If you were a student and the examiner asked you about Anterior compartment of Thigh how would you answer to score full marks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I have all the key information and images from Gray's Anatomy for Students and the THIEME Atlas. Here is the full-marks exam answer:
Anterior Compartment of the Thigh
Sources: Gray's Anatomy for Students; THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
1. Introduction / Overview
The anterior compartment of the thigh is bounded by the fascia lata (deep fascia of the thigh) and its lateral intermuscular septum. It contains the primary extensors of the knee and flexors of the hip, is innervated entirely by the femoral nerve (L2-L4), and is supplied by branches of the femoral artery. The compartment is best understood by covering its muscles, the femoral triangle, the adductor canal, its neurovascular supply, and clinical applications.
2. Fascial Covering - Fascia Lata
The deep fascia of the thigh (fascia lata) encloses the entire thigh and sends intermuscular septa between the three compartments (anterior, medial, posterior). On its anteromedial surface, just below the medial end of the inguinal ligament, lies the saphenous opening - an aperture that allows the great saphenous vein to pierce through to join the femoral vein. The margin is formed by the free medial edge of the fascia lata spiralling around the great saphenous vein.
3. Muscles of the Anterior Compartment
There are two groups:
3.1 Sartorius
| Feature | Detail |
|---|---|
| Origin | Anterior superior iliac spine (ASIS) |
| Insertion | Medial surface of the tibia (with gracilis and semitendinosus - forms pes anserinus) |
| Action (hip) | Flexion, abduction, lateral rotation |
| Action (knee) | Flexion, medial rotation |
| Nerve | Femoral nerve (L2-L4) |
The sartorius is the longest muscle in the body. It runs obliquely across the thigh from ASIS to the medial knee, forming the lateral boundary of the femoral triangle. Note: although classified in the anterior compartment, at the knee it migrates posterior to the joint axis and thus acts as a knee flexor.
3.2 Quadriceps Femoris
The quadriceps is a four-headed muscle - the only significant extensor of the knee. All four heads converge on the patella via the quadriceps tendon, which continues as the patellar ligament inserting into the tibial tuberosity. All parts are innervated by the femoral nerve (L2-L4).
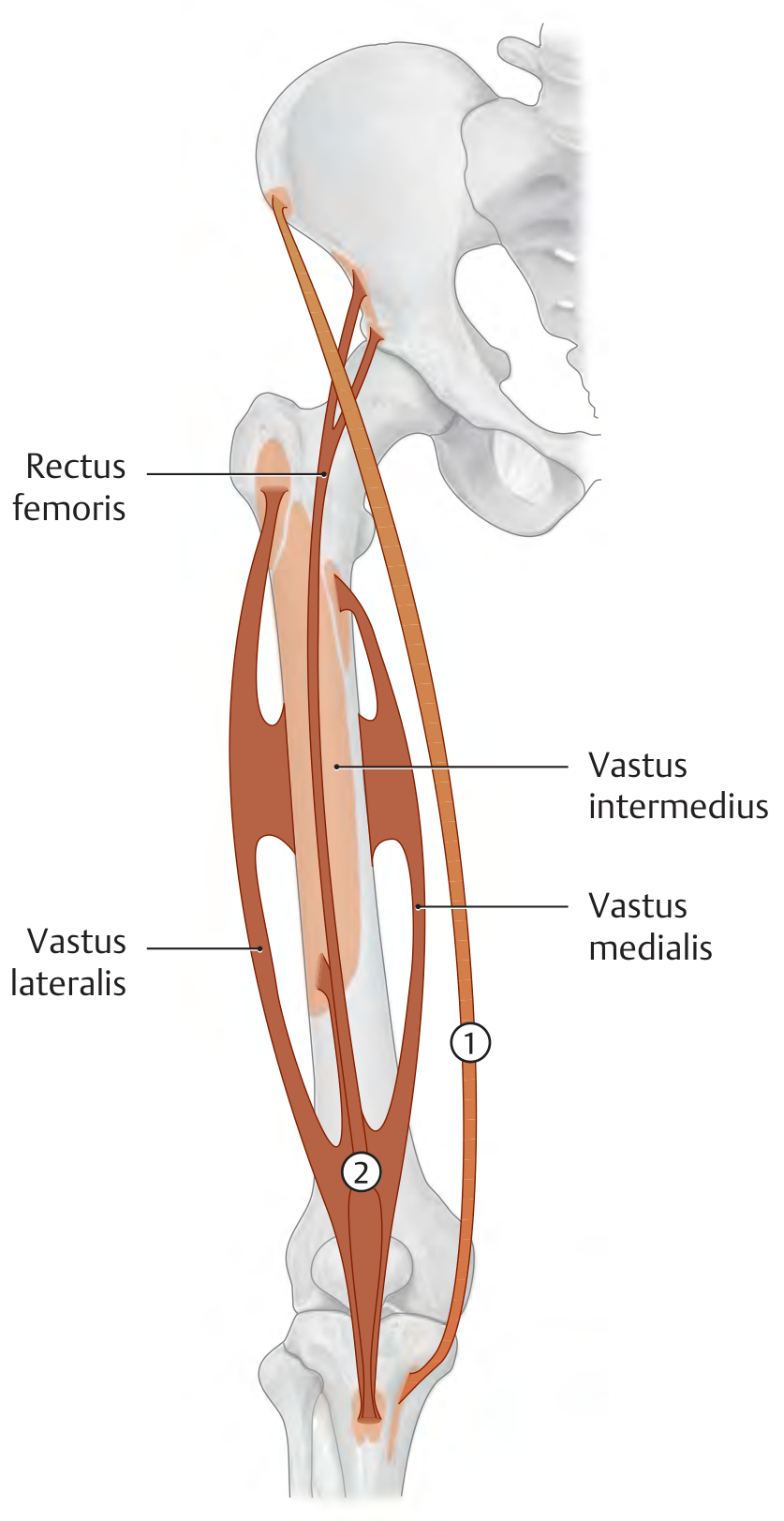
| Head | Origin | Special notes |
|---|---|---|
| Rectus femoris | Straight head: AIIS; Reflected head: roof of acetabulum | Only part that crosses the hip; also flexes the hip |
| Vastus lateralis | Lateral lip of linea aspera; lateral surface of greater trochanter | Largest of the four heads |
| Vastus medialis | Medial lip of linea aspera; distal part of intertrochanteric line | Lowest fibres (VMO) prevent lateral patellar dislocation |
| Vastus intermedius | Anterior surface of femoral shaft | Deep to rectus femoris |
| Articularis genus | Distal fibres of vastus intermedius; anterior femoral shaft | Pulls suprapatellar recess upward during extension - prevents capsule impingement |
Action: Knee extension (all parts); hip flexion (rectus femoris only).
Insertion: All via the patellar ligament to the tibial tuberosity; vastus medialis and lateralis also attach to tibial condyles via the medial and lateral patellar retinacula.
4. The Femoral Triangle
The femoral triangle is a wedge-shaped depression in the upper anterior thigh at the junction of the lower limb and anterior abdominal wall.
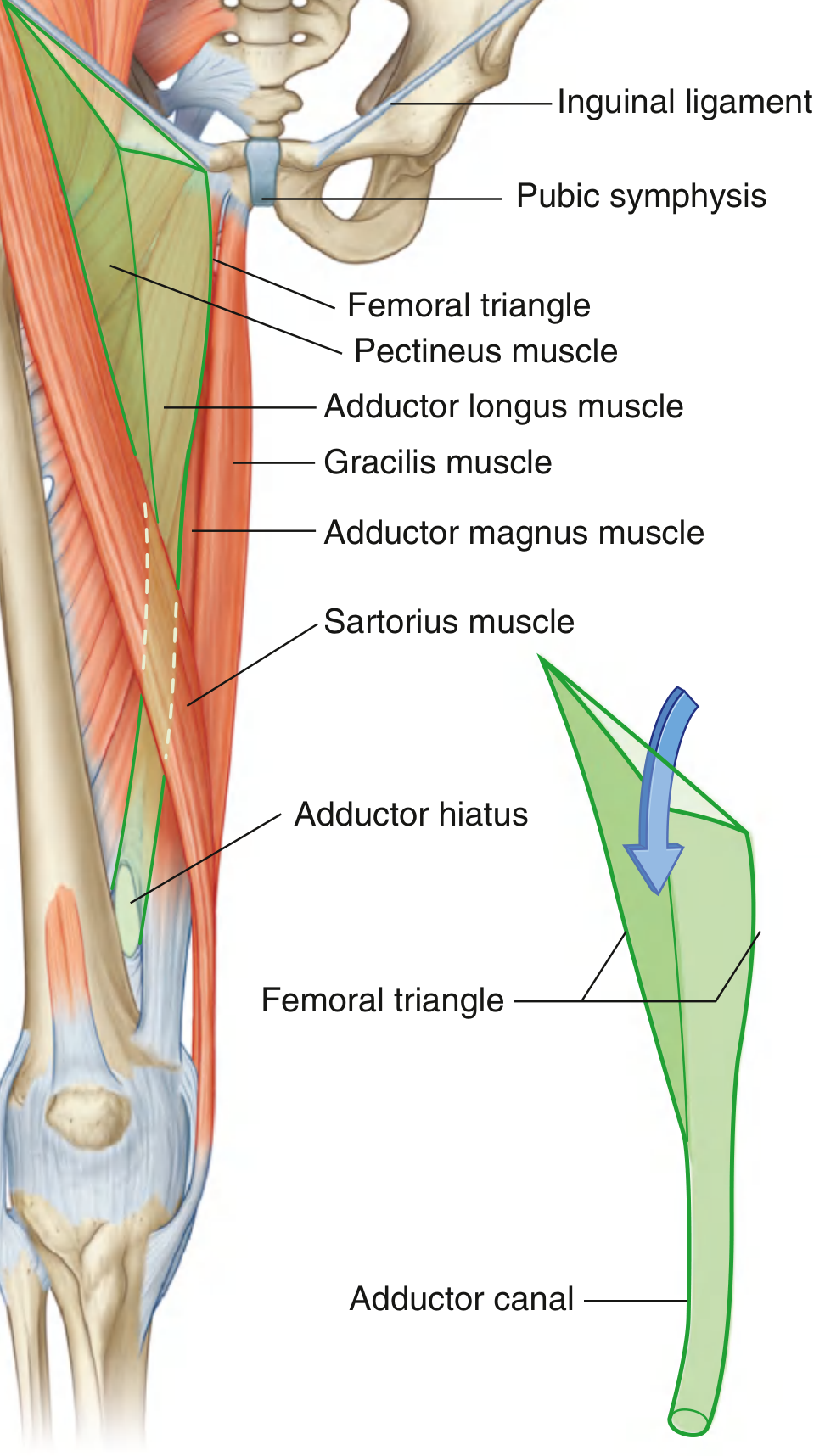
Boundaries
| Boundary | Structure |
|---|---|
| Base (superior) | Inguinal ligament |
| Lateral border | Medial margin of sartorius |
| Medial border | Medial margin of adductor longus |
| Floor (medial part) | Pectineus and adductor longus |
| Floor (lateral part) | Iliopsoas |
| Roof | Fascia lata (with saphenous opening medially) |
| Apex | Points inferiorly, continuous with the adductor canal |
Contents (lateral to medial - mnemonic: NAVY)
From lateral to medial: Nerve (femoral) - Artery (femoral) - Vein (femoral) - Y (lymphatics/empty space/femoral canal)
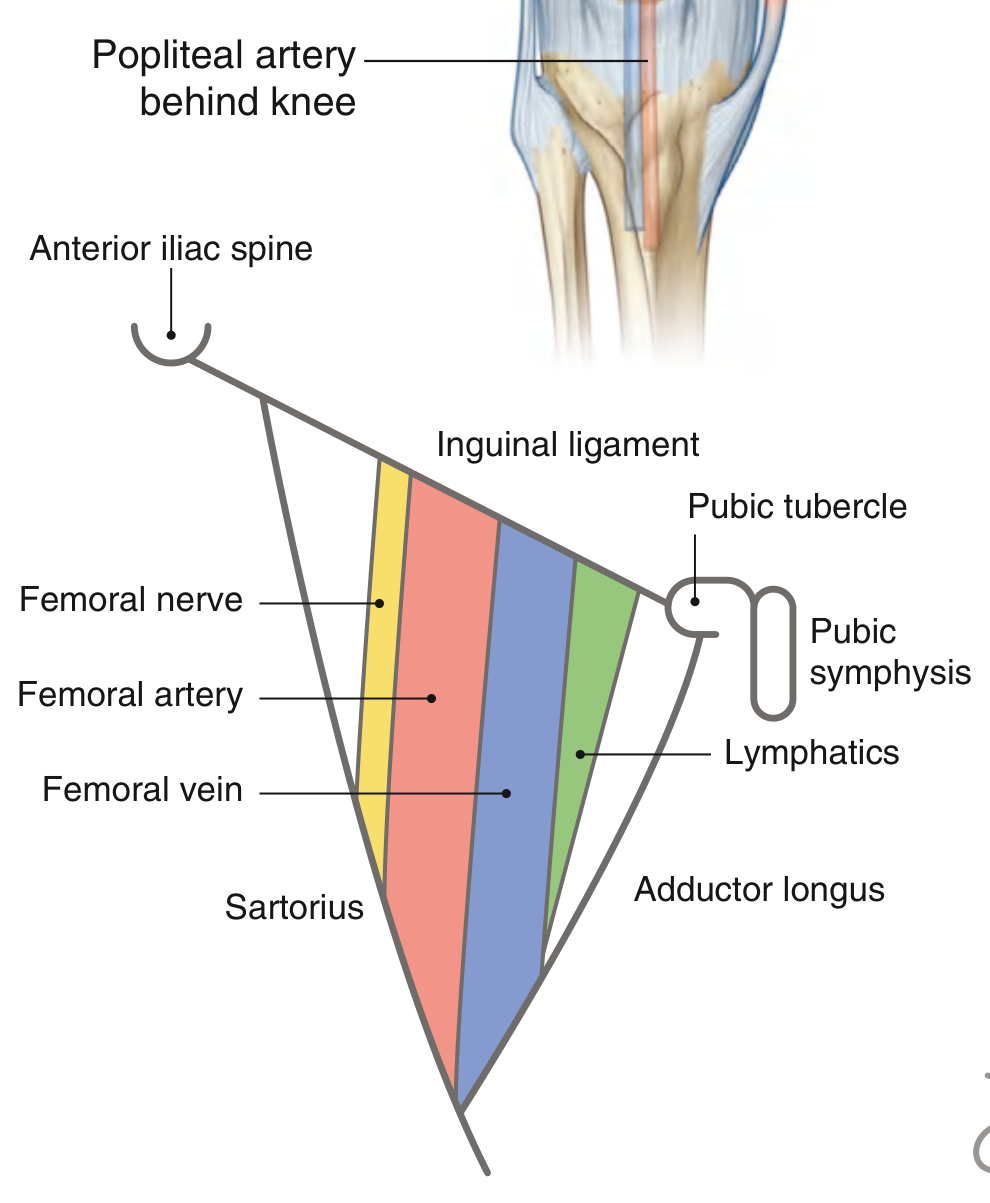
- Femoral nerve (L2-L4): Lateral-most; NOT enclosed in the femoral sheath
- Femoral artery: Palpable midway between ASIS and pubic symphysis, just below the inguinal ligament
- Femoral vein: Medial to the artery
- Lymphatics / femoral canal: Most medial
Femoral Sheath
The femoral artery, vein, and lymphatics (but not the nerve) are enclosed in a funnel-shaped fascial sleeve - the femoral sheath - which is continuous superiorly with the transversalis and iliac fasciae. It has three compartments:
- Lateral - femoral artery
- Middle - femoral vein
- Medial - femoral canal (lymphatics + fat + Rosenmüller/Cloquet lymph node)
The femoral canal is the most medial compartment; its superior opening (the femoral ring) is a potential weak point and is the site of femoral hernias. It is bounded by: inguinal ligament (anteriorly), femoral vein (laterally), lacunar ligament (medially), and pectineal ligament/pectineus (posteriorly).
5. The Adductor Canal (Subsartorial / Hunter's Canal)
The adductor canal continues from the apex of the femoral triangle and conducts the femoral vessels through the medial thigh to the adductor hiatus, where they become the popliteal vessels.
Boundaries
| Wall | Structure |
|---|---|
| Anterior (roof) | Vastoadductor membrane (sartorius overlying it) |
| Posterior | Adductor longus and adductor magnus |
| Lateral | Vastus medialis |
Contents
- Femoral artery
- Femoral vein
- Saphenous nerve (branch of femoral nerve) - exits by piercing the vastoadductor membrane along with the descending genicular artery, then passes to the medial side of the knee
- Nerve to vastus medialis
Key point: At the adductor hiatus (a gap in the adductor magnus tendon), the femoral artery and vein exit posteriorly to become the popliteal artery and vein. The saphenous nerve does NOT pass through the hiatus - it continues subcutaneously to the medial leg and foot.
6. Neurovascular Supply
Femoral Nerve (L2-L4)
- Formed in the lumbar plexus from posterior divisions of L2, L3, L4
- Passes under the inguinal ligament through the muscular compartment (lateral to the iliopectineal arch), lateral to the femoral artery
- In the femoral triangle it divides into multiple branches almost immediately
- Motor: All anterior compartment muscles + iliacus + pectineus (in the abdomen before entering the thigh)
- Sensory: Anterior thigh (anterior cutaneous branches), anteromedial knee, medial leg and medial foot (via the saphenous nerve - the only branch to descend below the knee)
Femoral Artery
- Direct continuation of the external iliac artery below the inguinal ligament
- Runs through the femoral triangle and adductor canal, exits at the adductor hiatus to become the popliteal artery
- Major branch: Profunda femoris (deep femoral artery) - arises ~4 cm below the inguinal ligament; gives rise to:
- Medial circumflex femoral artery (main supply to femoral head)
- Lateral circumflex femoral artery (anterior thigh muscles; ascending branch anastomoses with gluteal arteries)
- 1st-3rd perforating arteries (pierce adductor muscles to supply posterior thigh/hamstrings)
- Descending genicular artery (from the femoral artery in the canal, pierces the vastoadductor membrane with the saphenous nerve)
7. Applied Anatomy / Clinical Points
-
Femoral hernia: Protrudes through the femoral ring (medial compartment of the femoral sheath) - more common in females due to wider pelvis. The sharp lacunar ligament makes it prone to strangulation.
-
Femoral artery access: The femoral pulse is palpable at the midpoint of the inguinal ligament (midinguinal point). Used for arterial catheterisation in coronary angiography, peripheral angiography, cardiac catheterisation, and emergency vascular access.
-
Quadriceps weakness / paralysis: Loss of femoral nerve function causes inability to extend the knee. Walking on flat surfaces may still be possible by locking the knee hyperextended (line of gravity passing anterior to the knee axis), but stairs and rising from a chair are severely impaired.
-
Adductor canal block (Hunter's canal block): Regional anaesthesia technique targeting the saphenous nerve and nerve to vastus medialis for analgesia after knee surgery (e.g. total knee replacement) with minimal quadriceps weakness - preferred over femoral nerve block for faster rehabilitation.
-
Saphenous nerve injury: During harvesting of the great saphenous vein (for coronary bypass grafts), the saphenous nerve running alongside the vein can be damaged, causing medial leg and medial foot sensory loss.
-
Quadriceps tendon / patellar ligament rupture: The quadriceps insertion can rupture (quadriceps tendon, proximal to patella) or the continuation can rupture (patellar ligament, distal to patella). Both present with inability to extend the knee and a palpable gap.
Summary Table
| Feature | Detail |
|---|---|
| Nerve supply | Femoral nerve (L2-L4) |
| Artery | Femoral artery + profunda femoris branches |
| Muscles | Sartorius; Quadriceps (rectus femoris, vastus lateralis, vastus medialis, vastus intermedius, articularis genus) |
| Main action | Knee extension; hip flexion |
| Key space (proximal) | Femoral triangle |
| Key space (distal) | Adductor canal |
| Clinical imp. | Femoral hernia, vascular access, quadriceps paralysis, adductor canal block |
References: Gray's Anatomy for Students (Elsevier); THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.