Nepphrolithiasis
Reading File
Finding Sources
Searching PubMed
"nephrolithiasis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-structured response. Let me compile the full answer.
Nephrolithiasis (Kidney Stones / Urolithiasis)
Epidemiology
Urolithiasis affects 5-12% of the world population over a lifetime. Males are affected about twice as often as females, with peak onset between ages 20 and 30. Up to 50% of patients experience a recurrence within 5 years. Geographic, ethnic, dietary, and genetic factors all influence incidence. - Rosen's Emergency Medicine, p. 1396; Robbins Pathologic Basis of Disease
Types of Stones and Pathogenesis
The fundamental mechanism for all stone types is supersaturation of the urine with a stone-forming substance. A low urine volume is the most universal predisposing factor.
| Stone Type | % of All Stones | Key Conditions / Promoters |
|---|---|---|
| Calcium oxalate (± calcium phosphate) | ~70% | Hypercalciuria, hyperoxaluria, hypocitraturia, hyperuricosuria |
| Struvite (magnesium ammonium phosphate) | 5-15% | UTI with urea-splitting organisms |
| Uric acid | 5-10% | Acidic urine (pH <5.5), gout, hyperuricosuria, leukemia |
| Cystine | 1-2% | Cystinuria (autosomal recessive) |
(Robbins, Table 20.12)
Calcium Stones (Most Common)
- ~5% have hypercalcemia (hyperparathyroidism, sarcoidosis, malignancy)
- ~55% have hypercalciuria without hypercalcemia: absorptive hypercalciuria, renal tubular hypercalciuria, or idiopathic
- ~20% are associated with hyperuricosuria - uric acid crystals nucleate calcium oxalate deposition in the collecting ducts
- ~5% are driven by hyperoxaluria (Crohn disease, small bowel resection, bariatric surgery, radiation enteritis, or rare primary/hereditary oxaluria)
- Hypocitraturia (citrate normally inhibits stone formation) can be idiopathic or due to metabolic acidosis/chronic diarrhea
- Robbins Pathologic Basis of Disease; Rosen's Emergency Medicine
Struvite Stones
- Formed by urea-splitting organisms: Proteus, Providencia, Klebsiella, Pseudomonas, Staphylococcus
- Produce ammonia, raising urinary pH and precipitating MgNH₄PO₄
- Often grow very large - staghorn calculi (75% of staghorn calculi are struvite) that fill much of the renal pelvis
- Common in patients with anatomic abnormalities predisposing to recurrent UTI
- Robbins; Rosen's Emergency Medicine
Uric Acid Stones
- Radiolucent (do not show on plain X-ray) - a classic distinction
- Require persistently acidic urine (pH <5.5) for precipitation
- Associated with gout (~15% of gout patients develop stones), leukemia/rapid cell turnover, uricosuric drugs
- More than 50% of uric acid stone formers have neither hyperuricemia nor hyperuricosuria - urine pH is the primary driver
- Robbins; Rosen's Emergency Medicine
Cystine Stones
- Autosomal recessive defect in renal (and intestinal) reabsorption of dibasic amino acids: Cystine, Ornithine, Lysine, Arginine (mnemonic: COLA)
- Cystine is the least soluble; hexagonal crystals on urine microscopy
- Quick Compendium of Clinical Pathology, 5th Ed.
Urine Crystal Morphology
| Crystal | Shape |
|---|---|
| Calcium oxalate | "Envelopes" |
| Uric acid | Pleomorphic - diamond, square, rod; polarize in multiple colors |
| Struvite | "Coffin lids" (form in alkaline pH) |
| Cystine | Hexagonal |
| Ammonium biurate | "Thorn apples" |
(Quick Compendium of Clinical Pathology, 5th Ed.)
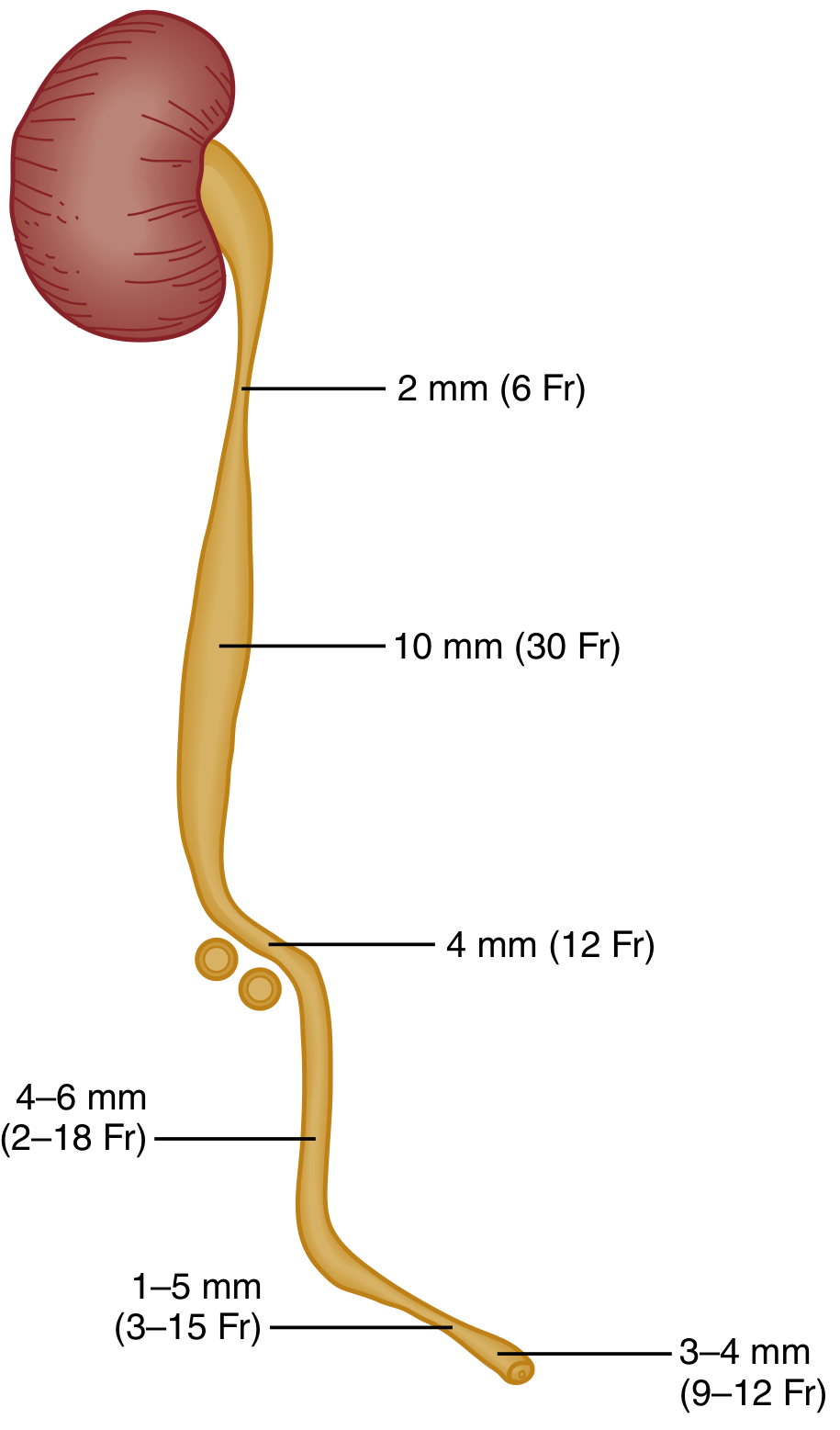
Sites of Impaction
Stones originate in the kidney and migrate. There are five classic sites of impaction along the ureter:
- Calyx / renal pelvis
- Ureteropelvic junction (UPJ) - abrupt narrowing from ~1 cm pelvis to 2-3 mm ureter
- Pelvic brim - where ureter crosses the iliac vessels
- Ureterovesical junction (UVJ) - the most constricted point; most common site of impaction
- Vesical orifice
At diagnosis, up to 75% of stones are in the distal third of the ureter.
Clinical Features
- Renal colic: abrupt onset, crescendo of extreme flank pain radiating laterally around the abdomen and into the groin/labia/testicle
- Hematuria (microscopic or gross) - present in most cases but not universal
- Nausea and vomiting - common
- Pain is typically colicky, not positional (unlike peritonitis)
- Urinary urgency and dysuria with distal ureteral stones
- Fever/chills if there is concomitant infection - this is a urologic emergency
- Rosen's Emergency Medicine
Complications
- Obstruction - causes rapid redistribution of renal blood flow and decreased GFR. Complete obstruction for 1-2 weeks can cause irreversible renal damage
- Infection - obstructed + infected stone = urosepsis risk. Pyelonephritis, perinephric abscess, gram-negative sepsis
- Partial obstruction still risks permanent damage
- Rosen's Emergency Medicine
Diagnosis
Urinalysis
- Hematuria (micro or macro)
- Crystals (see crystal morphology table above)
- Pyuria + bacteriuria suggest concurrent infection
Imaging
Non-contrast CT (NCCT) of abdomen/pelvis is the gold standard outside pregnancy:
- Sensitivity and specificity >90%; detects stones as small as 1 mm
- Identifies hydronephrosis, hydroureter, ureteral edema, and alternative diagnoses (AAA, abscess, malignancy)
- Radiolucent uric acid stones are visible on CT (unlike plain film)
- Low-dose protocols are appropriate for BMI <30 kg/m²
- Patients with known stone history and classic renal colic without fever, infection, solitary kidney, or concern for alternative diagnosis may not need CT
Ultrasound:
- First-line in pregnancy and pediatrics
- Sensitivity ~54%, specificity ~91% for stones; up to 100% sensitive for ureteral obstruction
- Detects hydronephrosis reliably
- Less accurate for stone size and location
Plain X-ray (KUB):
- Detects radiopaque stones (calcium-containing)
- Misses uric acid, cystine, and many small stones
Rosen's Emergency Medicine
Management
Acute Pain Control
- NSAIDs are first-line (ketorolac 30 mg IV or diclofenac 75 mg IM)
- Reduce ureteral spasm and renal capsular pressure by lowering GFR in the obstructed kidney
- Use with caution in renal insufficiency or peptic ulcer disease
- IV opioids (fentanyl 1-2 mcg/kg) are also effective; combination with NSAIDs may reduce ED length of stay
- Antiemetics (ondansetron 4 mg IV) + IV fluids for vomiting
- High-volume IV hydration has NOT been shown to improve stone passage
Medical Expulsive Therapy (MET)
- Alpha-blockers (tamsulosin) facilitate passage of distal ureteral stones by relaxing ureteral smooth muscle
Spontaneous Passage Rates (by stone size)
| Size | Spontaneous Passage Rate |
|---|---|
| <5 mm | ~90% within 4 weeks |
| 5-8 mm | ~15% |
| >8 mm | ~5% (usually requires intervention) |
Rosen's Emergency Medicine
Urologic Emergency Indications
Immediate intervention (ureteral stent or percutaneous nephrostomy) is required for:
- Obstructing stone + infection/sepsis
- Bilateral obstructing stones
- Obstruction of a solitary or transplanted kidney
- Significant renal impairment
Surgical Options
- Extracorporeal shock wave lithotripsy (ESWL)
- Ureteroscopy with laser lithotripsy
- Percutaneous nephrolithotomy (PCNL) - for large/staghorn calculi
- Surgery can generally be outpatient if oral intake is tolerated and pain is controlled
Indications for Admission
- Inability to tolerate oral intake / uncontrolled pain
- High-grade obstruction, large stone unlikely to pass
- Concomitant infection
- Solitary/transplanted kidney obstruction
- Significant renal impairment
Prevention (Recurrence Reduction)
| Stone Type | Prevention Strategy |
|---|---|
| All types | Increase fluid intake (urine output >2 L/day) |
| Calcium oxalate | Thiazide diuretics (reduce hypercalciuria); potassium citrate (raises pH, increases citrate); low-oxalate diet; dietary calcium is NOT restricted (reduces enteric oxalate absorption) |
| Uric acid | Allopurinol; urinary alkalinization (potassium citrate) to pH 6-6.5 |
| Struvite | Eradicate underlying infection; complete stone removal |
| Cystine | High fluid intake; urinary alkalinization; D-penicillamine or tiopronin |
Special Considerations: Pregnancy
- Incidence is similar to non-pregnant women (1 in 188 to 1 in 4600)
- Calcium phosphate stones are most common in pregnancy (vs. calcium oxalate outside pregnancy); this is because pregnancy causes physiologic hypercalciuria balanced by increased citrate and nephrocalcin
- ~64-84% of stones pass spontaneously in pregnancy
- Imaging: ultrasound is first-line; MR urography or limited IVU if needed; CT is reserved for cases where benefits outweigh radiation risk
- Risks: increased rates of preterm labor, pyelonephritis, hypertensive disorders
- Comprehensive Clinical Nephrology, 7th Ed.
Sources: Robbins & Cotran Pathologic Basis of Disease | Rosen's Emergency Medicine | Quick Compendium of Clinical Pathology, 5th Ed. | Comprehensive Clinical Nephrology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.