Post menopausal bleeding diagnosis and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"postmenopausal bleeding" AND diagnosis AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
postmenopausal bleeding evaluation algorithm transvaginal ultrasound endometrial biopsy
I now have comprehensive information. Let me compile the full answer.
Postmenopausal Bleeding: Diagnosis and Management
Definition
Postmenopausal bleeding (PMB) is any vaginal bleeding occurring ≥12 months after the last menstrual period. Even minimal spotting or brownish discharge must be fully evaluated — it should never be dismissed. PMB is distinct from abnormal uterine bleeding in reproductive-age women and sits outside the PALM-COEIN classification system.
Etiology & Differential Diagnosis
| Cause | Approximate Frequency |
|---|---|
| Endometrial atrophy | 60–80% (most common overall) |
| Exogenous estrogens / HRT | ~30% |
| Atrophic vaginitis | Up to 15% |
| Endometrial cancer | 10–15% |
| Endometrial or cervical polyps | 2–12% |
| Endometrial hyperplasia | 5–10% |
| Miscellaneous (cervical cancer, uterine sarcoma, urethral caruncle, trauma, coagulation disorders) | ~10% |
Key statistic: ~10% of women with PMB will have a malignancy (endometrial or cervical). Conversely, 90% of women with endometrial cancer present with PMB.
Important Points on Cause
- Endometrial atrophy is the single most common finding — women are typically menopausal for ~10 years; biopsy often yields scant or insufficient tissue
- Tamoxifen use is associated with endometrial polyps and increases malignancy risk; these polyps may not be detected by office biopsy alone
- Uterine leiomyomas should never be accepted as the cause of PMB — a malignant source must be excluded first
- Functional ovarian tumors secreting estrogen can cause endometrial hyperplasia/carcinoma
- Non-genital sources (hematuria, rectal bleeding) must always be excluded by history and exam
Risk Factors for Endometrial Cancer
- Obesity (excess peripheral estrogen conversion)
- Unopposed exogenous estrogen use
- Tamoxifen use
- Diabetes mellitus, hypertension
- Nulliparity, late menopause
- Hereditary syndromes (Lynch syndrome / HNPCC)
- Estrogen-secreting ovarian tumor
Diagnostic Approach
Step 1 — History & Physical Examination
- Characterize bleeding (duration, amount, associated symptoms)
- Medication history — HRT type/regimen, tamoxifen, anticoagulants
- Pelvic examination: inspect vulva, vagina (atrophic changes, lesions), cervix
- Any grossly visible cervical lesion → cervical biopsy directly
- Assess for uterine size, adnexal masses
Step 2 — First-Line Investigations (run in parallel)
| Test | Purpose |
|---|---|
| Cervical cytology (Pap smear) | Screen for cervical pathology (note: insensitive for endometrial cancer; may be negative even in invasive cervical cancer due to necrosis) |
| Transvaginal ultrasound (TVUS) | Measure endometrial thickness; identify focal lesions, polyps |
| Endometrial biopsy (EMB) | Histological diagnosis — first-line tissue sampling |
| CBC, TSH, coagulation studies | If clinically indicated |
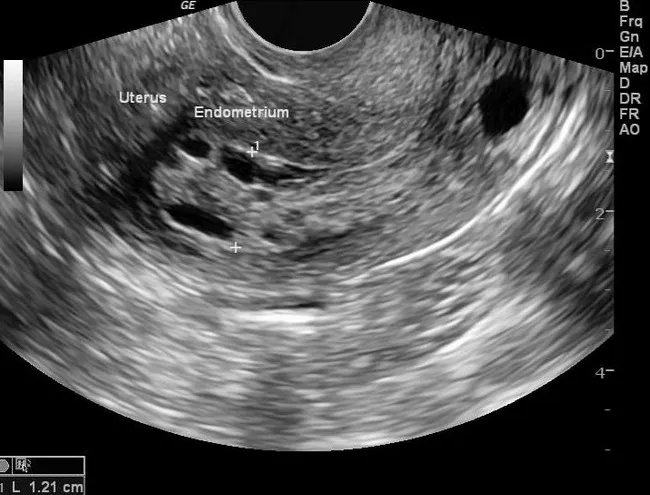
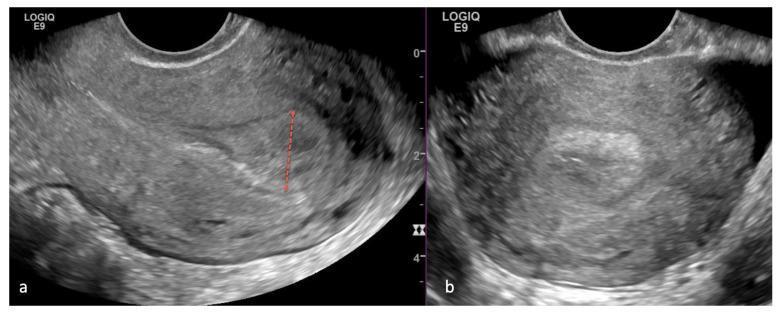
Step 3 — Interpreting Endometrial Thickness on TVUS
The 4–5 mm threshold is the core decision point:
| Endometrial Thickness | Interpretation | Action |
|---|---|---|
| ≤ 4 mm | Low risk of malignancy | Biopsy can be deferred if no high-risk features; monitor |
| > 4 mm | Requires tissue sampling | Proceed to endometrial biopsy |
| Any thickness with persistent bleeding | Cannot exclude cancer | Endometrial biopsy regardless of thickness |
Important caveat (equity issue): Recent data show the ≤4 mm cutoff has led to underdiagnosis of endometrial cancer in Black patients. Clinical judgment and low threshold for biopsy should apply regardless of ultrasound findings in high-risk populations. — Sabiston Textbook of Surgery
Here are representative TVUS images showing endometrial thickening in PMB:
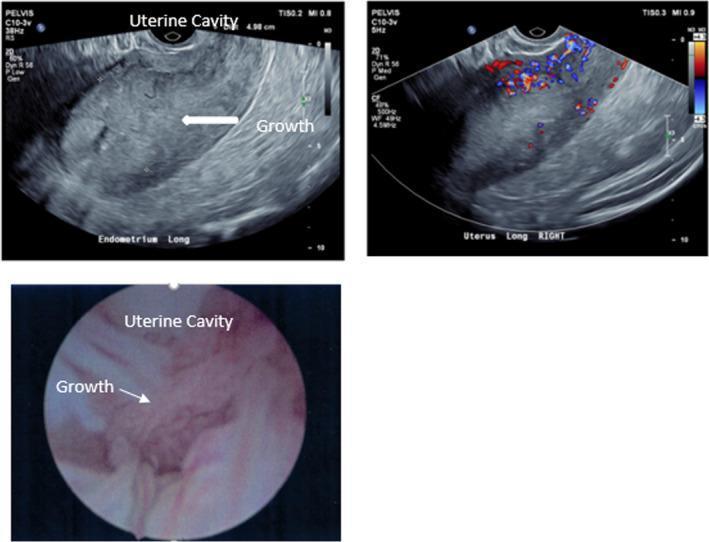
Step 4 — Tissue Sampling Methods
| Method | When to Use |
|---|---|
| Office endometrial biopsy (Pipelle/similar) | First-line; adequate in most cases |
| Sonohysterography (saline infusion) | Better characterization of focal lesions |
| Hysteroscopy + directed biopsy | Preferred when polyps suspected; biopsy may miss focal lesions; definitive for polypoid pathology |
| D&C (dilatation and curettage) | When office biopsy fails (cervical stenosis), insufficient tissue, or persistent bleeding with negative initial workup |
Endometrial polyps are often missed by office biopsy; hysteroscopy is the gold standard for their detection and removal.
Management
1. Atrophic Vaginitis / Endometrial Atrophy
- Topical (vaginal) estrogens: creams, tablets, or rings — systemic absorption is minimal compared to oral routes
- Systemic HRT if broader menopausal symptoms warrant it
- Treat after excluding malignancy
2. HRT-Related Bleeding
- Continuous combined regimen: irregular bleeding for first few months is expected; resolves in most women after 6 months — endometrial cancer risk is low
- Significant change in withdrawal bleeding or breakthrough bleeding → endometrial sampling indicated
- Missed doses of oral HRT can cause spotting; consider non-oral routes for better compliance
- Unopposed estrogen → endometrial hyperplasia risk ×4–8; always add progestogen in women with a uterus
3. Cervical/Endometrial Polyps
- Cervical polyps: easily removed in office
- Endometrial polyps: hysteroscopic polypectomy — up to 5% undergo malignant transformation; risk higher with tamoxifen use, obesity, and age
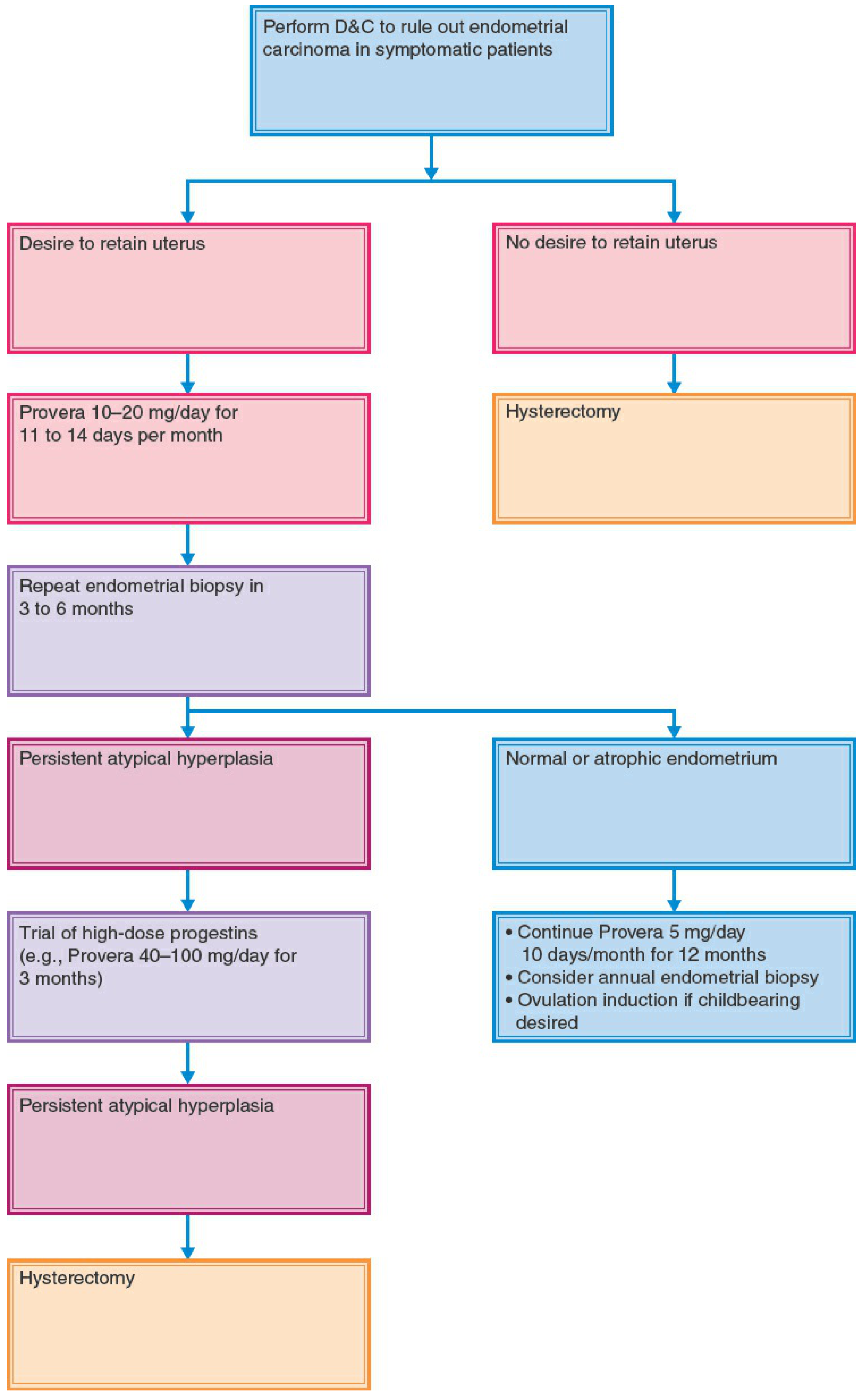
4. Endometrial Hyperplasia (2015 ACOG/SGO EIN Nomenclature)
| Class | Pathology | Treatment |
|---|---|---|
| Benign | Benign endometrial hyperplasia | Medical: progestins (oral, Mirena IUS) |
| Premalignant | EIN (replaces "atypical hyperplasia") | Surgical (hysterectomy) preferred; medical (progestins) if fertility desired or poor surgical candidate |
| Malignant | Endometrioid adenocarcinoma, well-differentiated | Surgical staging ± adjuvant therapy |
Progestin therapy monitoring: endometrial biopsy every 3 months; recurrence risk approaches 50% with conservative medical management of EIN.
5. Endometrial Cancer
- Requires surgical staging: total hysterectomy + bilateral salpingo-oophorectomy + pelvic/para-aortic lymph node assessment
- Multidisciplinary planning for adjuvant radiotherapy/chemotherapy based on stage and grade
- Even with a normal endometrial stripe on TVUS, endometrial sampling should be performed for persistent PMB
- Poor surgical candidates: progestin therapy (oral/parenteral/IUS) with close surveillance
Special Circumstances
| Situation | Action |
|---|---|
| On HRT, no bleeding for several months → resumes | Endometrial sampling |
| PMB with normal TVUS (≤4 mm) but persistent bleeding | EMB still required |
| Negative biopsy but bleeding continues | Hysteroscopy + D&C |
| Pyometra or hematometra (especially older women) | Investigate for cervical stenosis concealing endometrial cancer — often poor prognosis |
| Tamoxifen user | Low threshold for hysteroscopy; polyps more common and may be malignant |
Summary Algorithm
PMB
└→ Full history + pelvic exam + Pap smear
└→ Visible cervical lesion? → Biopsy directly
└→ No lesion → TVUS
├→ Endometrial thickness ≤ 4 mm
│ ├→ No risk factors + bleeding stopped → Monitor
│ └→ Persistent bleeding / high risk → EMB anyway
└→ Endometrial thickness > 4 mm
└→ Endometrial biopsy (office)
├→ Adequate tissue → Histopathology → Treat per result
└→ Inadequate / persistent bleeding → Hysteroscopy ± D&C
Sources:
- Berek & Novak's Gynecology, pp. 479–484
- Sabiston Textbook of Surgery, 20th ed., pp. 2794–2795
- Berek & Novak's Gynecology, pp. 2150–2151 (Endometrial Carcinoma chapter)
Adenomyosis
Finding Sources
Finding Sources
Searching PubMed
"adenomyosis"[MeSH Terms] AND diagnosis AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
adenomyosis histology endometrial glands stroma myometrium microscopy
Reading Article
PMID: 39032312
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.