deltoid, under elbow, up into axilla |
| Functional brace (clamshell plastic brace + Velcro) | Replaces coaptation splint at 10-14 days | Gold standard for definitive conservative treatment |
| Hanging arm cast | Grossly displaced or spiral fractures | Gravity provides traction; patient must remain upright; not well tolerated by many |
- Gentle motion exercises begin within 1-2 weeks
- Serial radiographs to verify healing
- Radial nerve palsy alone is NOT a contraindication to conservative treatment - up to 92% resolve spontaneously within 3-6 months
Operative Indications
| Indication | Notes |
|---|---|
| Polytrauma | Facilitates early mobilization and upper extremity weight bearing |
| Gross mobility at 6 weeks post-injury | Predicts nonunion; proceed to ORIF |
| Floating elbow (ipsilateral forearm fracture) | |
| Open fracture | Wash out + fixation |
| Pathologic fracture | Stabilize + treat underlying cause |
| Vascular injury requiring repair | Stabilize bone first |
| Secondary radial nerve palsy (after manipulation) | Controversial - suggests nerve entrapment |
| Bilateral humeral fractures |
Fixation Options
1. Plate fixation (Gold Standard)
| Approach | Use |
|---|---|
| Anterolateral approach | Proximal 2/3 of shaft - lowest incidence of radial nerve palsy |
| Posterior approach | Distal half of shaft |
| Lateral approach | Highest incidence of radial nerve palsy - generally avoid |
- Weight bearing to tolerance is safe after plate fixation
- Allows early mobilization
2. Intramedullary (IM) Nail
- Consider for: pathologic fractures, segmental fractures
- Disadvantages vs. plate:
- More shoulder pain (from proximal nail entry)
- Risk of radial nerve injury with lateral-to-medial distal locking screw
- Risk of musculocutaneous nerve with AP distal locking screw
Radial Nerve Palsy - Management
| Situation | Action |
|---|---|
| Closed fracture, palsy present at time of injury | Observe expectantly (most are neuropraxia); EMG at 3-4 weeks; wait up to 6 months for recovery |
| Closed fracture, palsy appears AFTER manipulation/reduction | Urgent exploration - suggests nerve entrapment between fragments |
| Open fracture with palsy | Explore nerve at time of surgical fixation |
| Gunshot/penetrating wound with palsy | Explore nerve |
| No recovery at 6 months | Surgical exploration ± nerve grafting ± tendon transfers |
Recovery Order (Proximal to Distal)
- Brachioradialis (first)
- Extensor carpi radialis longus (wrist extension in radial deviation)
- Extensor carpi radialis brevis
- Extensor pollicis longus + extensor indicis proprius (last)
Complications
| Complication | Details |
|---|---|
| Radial nerve palsy | 10-12% overall; 22% in distal-third fractures; 92% resolve with observation |
| Nonunion | ~10%; risk factors: distraction, insufficient immobilization, infection, pathologic bone |
| Malunion | Varus/valgus or rotational deformity |
| Infection | Higher in open fractures |
| Shoulder stiffness | Particularly with IM nailing |
| Iatrogenic nerve injury | Radial nerve in lateral approach; musculocutaneous with IM nail |
Special Situations
Children
- Humeral shaft fractures in children are uncommon (<10% of all humeral fractures)
- Peak in <3 years or >12 years
- Nearly all treated non-operatively given remodeling potential
- Acceptable angulation: up to 70° in children <5 years, 30° in ages 12-13
- Radial nerve entrapment can occur after closed reduction - loss of radial nerve function after reduction = urgent nerve exploration (Campbell's Operative Orthopaedics, 15th ed.)
Pathologic Fractures
- Humerus is a common site for bone metastases, unicameral bone cysts, and primary bone tumors
- Cortical thinning and abnormal bone activity on X-ray are warning signs
- Require multidisciplinary management with oncology
- Stabilization options: plates, IM nails, cement, joint replacement - but underlying pathology must be treated concurrently for healing
(Sources: Rockwood & Green's Fractures in Adults 10th ed. 2025; Campbell's Operative Orthopaedics 15th ed. 2026; Schwartz's Principles of Surgery 11th ed.; Miller's Review of Orthopaedics 9th ed.)
Triceps splitting approach to hunerus
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed. Let me compile a comprehensive, well-illustrated answer.
Triceps-Splitting Approach to the Humerus
Overview
The triceps-splitting approach is a posterior approach to the humerus. It provides access to the distal two-thirds of the posterior humeral shaft - from the olecranon fossa up to the junction of the proximal and middle thirds. It is one of several posterior approaches, alongside the triceps-reflecting (TRAP) and paratricipital approaches.
The approach was described by Campbell and involves a midline split through the triceps muscle and tendon to expose the posterior humerus.
Indications
- Humeral shaft fractures of the middle third and distal third
- Distal humeral fractures requiring ORIF
- Can be used as a preliminary to Total Elbow Arthroplasty (TEA) - the ability to convert from ORIF to TEA intraoperatively is a major advantage
- Outerbridge-Kashiwagi procedure (ulnohumeral arthroplasty) for elbow arthritis
- Bridge plating for complex distal humerus/periarticular fractures
- Preferred over anterolateral approach for fractures of the distal half of the humeral shaft
Positioning
- Prone or lateral decubitus position
- Arm abducted 90° on a radiolucent arm support
- This allows the elbow to flex freely during the approach, which is important for improving exposure
Surgical Technique (Step by Step)
Skin Incision
Longitudinal midline incision along the posterior aspect of the arm, from the tip of the olecranon to approximately 5-10 cm distal to the acromion.
Step 1 - Identify the Interval (Superficial Dissection)
At the proximal end of the incision, identify and develop the interval between the long head (medial) and lateral head (lateral) of the triceps by blunt dissection.
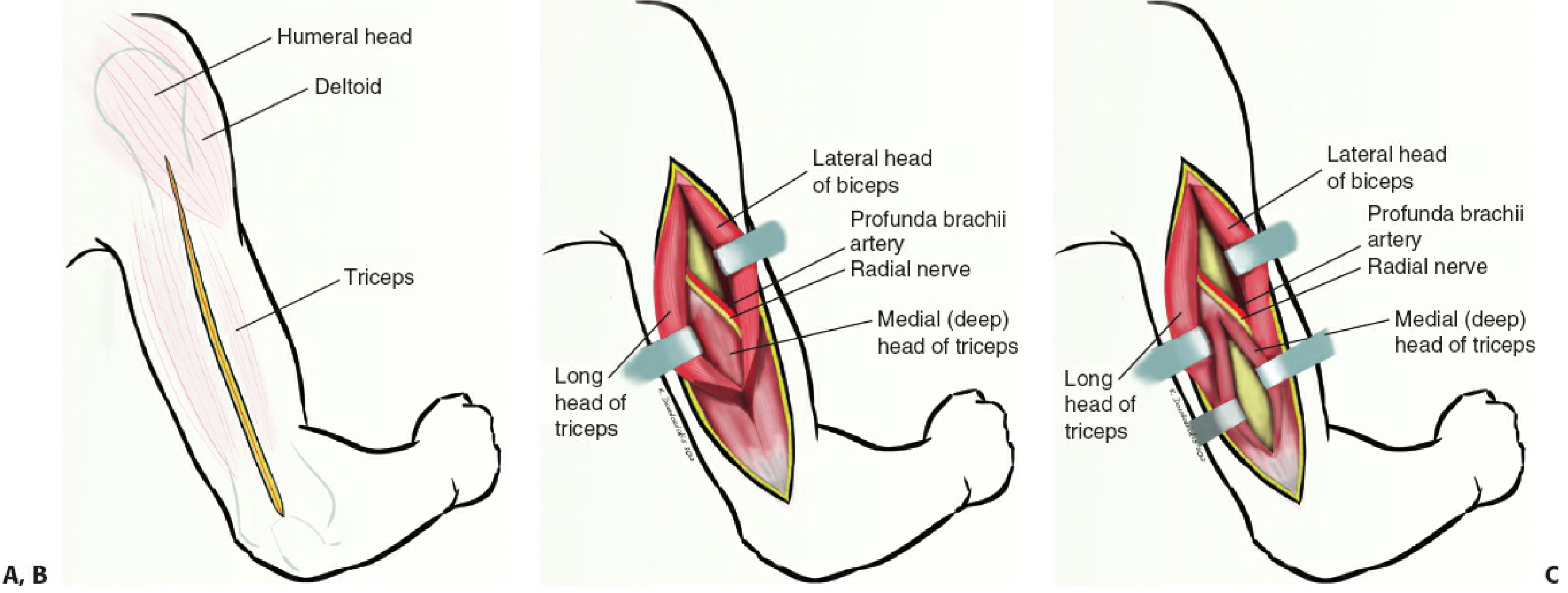
Key landmark: As you retract the lateral head laterally and the long head medially at the proximal part, the radial nerve and profunda brachii artery are exposed as they run together in the spiral groove.
- The radial nerve lies approximately 39 ± 2.1 mm from the point of confluence between the long and lateral heads of the triceps and the triceps aponeurosis.
- The first branch identifiable at the lateral septum is the lateral sensory branch of the radial nerve - trace it proximally to find the main radial nerve.
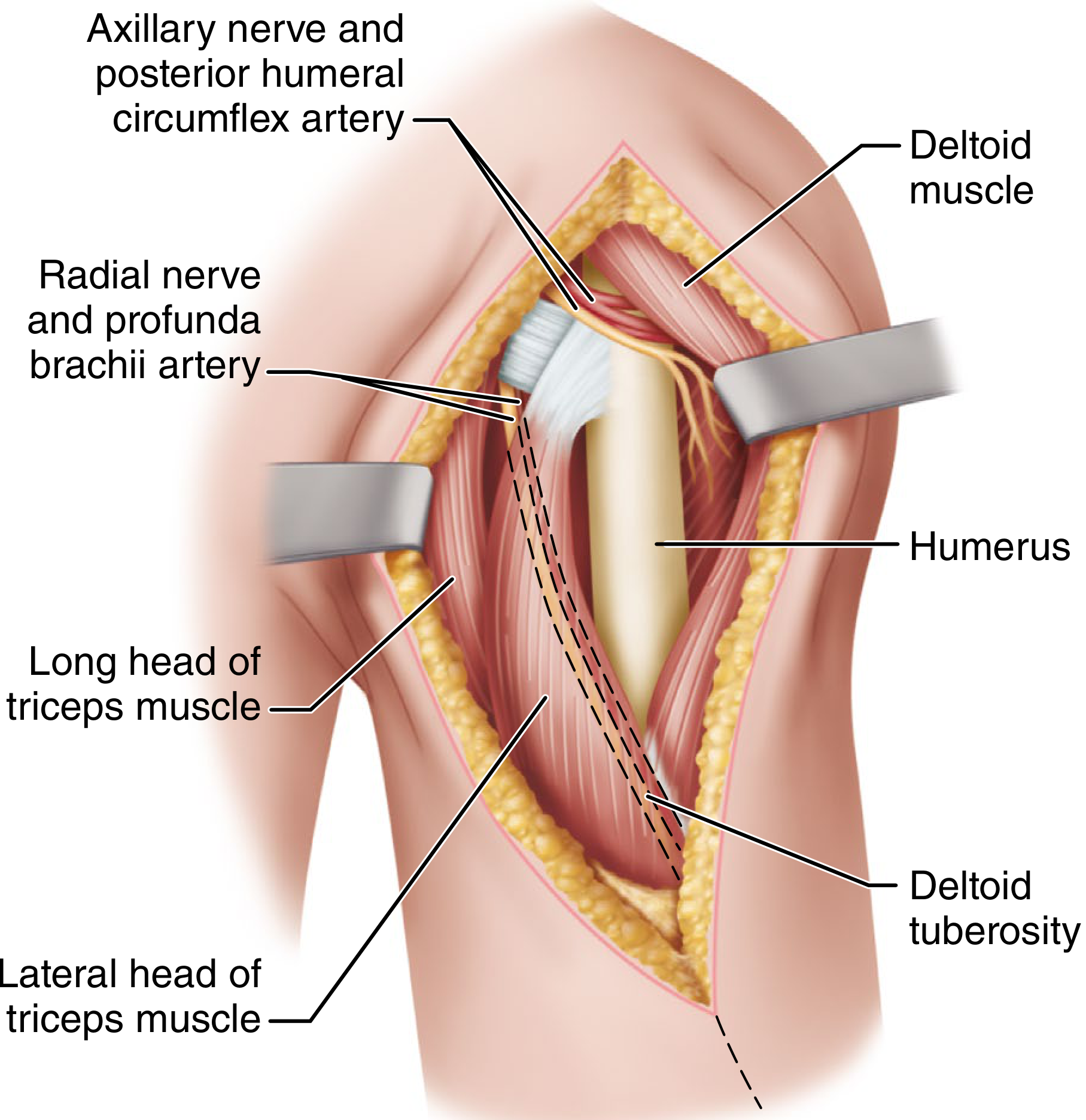
Step 2 - Deep Dissection (Midline Split)
Incise the common triceps tendon sharply in the midline as it runs distally toward the olecranon. Extend this split through the medial (deep) head of the triceps longitudinally in the midline.
- The medial head originates just distal to the spiral groove and is the deepest layer
- Longitudinal midline dissection through it reveals the periosteum of the posterior humeral shaft
Step 3 - Periosteal Elevation
Incise the periosteum longitudinally and elevate it with subperiosteal dissection outward from the midline in both directions, exposing the medial and lateral columns.
- The medial and lateral columns of the distal humerus are exposed
- Periosteal retraction also protects the radial, ulnar, and lateral brachial cutaneous nerves
Step 4 - Distal Extension (if needed)
To extend distally, continue the midline split through the triceps insertion on the olecranon:
- Release Sharpey fibers to create medial and lateral fasciotendinous sleeves
- This allows access to the olecranon fossa and articular surface
Tip: Visualization of the articular surface of the distal humerus can be improved by partial excision of the olecranon tip and flexion of the elbow.
Step 5 - Proximal Extension (if needed)
The approach can be extended proximally to the level of the radial nerve as it crosses the humeral shaft in the spiral groove.
- With mobilization of the radial nerve, access to the posterior humerus increases from 55% to 76% of the shaft.
Closure
The triceps tendon is repaired to the olecranon using transosseous non-absorbable braided sutures through bone tunnels. Gschwend's modification incorporates a small flake of olecranon bone to improve triceps healing.
Anatomical Interval
| Detail | |
|---|---|
| True internervous plane | None - the triceps (all heads) is innervated by the radial nerve; the split is within a single muscle |
| Superficial split | Between lateral head (radial n.) and long head (radial n.) of triceps |
| Deep split | Through medial head (radial n.) of triceps |
| Nerve at risk | Radial nerve in the spiral groove (identify and protect at the proximal part of the incision) |
| Also at risk | Ulnar nerve distally; axillary nerve proximally if extended |
Access Provided
| Region | Accessible? |
|---|---|
| Distal third of humeral shaft | Yes - best exposure |
| Middle third of humeral shaft | Yes |
| Proximal third of humeral shaft | Limited (requires radial nerve mobilization) |
| Distal humerus (columns + articular) | Yes, with distal extension |
Advantages
- Relatively technically straightforward
- Can be extended proximally and distally as needed
- Ability to convert from ORIF to TEA intraoperatively with minimal additional steps
- No bone osteotomy required (unlike olecranon osteotomy)
- McKee et al. showed no significant difference in extensor mechanism strength between triceps-splitting and olecranon osteotomy approaches
Disadvantages
- Limited visibility of the articular surface - not ideal for highly comminuted intra-articular distal humerus fractures
- Requires postoperative protection of the triceps repair - risk of extensor mechanism disruption
- No true internervous plane (working within the radial nerve's territory throughout)
- Triceps splitting at the olecranon insertion risks extensor weakness or dehiscence
Postoperative Care
- Patients with triceps-splitting approach are restricted to gravity-assisted range of motion initially (unlike paratricipital approach, where unrestricted active ROM is allowed)
- Triceps protection for approximately 6 weeks to allow tendon-to-bone healing
- Gentle flexion exercises permitted; active extension against resistance restricted early
Comparison with Other Posterior Approaches
| Approach | Key Feature | Best Used For |
|---|---|---|
| Triceps-splitting | Midline split through all 3 heads | Midshaft/distal fractures, ORIF, bridge plating, TEA |
| Paratricipital (triceps-sparing) | Medial + lateral windows, triceps left intact | Less risk of extensor weakness; limited articular visibility |
| Olecranon osteotomy | Osteotomy of olecranon tip | Best articular exposure for comminuted intra-articular fractures |
| TRAP approach | Triceps + anconeus reflected as one flap | TEA; avoids osteotomy complications |
| Van Gorder (triceps tongue) | V-Y plasty at musculotendinous junction | TEA, especially with associated triceps injury |
| Lateral triceps slide | Entire triceps mobilized medially | Alternative for proximal extension |
(Sources: Rockwood & Green's Fractures in Adults 10th ed. 2025; Campbell's Operative Orthopaedics 15th ed. 2026; Miller's Review of Orthopaedics 9th ed.)
Anterolateral approach to humerus
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I have everything needed for a thorough, well-illustrated answer. Let me compile it now.
Anterolateral Approach to the Humerus
Also called the Thompson-Henry approach or brachialis-splitting approach, this is the standard approach to the anterior and anterolateral humeral shaft. It is an extension of the deltopectoral interval and provides extensile exposure from the humeral head proximally to the coronoid fossa distally.
Indications
- Humeral shaft fractures of the proximal and middle thirds (preferred approach for these levels)
- ORIF of humeral diaphyseal fractures requiring anterolateral plate placement
- Lowest incidence of iatrogenic radial nerve palsy compared to the lateral and posterior approaches
- Pathologic lesions of the humeral shaft
- Brachial artery repair (can combine with medial approach)
- Can be combined with a volar Henry approach distally to extend into the forearm
Positioning
- Supine with the arm on an arm table, or lateral decubitus
- A padded support under the shoulder allows the arm to fall into slight abduction
- Elbow flexion to 90° during the distal part of the dissection relaxes the brachialis and improves exposure
Anatomical Intervals
The approach uses three different intervals as it descends the arm:
| Level | Interval / Plane |
|---|---|
| Proximal (shoulder region) | Between deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves) |
| Middle third of humerus | Longitudinal split of brachialis (dual innervation: radial nerve laterally, musculocutaneous nerve medially - splitting midline preserves both) |
| Distal third of humerus | Between brachialis (medially) and brachioradialis (laterally), both radial nerve |
This approach is extensile but not truly internervous at all levels - the brachialis split in the middle third is the key "safe" plane because the dual nerve supply allows longitudinal splitting without paralysis.
Surgical Technique (Step by Step)
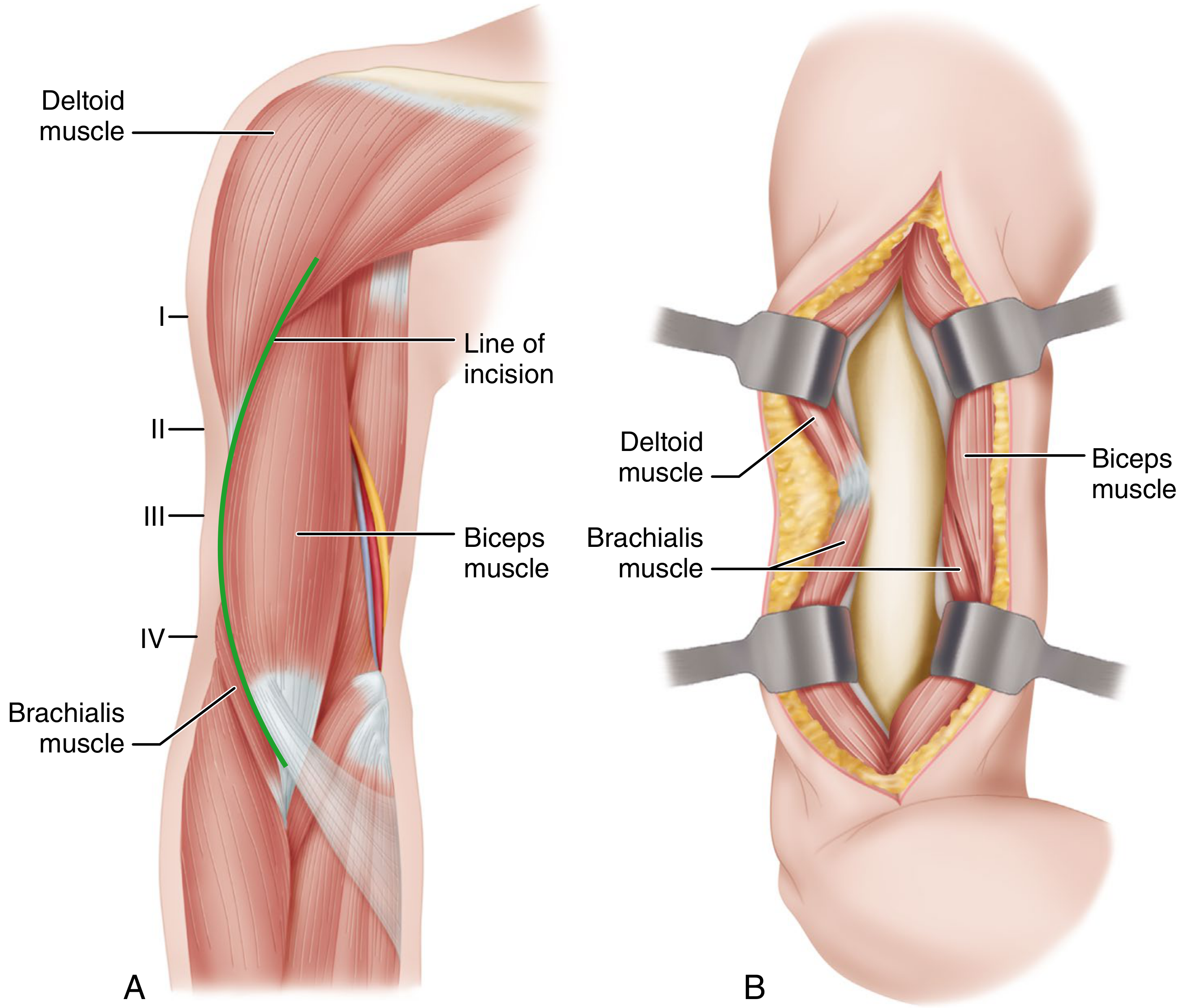
Skin Incision (Thompson-Henry)
The incision runs from the coracoid process proximally, continuing distally along the deltopectoral groove to the level of the deltoid tuberosity, then curves to follow the lateral border of the biceps down to approximately 5 cm proximal to the elbow flexion crease.
A slight apex-lateral curve may be used as preferred.
Step 1 - Superficial Fascia and Cephalic Vein
Incise the superficial and deep fascia. The cephalic vein is identified running in the deltopectoral groove and must be mobilized or ligated.
Step 2 - Proximal Exposure (Deltopectoral Interval)
Develop the interval between:
- Deltoid - retract laterally
- Pectoralis major / biceps long head - retract medially
The anterior circumflex humeral artery will be encountered during deep proximal dissection and should be kept intact if possible, or ligated if necessary.
Caution: Avoid excessive lateral retraction of the deltoid - the axillary nerve enters the deltoid from its deep surface and is at risk from forceful retraction.
Step 3 - Pectoralis Major Attachment (if needed)
Partial detachment of the pectoralis major tendon from the lateral lip of the bicipital groove may be performed to improve proximal exposure of the shaft.
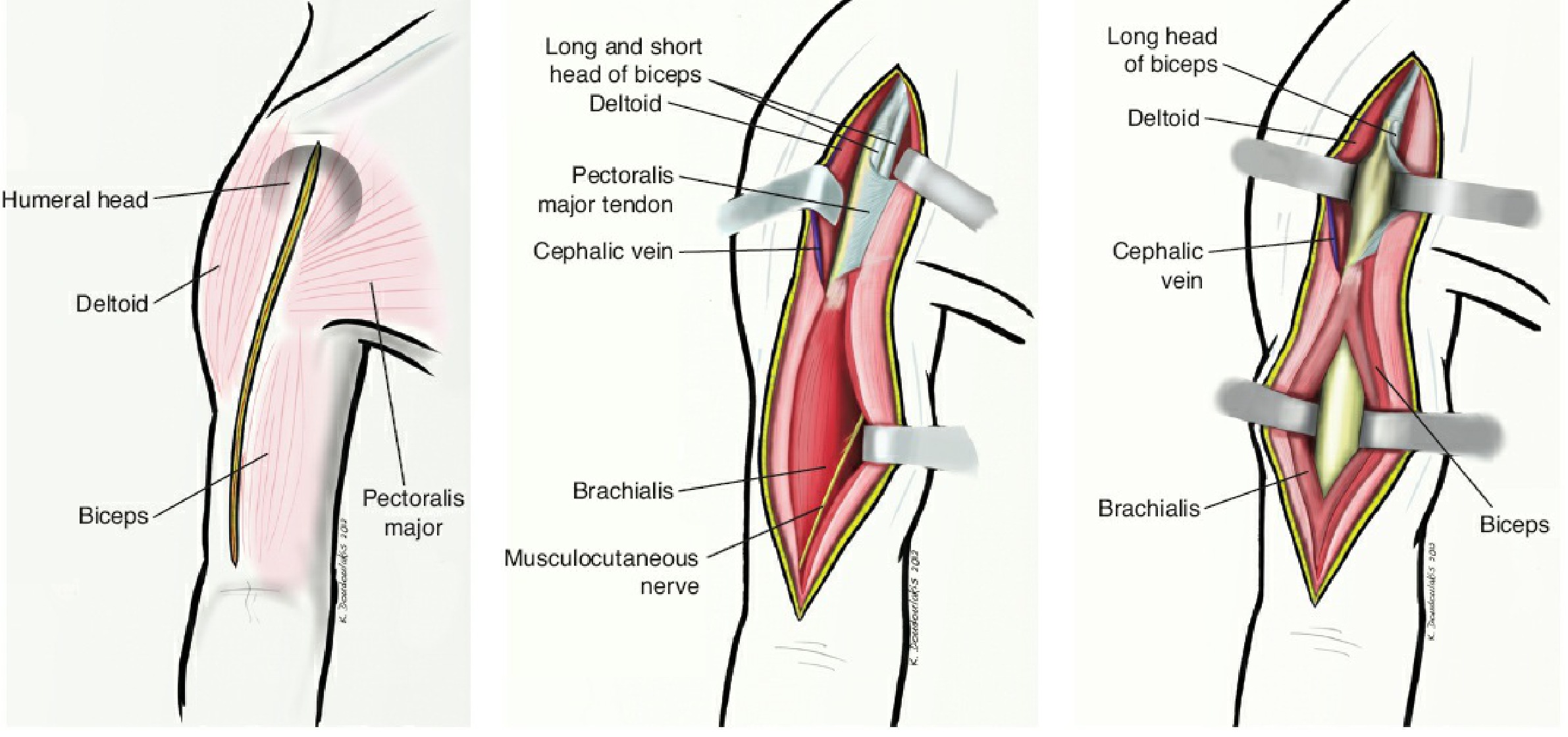
Step 4 - Middle Third Exposure (Brachialis Split)
Distal to the deltoid insertion:
- Mobilize the biceps medially
- This exposes the brachialis muscle, which covers the anterior humeral diaphysis
- Split the brachialis longitudinally at its lateral third (one-third lateral, two-thirds medial)
- Retract the brachialis subperiosteally to expose the shaft
Why split at the lateral third? The brachialis is supplied by the musculocutaneous nerve medially and the radial nerve laterally. A midline or lateral-third split preserves the innervation to both halves. The lateral half of the brachialis also acts as a protective buffer for the radial nerve as it winds around the spiral groove.Retraction is easiest when the elbow is flexed to 90°, which relaxes the brachialis tendon.
Step 5 - Distal Exposure
As the approach extends distally toward the elbow, continue between:
- Brachialis (medially)
- Brachioradialis (laterally)
At the distal end, be vigilant for:
- Radial nerve traveling deep to the brachioradialis muscle
- Lateral antebrachial cutaneous nerve (terminal branch of musculocutaneous) coursing medially to laterally under the biceps tendon as it enters the field
Step 6 - Periosteal Elevation
Incise the periosteum over the anterolateral surface and elevate it as needed to expose the humeral shaft for plate placement.
Access Provided
| Region | Accessible? |
|---|---|
| Humeral head / surgical neck | Yes (proximal extension) |
| Proximal third of shaft | Yes (excellent) |
| Middle third of shaft | Yes (excellent) |
| Distal third of shaft | Yes (to within 5 cm of condyles) |
| Coronoid fossa | Yes |
| Distal forearm (combined) | Yes - extend as volar Henry approach |
Structures at Risk
| Structure | Location at Risk | Prevention |
|---|---|---|
| Axillary nerve | Enters deltoid from deep surface; proximal retraction | Avoid excessive lateral retraction of deltoid |
| Radial nerve | Winds in spiral groove; lies under lateral brachialis | Lateral half of brachialis protects it; identify if plating near coronoid fossa |
| Musculocutaneous nerve | Runs with brachialis medially | Preserved by splitting brachialis at its lateral third |
| Anterior circumflex humeral artery | Encountered in proximal deep dissection | Preserve or ligate carefully |
| Cephalic vein | Runs in deltopectoral groove | Mobilize or ligate |
| Lower lateral brachial cutaneous nerve | Subcutaneous, crosses the incision line distally | King & Johnston modification uses a more anterior incision to avoid this nerve - the original Henry incision transects it in ~62% of cases, causing painful neuromata |
| Lateral antebrachial cutaneous nerve | Exits lateral to biceps tendon at elbow | Protect during distal dissection |
Advantages
- Truly extensile - from humeral head to coronoid fossa, and further into forearm
- Lowest incidence of radial nerve palsy among humeral shaft approaches (the lateral brachialis half provides a physical nerve shield)
- Intermuscular at most levels; brachialis dual innervation allows safe longitudinal splitting
- Can be performed supine (patient comfort, ease of anaesthesia)
- Most appropriate for proximal two-thirds of humeral shaft
Disadvantages
- Not the best approach for distal third fractures - posterior approach is preferred there
- Radial nerve still at risk with excessive dissection or screw penetration near spiral groove
- King & Johnston modification required to avoid painful neuromata from lower lateral brachial cutaneous nerve
Modifications
| Modification | Description |
|---|---|
| King & Johnston modification | More anteriorly placed incision (watershed zone between medial and brachial cutaneous nerve territories) - reduces painful neuromata |
| Alternative distal plane | Between biceps + brachialis medially and brachioradialis laterally at the junction of middle and distal thirds - but not extensile enough alone |
| Proximal extension | Extends into anteromedial shoulder approach (deltopectoral) |
| Distal extension | Continues as volar Henry approach into forearm |
Comparison: Anterolateral vs. Posterior Approach
| Feature | Anterolateral | Posterior (Triceps-Splitting) |
|---|---|---|
| Best level | Proximal 2/3 of shaft | Middle 1/3 to distal 1/3 |
| Position | Supine | Prone or lateral |
| Radial nerve palsy risk | Lowest | Moderate |
| Internervous plane | Partial (brachialis dual innervation) | None (all radial nerve) |
| Postop restriction | None specific | Triceps repair protection |
| Conversion to TEA | Not directly | Yes - easy |
(Sources: Campbell's Operative Orthopaedics 15th ed. 2026; Rockwood & Green's Fractures in Adults 10th ed. 2025; Miller's Review of Orthopaedics 9th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.