Leutal phase timing
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough breakdown of luteal phase timing drawn from multiple authoritative physiology and clinical textbooks.
Luteal Phase - Timing and Key Events
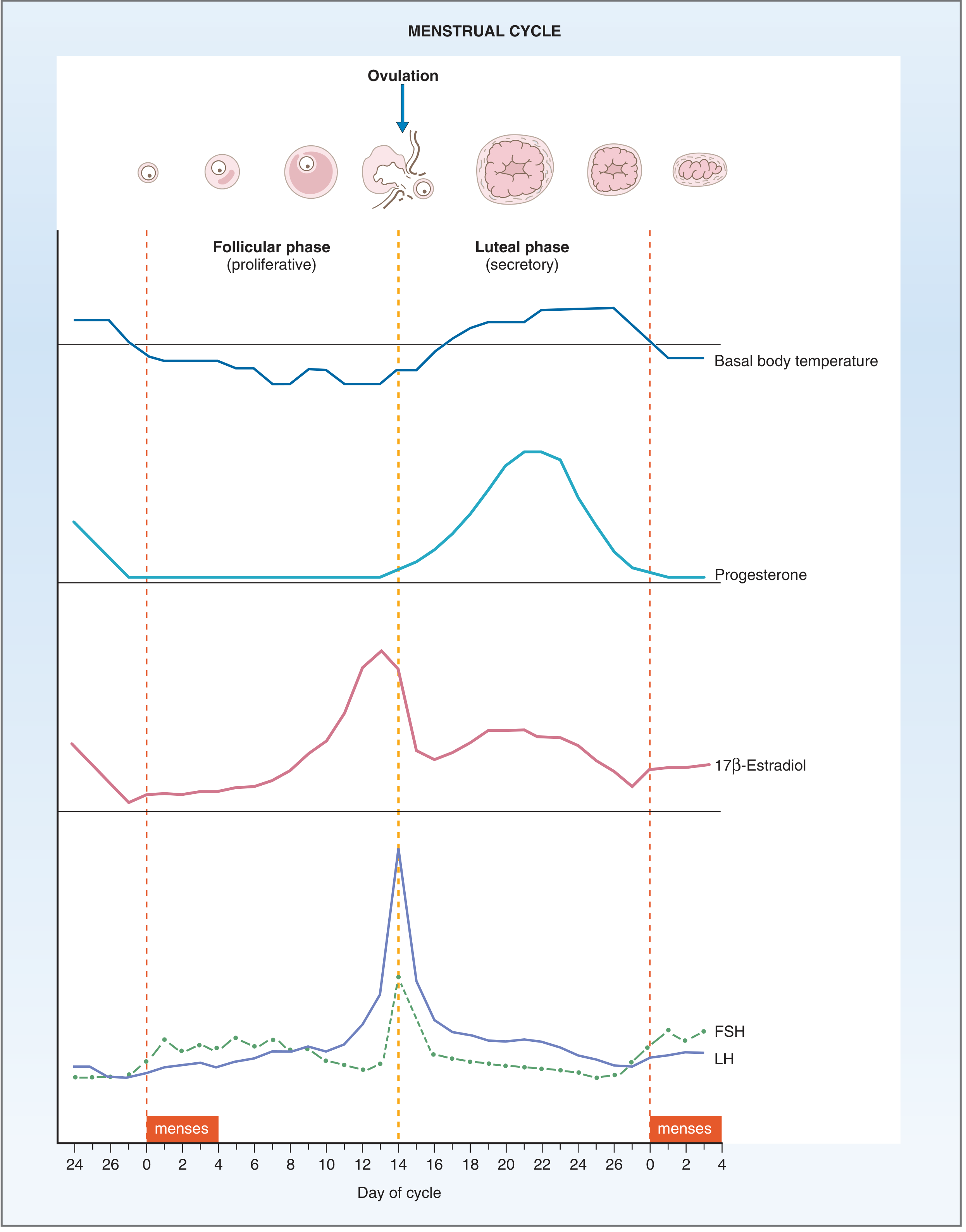
Menstrual cycle hormone profiles - Costanzo Physiology, 7th Ed., Fig. 10.10
When Does It Start and End?
| Marker | Timing |
|---|---|
| Start | Day 14 (ovulation) in a 28-day cycle |
| End | Day 28 (onset of next menses) |
| Duration | 12-14 days - relatively fixed |
| Ovulation rule | Always ~14 days BEFORE the next period, regardless of cycle length |
Key point: The follicular phase is variable (accounts for all cycle-length variation), but the luteal phase is remarkably constant at 12-14 days. - Harrison's Principles of Internal Medicine, 22nd Ed.
What Happens During the Luteal Phase
Corpus luteum formation (days 14-21)
- The ruptured follicle transforms via luteinization: granulosa and theca interna cells enlarge, fill with lipid inclusions, and gain a yellowish appearance
- The corpus luteum grows to ~1.5 cm diameter, peaking 7-8 days after ovulation (around day 21-22)
- Granulosa-lutein cells produce large amounts of progesterone (dominant hormone) and estradiol
- Theca-lutein cells supply androgen precursors, which are aromatized into estradiol
Hormone timeline within the luteal phase
- Progesterone: rises modestly just before ovulation, spikes sharply after, peaks ~day 21, then drops
- Estradiol: dips just after ovulation, then rises again from corpus luteum production mid-luteal phase, falls before menses
- FSH and LH: both suppressed by negative feedback from progesterone and estrogen; lutein cells also secrete inhibin (suppresses FSH further)
Endometrial effects
- Progesterone converts the proliferative endometrium into a secretory endometrium - increasing vascularity and glandular secretion, preparing for implantation
- Basal body temperature rises ~0.24°C (>0.5°F) due to the thermogenic action of progesterone on the hypothalamic set point - this is detectable clinically
Corpus luteum involution (days 22-28)
- Without hCG (no pregnancy), the corpus luteum begins degenerating ~day 22-23, completing by ~day 26
- Progesterone and estradiol fall abruptly
- The endometrium loses hormonal support leading to ischemia, cytokine release, and shedding (menses)
- The corpus luteum becomes the corpus albicans (fibrotic scar), absorbed over months
If Pregnancy Occurs
- Trophoblast-produced hCG binds LH receptors on the corpus luteum, rescuing it from involution
- The corpus luteum is maintained for the first 6-10 weeks of gestation (luteal-placental shift), at which point the placenta takes over steroidogenesis
- This is why early pregnancy tests detect hCG and why early miscarriage can follow luteal failure
Luteal Phase Defect (LPD)
A shortened or inadequate luteal phase is clinically defined by:
- Serum progesterone level below normal in the mid-luteal phase (~day 21)
- Basal body temperature elevation lasting less than 11 days
- Shortened luteal phase on charting
LPD is associated with implantation failure, early pregnancy loss, and subfertility.
Clinical Assessment of Ovulation Timing
| Method | Details |
|---|---|
| Serum progesterone | >3 ng/mL drawn ~7 days after ovulation (mid-luteal, ~day 21) confirms ovulation |
| Basal body temperature | Rise of >0.5°F marks onset of luteal phase |
| Urinary LH surge | Ovulation occurs ~36 hours after the surge (can time intercourse) |
| Ultrasound | Follicle collapse + corpus luteum formation confirms ovulation |
Sources:
- Costanzo Physiology, 7th Ed., pp. 479-481
- Guyton and Hall Medical Physiology, pp. 1018-1019
- Medical Physiology (Boron & Boulpaep), pp. 2576-2582
- Harrison's Principles of Internal Medicine, 22nd Ed., pp. 3172-3173
This is a shared conversation. Sign in to Orris to start your own chat.