Bronchial asthama
Reading File
Finding Sources
Finding Sources
Searching PubMed
"asthma"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"asthma" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Bronchial Asthma - A Comprehensive Overview
Definition
Asthma is a chronic inflammatory disease of the airways in which many cells and cellular elements play a role. In susceptible individuals, this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and cough - particularly at night and/or in the early morning. These episodes are associated with widespread but variable airflow limitation that is often reversible either spontaneously or with treatment.
Unlike COPD, cystic fibrosis, and bronchiectasis, asthma is usually not a progressive disease. However, if untreated, it may cause airway remodeling, resulting in increased severity and death.
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
Pathophysiology
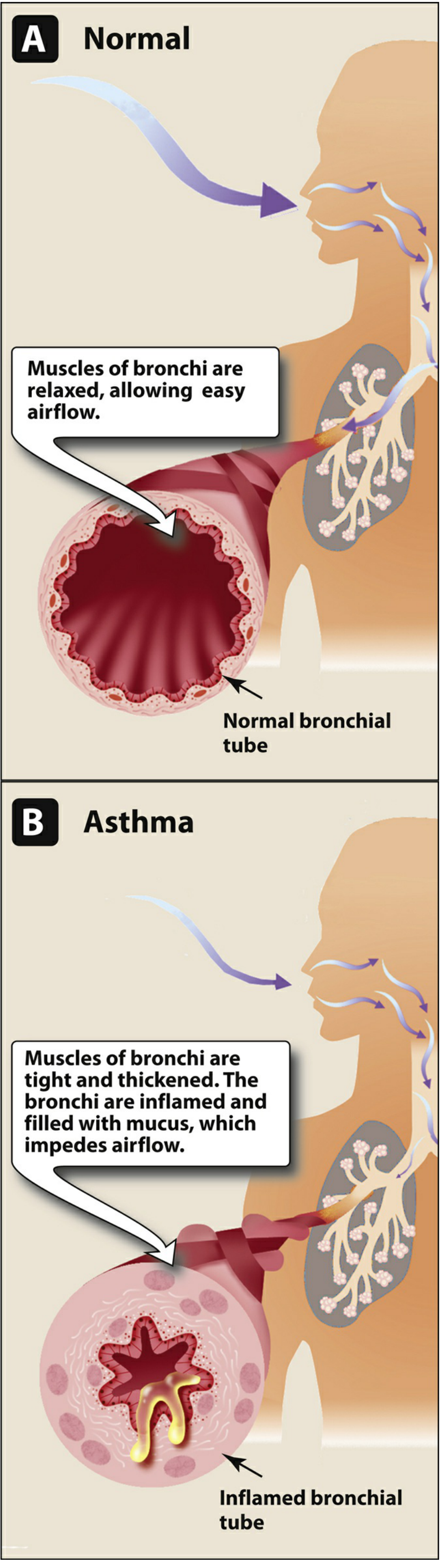
Airflow obstruction in asthma results from three key processes:
- Bronchoconstriction - contraction of bronchial smooth muscle
- Airway wall inflammation - edema of the bronchial wall, driven by eosinophils, macrophages, T lymphocytes, and mast cells
- Mucus hypersecretion - increased mucus production narrowing the lumen
The underlying chronic inflammation leads to:
- Airway hyperresponsiveness (exaggerated bronchoconstrictor response to stimuli)
- Airflow limitation (worst during expiration)
- Recurrent respiratory symptoms
- Disease chronicity and potential airway remodeling
Mediators of Inflammation
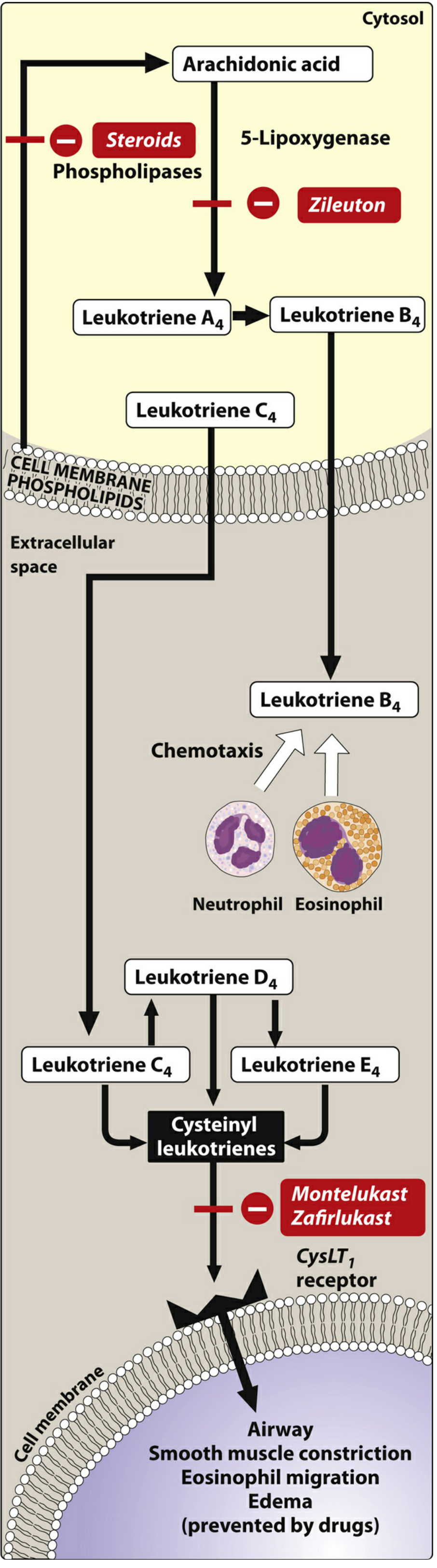
The arachidonic acid pathway is central:
-
Cysteinyl leukotrienes (LTC4, LTD4, LTE4) - cause airway smooth muscle constriction, eosinophil migration, and edema
-
LTB4 - attracts neutrophils and eosinophils via chemotaxis
-
IgE-mediated mast cell degranulation releases histamine, prostaglandins, and leukotrienes on allergen exposure
-
Lippincott Illustrated Reviews: Pharmacology
Triggers
| Category | Examples |
|---|---|
| Allergens | Dust mites, pollen, pet dander, mold, cockroach |
| Respiratory infections | Viral URIs (most common in children) |
| Exercise | Airway cooling and drying |
| Environmental irritants | Ozone, SO2, NO2, tobacco smoke, air pollution |
| Occupational agents | Ammonia, organophosphates, latex (IgE-mediated) |
| Cold air | Direct bronchoconstriction |
| GERD | Reflex bronchoconstriction |
| Stress/emotion | Neurogenic pathways |
| Medications | Aspirin, NSAIDs, beta-blockers |
Asthma frequently worsens at night (decreased mucociliary clearance, airway cooling, low endogenous catecholamines) and with exercise.
Clinical Features
- Recurrent episodes of dyspnea, chest tightness, cough, and wheezing
- Symptoms typically reversible (spontaneously or with treatment)
- Stereotypical triggers help in diagnosis
- Rapid response to beta-agonist inhalers
- Airway function fluctuates widely - PEF varies > 20% over the course of the day, lowest in the morning
- Absence of wheezing does not exclude asthma
Classification by Severity
| Classification | Symptoms | Lung Function (PEF) |
|---|---|---|
| Mild Intermittent | < 2x/week; asymptomatic between; nighttime < 2x/month | > 80% predicted |
| Mild Persistent | 1-2x/week to daily; nighttime > 2x/month | > 80% predicted |
| Moderate Persistent | Daily; nighttime > weekly; limits activity | 60-80% predicted |
| Severe Persistent | Continual; chronically limits activity; frequent nighttime | < 60% predicted |
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
Diagnosis
No single test diagnoses asthma - the diagnosis is clinical, based on history, physical exam, and spirometry.
Spirometry (Most Useful Test)
- Demonstrates obstructive pattern: reduced FEV1/FVC ratio
- Reversibility: ≥ 12% improvement AND ≥ 200 mL increase in FEV1 after bronchodilator = positive
- Severity also assessed by post-bronchodilator FEV1 (% predicted)
Other Tests
| Test | Use |
|---|---|
| Peak Expiratory Flow (PEF) | Monitoring and severity assessment |
| Methacholine challenge | Diagnose/exclude asthma when history suspicious but PFTs normal; decrease in FEV1 < 20% has 95% negative predictive value |
| Chest X-ray | Mainly to exclude other causes; may show hyperinflation |
| Eosinophil count / FeNO | Support eosinophilic asthma diagnosis; guides biologic therapy |
| Allergy testing | Identifies allergic triggers |
- Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine
Treatment
Goals of Therapy (GINA Guidelines)
- Decrease intensity and frequency of symptoms
- Prevent future exacerbations
- Minimize limitations in physical activity
- Minimize adverse effects
Step-by-Step Treatment (GINA - Patients ≥ 12 years)
| Asthma Symptoms | Preferred Controller | Reliever |
|---|---|---|
| Less than 2x/month | Low-dose ICS-formoterol as needed | (combined with controller) |
| > 2x/month but < 4-5 days/week | Low-dose ICS-formoterol as needed | (as needed) |
| Most days/week or waking ≥ 1x/week | Low-dose maintenance ICS-formoterol | Low-dose ICS-formoterol as needed |
| Daily symptoms or low lung function | Medium-dose maintenance ICS-formoterol | Low-dose ICS-formoterol as needed |
- Lippincott Illustrated Reviews: Pharmacology
Drug Classes
1. Inhaled Corticosteroids (ICS) - Foundation of Therapy
- Examples: budesonide, fluticasone, beclomethasone
- Mechanism: Inhibit phospholipase A2 → reduce arachidonic acid release → anti-inflammatory
- Decrease eosinophils, macrophages, T lymphocytes; reverse mucosal edema; reduce capillary permeability; inhibit leukotriene release
- After months of regular use: reduce airway hyperresponsiveness
- Adverse effects: oropharyngeal candidiasis, hoarseness (use spacer + rinse mouth)
- Systemic ICS (oral/IV methylprednisolone, prednisone): for severe exacerbations; no taper needed for short burst
2. Short-Acting β2 Agonists (SABAs)
- Examples: albuterol (salbutamol), levalbuterol
- Onset: 5-15 minutes; duration: 3-6 hours
- Direct relaxation of airway smooth muscle
- No anti-inflammatory effect; should not be used as monotherapy in persistent asthma
- Used as needed for quick relief; can prevent exercise-induced bronchospasm
- Adverse effects: tachycardia, hyperglycemia, hypokalemia, hypomagnesemia, skeletal muscle tremors
3. Long-Acting β2 Agonists (LABAs)
- Examples: salmeterol, formoterol
- Duration: ≥ 12 hours
- Formoterol also has rapid onset (used for both control and quick relief)
- LABA monotherapy is contraindicated in asthma - must combine with ICS
- ICS/formoterol combination (e.g., budesonide/formoterol) = preferred controller AND reliever
4. Anticholinergics
- Ipratropium (short-acting): Not for routine acute bronchospasm (slower onset than SABAs); useful add-on in ED; useful if SABA not tolerated or asthma-COPD overlap
- Tiotropium (long-acting): Add-on for severe asthma with history of exacerbations
5. Leukotriene Receptor Antagonists (LTRAs)
- Examples: montelukast, zafirlukast
- Block CysLT1 receptors → prevent smooth muscle constriction, edema, eosinophil migration
- Alternative controller option; useful in aspirin-exacerbated asthma and allergic rhinitis comorbidity
6. 5-Lipoxygenase Inhibitor
- Zileuton: Inhibits 5-lipoxygenase → blocks leukotriene synthesis
7. Theophylline
- Methylxanthine bronchodilator; now rarely used
- Narrow therapeutic window, serious adverse effects (seizures, fatal arrhythmias at toxicity), numerous drug interactions (CYP1A2/OAA substrate)
- Requires serum concentration monitoring
8. Monoclonal Antibodies (Biologics) - For Severe Persistent Asthma
| Drug | Target | Mechanism |
|---|---|---|
| Omalizumab | IgE | Binds free IgE → decreases mast cell/basophil IgE binding |
| Mepolizumab, Benralizumab, Reslizumab | IL-5 | Block eosinophil recruitment, activation, survival |
| Dupilumab | IL-4 / IL-13 | Reduces proinflammatory cytokines, chemokines, IgE |
Indicated as add-on for poorly controlled severe persistent asthma. Adverse effects include anaphylaxis (rare), arthralgias, fever, rash, increased infection risk.
Management of Exacerbations
- Mild exacerbation: FEV1 or PEF ≥ 70% predicted
- Moderate exacerbation: FEV1 or PEF 40-69%
- Severe/life-threatening: FEV1 or PEF < 40%; accessory muscle use, paradoxical breathing, altered consciousness
ED management of acute exacerbation:
- Inhaled SABA (albuterol) - first-line, repeated doses
- Ipratropium added to SABA - additional benefit in ED
- Systemic corticosteroids (IV methylprednisolone or oral prednisone) - reduce inflammation
- Supplemental oxygen to maintain SpO2 ≥ 95%
- IV magnesium sulfate - for severe exacerbations not responding to initial therapy
- Heliox, IV aminophylline - rarely used
- Intubation/mechanical ventilation - last resort
ATS Impairment Classification (for Disability Rating)
| Impairment Class | Total Score |
|---|---|
| Class 0 | Score = 0 |
| Class I | Score 1-3 |
| Class II | Score 4-6 |
| Class III | Score 7-9 |
| Class IV | Score 10-11 |
| Class V | Asthma not controlled despite maximal treatment (FEV1 < 50% despite ≥ 20 mg prednisone/day) |
Scoring is based on post-bronchodilator FEV1, reversibility/airway hyperresponsiveness (PC20), and minimum medication need.
- Murray & Nadel's Textbook of Respiratory Medicine
Recent Evidence (PubMed, 2025)
A 2025 JAMA systematic review and network meta-analysis (PMID: 39465893) on inhaled reliever therapies for asthma confirms that ICS-formoterol as needed is superior to SABA-only approaches for reducing exacerbations, supporting the GINA recommendation to move away from SABA monotherapy as a reliever.
Key Clinical Pearls
- Asthma should be in the differential diagnosis of any patient with intermittent respiratory symptoms
- The absence of wheezing does not exclude asthma
- PEF values are lowest in the morning and vary > 20% daily in asthmatics
- LABA monotherapy is contraindicated in asthma - always combine with ICS
- After ICS use: rinse mouth to prevent oropharyngeal candidiasis
- Corticosteroid short "burst" for exacerbations does not require a taper
- Downregulation of β2 receptors occurs with long-term SABA/LABA use (tolerance via GRK-mediated phosphorylation and β-arrestin internalization)
Bronchial asthama
Reading File
Finding Sources
Finding Sources
Searching PubMed
"asthma" AND "treatment guidelines"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, authoritative content from Robbins Pathology, Lippincott Pharmacology, Murray & Nadel's, and Textbook of Family Medicine. Here is the full structured answer:
Bronchial Asthma
1. Definition
Asthma is a chronic inflammatory disease of the airways characterized by recurring acute episodes of reversible airway obstruction, with return to normal lung function between episodes. In susceptible individuals, airway inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and cough - particularly at night and/or early morning.
Unlike COPD, cystic fibrosis, and bronchiectasis, asthma is usually not progressive. However, if untreated, it may cause irreversible airway remodeling, increasing severity, exacerbations, and death.
- Textbook of Family Medicine, 9e; Lippincott Illustrated Reviews: Pharmacology
2. Epidemiology & Risk Factors
-
Most common chronic disease of childhood; affects >300 million people worldwide
-
Causes >15 million disability-adjusted life-years (DALYs) annually
-
Prevalence is increasing globally
-
Strongest risk factors: household smoker exposure, family history of asthma or atopy (atopic dermatitis, allergic rhinitis)
-
High-disparity condition - hospitalization rates 3.3x higher in Black vs. White patients in the US
-
The hygiene hypothesis: reduced microbial exposure in early childhood increases risk of allergic/autoimmune disease
-
Textbook of Family Medicine, 9e
3. Types of Asthma
| Type | Key Feature |
|---|---|
| Atopic (Allergic) | Most common; Th2/IgE-mediated response to allergens; genetically predisposed |
| Non-Atopic | Triggered by viral infections, cold air, exercise; no demonstrable sensitization |
| Drug-Induced | Aspirin/NSAIDs (inhibit COX → ↓PGE2 → ↑leukotrienes); beta-blockers |
| Occupational | Fumes, organic/chemical dusts, gases (formaldehdye, toluene, epoxy resins) |
| Exercise-Induced | Airway cooling and drying during exercise |
| Cough-Variant | Chronic nocturnal cough as the only symptom (common in children) |
| Aspirin-Sensitive | Associated with nasal polyps + urticaria + recurrent rhinitis |
| Neutrophilic (Severe) | Th17-mediated; enriched for neutrophils; often refractory to corticosteroids |
- Robbins & Cotran Pathologic Basis of Disease; Textbook of Family Medicine, 9e
4. Pathogenesis
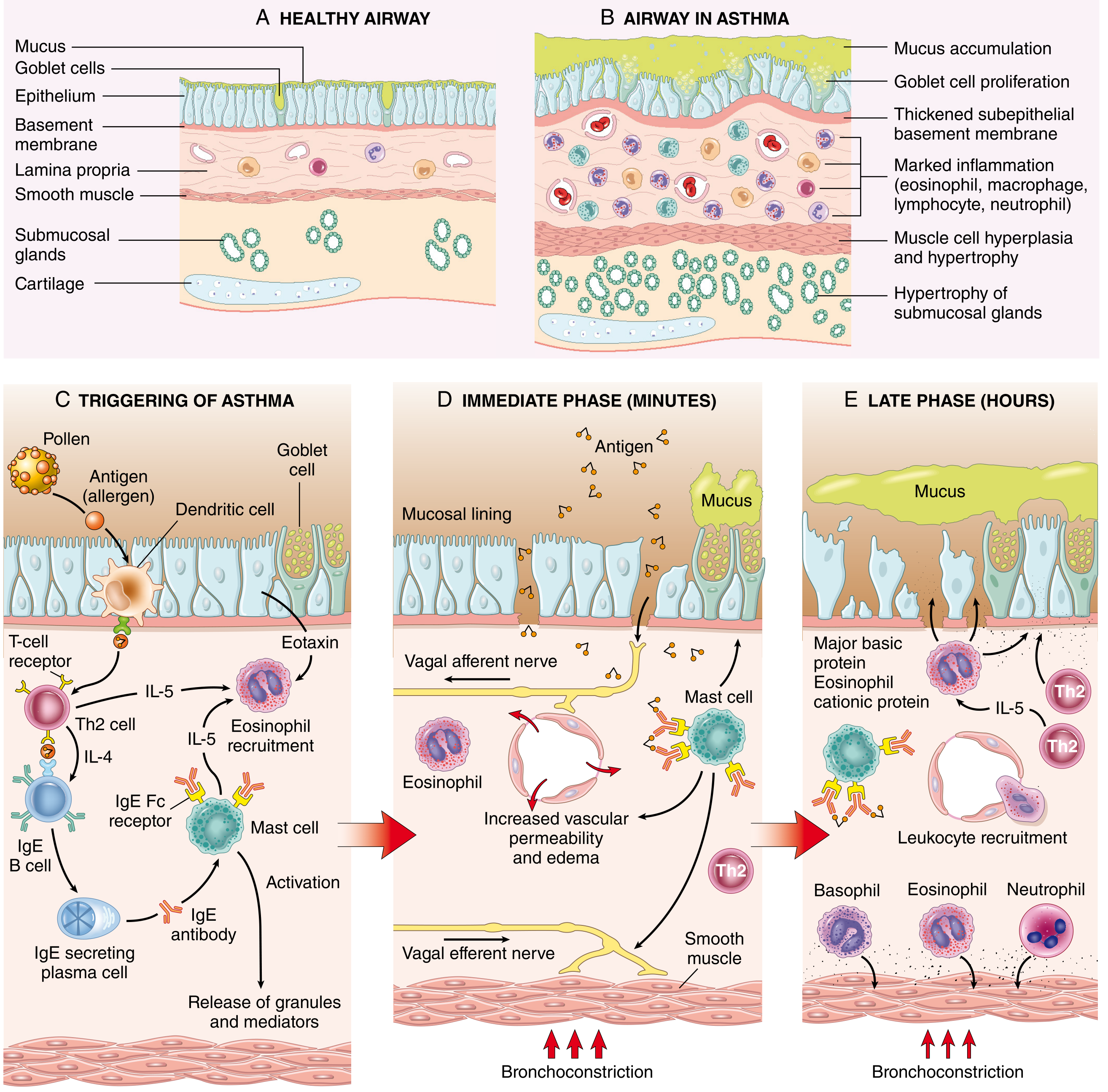
Immune Mechanism (Atopic Asthma)
The fundamental abnormality is an exaggerated Th2 response to normally harmless environmental antigens:
Step 1 - Sensitization (Panel C above):
- Antigen (allergen) is processed by dendritic cells and presented to T cells
- T cells differentiate into Th2 cells, secreting:
- IL-4 → stimulates B cells to produce IgE
- IL-5 → activates and recruits eosinophils
- IL-13 → stimulates mucus secretion from submucosal glands; promotes IgE production
- IgE binds to Fc receptors on mast cells and basophils
Step 2 - Immediate (Early) Phase (Panel D - Minutes):
- Re-exposure to allergen → cross-linking of IgE on mast cells
- Mast cells release preformed mediators (histamine, tryptase) and synthesize new mediators
- Results: bronchoconstriction (via vagal reflexes), increased vascular permeability, mucus production
- Leukotrienes C4, D4, E4 → prolonged smooth muscle constriction, edema, ↑ mucus
- Acetylcholine (parasympathetic) → smooth muscle constriction via muscarinic receptors
- Galectin-10 (GAL10) from eosinophils → forms Charcot-Leyden crystals → induces inflammation + mucus
Step 3 - Late Phase (Panel E - Hours):
- Recruitment of leukocytes: eosinophils, neutrophils, basophils, T cells, monocytes
- Eosinophils release major basic protein (MBP) and eosinophil cationic protein (ECP) → epithelial damage
- Th2 cells sustain the cycle via continued IL-5 production
- Group 2 innate lymphoid cells (ILC2s) - activated by damaged epithelial cell cytokines; amplify Th2-type responses without antigen receptors
Airway Changes in Asthma (Airway Remodeling)
Chronic exposure leads to structural remodeling:
- Thickening of the airway wall
- Sub-basement membrane fibrosis (type I and III collagen deposition)
- Goblet cell proliferation → mucus accumulation
- Hypertrophy of submucosal glands
- Smooth muscle hypertrophy and hyperplasia
- Increased vascularity (angiogenesis)
Genetics
-
Susceptibility locus on chromosome 5q near IL-3, IL-4, IL-5, IL-9, IL-13 gene cluster
-
IL-13 gene polymorphisms - strongest association with asthma/allergic disease
-
IL-4 receptor gene variants - associated with atopy, elevated total IgE, and asthma
-
HLA class II alleles linked to IgE production against specific allergens
-
IL-33 / ST2 variants - induce Th2 cytokine production
-
TSLP (thymic stromal lymphopoietin) gene variants - epithelial cytokine initiating allergic reactions
-
Robbins & Cotran Pathologic Basis of Disease
5. Airflow Obstruction Mechanism
Three simultaneous processes narrow the airway:
- Bronchoconstriction - bronchial smooth muscle contraction
- Mucosal edema and inflammation - eosinophils, macrophages, lymphocytes, neutrophils
- Mucus hypersecretion - goblet cell proliferation + submucosal gland hypertrophy
Result: Obstruction is worst during expiration → air trapping → hyperinflation
- Lippincott Illustrated Reviews: Pharmacology
6. Pathological Findings (Morphology)
Gross
- Lungs overinflated, small areas of atelectasis
- Thick, tenacious mucus plugs occluding bronchi and bronchioles
Microscopic (Sputum/BAL)
-
Curschmann spirals - extrusion of mucus plugs from subepithelial gland ducts/bronchioles
-
Charcot-Leyden crystals - composed of eosinophil-derived galectin-10
-
Eosinophilia (peripheral blood and sputum)
-
Thickened basement membrane
-
Smooth muscle hypertrophy/hyperplasia
-
Sub-basement membrane fibrosis
-
Robbins & Cotran Pathologic Basis of Disease
7. Triggers
| Category | Examples |
|---|---|
| Allergens | Dust mites, pollen, pet dander, mold, cockroaches |
| Respiratory infections | Viral URIs (rhinovirus type C, RSV) - most common |
| Exercise | Airway cooling and drying |
| Environmental irritants | Ozone, SO₂, NO₂, tobacco smoke, air pollution |
| Occupational agents | Ammonia, epoxy resins, wood/cotton dust, formaldehyde, latex |
| Cold air | Direct bronchoconstriction |
| GERD | Reflex bronchoconstriction |
| Medications | Aspirin/NSAIDs (↑ leukotrienes), beta-blockers |
| Stress/emotions | Neurogenic pathways |
Worsening predictably occurs:
- At night - decreased mucociliary clearance, airway cooling, low endogenous catecholamines
- With exercise - airway cooling and drying
8. Clinical Features
- Recurrent episodic dyspnea, chest tightness, cough, wheezing
- Symptoms often worse at night or early morning
- Rapid response to beta-agonist inhalers
- Stereotypical triggers identify individual pattern
Physical Examination Findings
| Finding | Significance |
|---|---|
| Prolonged expiratory phase | Earliest sign of airway obstruction |
| Expiratory wheezing | Classic finding (but absence does NOT exclude asthma) |
| Inspiratory + expiratory wheezing | Severe obstruction |
| Silent chest (no wheeze) | Most severe - minimal airflow |
| Accessory muscle use, nasal flaring, pursed lip breathing | Significant respiratory distress |
| Central cyanosis, altered mental status | Life-threatening |
| Pulsus paradoxus >20 mmHg | Marker of severe exacerbation |
The absence of wheezing does NOT exclude asthma.
9. Classification by Severity
| Classification | Daytime Symptoms | Nighttime Symptoms | PEF (% predicted) |
|---|---|---|---|
| Mild Intermittent | < 2 days/week | < 2 nights/month | > 80% |
| Mild Persistent | > 2 days/week, not daily | 3-4 nights/month | > 80% |
| Moderate Persistent | Daily | > 1 night/week | 60-80% |
| Severe Persistent | Continual; limits activity | Frequent (often nightly) | < 60% |
- Textbook of Family Medicine, 9e; Symptom to Diagnosis, 4th Ed.
10. Diagnosis
No single test diagnoses asthma - the diagnosis is clinical, based on history, physical examination, and objective testing.
Spirometry (Most Useful Test)
- Obstructive pattern: reduced FEV1/FVC ratio (< 70%)
- Reversibility: ≥ 12% AND ≥ 200 mL increase in FEV1 post-bronchodilator = confirms diagnosis
- PEF varies > 20% over the course of the day in asthmatics; lowest in morning
Other Investigations
| Test | Purpose |
|---|---|
| Peak Expiratory Flow (PEF) | Home monitoring; severity assessment; diurnal variation |
| Methacholine challenge | Exclude asthma when symptoms present but spirometry normal; FEV1 fall < 20% has 95% NPV |
| Chest X-ray | Exclude other diagnoses; shows hyperinflation during attacks |
| Blood eosinophil count / FeNO | Identifies eosinophilic asthma; guides biologic therapy selection |
| Serum IgE / Skin prick test | Identifies atopic triggers |
| ABG | Severe exacerbations - rising PaCO₂ = impending respiratory failure |
11. Treatment
Goals of Therapy (GINA Guidelines)
- Decrease intensity and frequency of asthma symptoms
- Prevent future exacerbations
- Maintain normal lung function (PEF/spirometry)
- Maintain normal levels of physical activity
- Minimize adverse effects of medications
GINA Step-Based Treatment (≥12 years)
| Asthma Symptoms | Preferred Controller | Preferred Reliever |
|---|---|---|
| < 2 days/month | Low-dose ICS-formoterol as needed | (combined, no separate reliever) |
| > 2x/month, < 4-5 days/week | Low-dose ICS-formoterol as needed | (as needed) |
| Most days, OR waking ≥ 1 night/week | Low-dose maintenance ICS-formoterol | Low-dose ICS-formoterol as needed |
| Daily + low lung function | Medium-dose maintenance ICS-formoterol | Low-dose ICS-formoterol as needed |
- Lippincott Illustrated Reviews: Pharmacology (GINA guidelines)
12. Pharmacotherapy
Leukotriene Pathway (Drug Targets)
A. Inhaled Corticosteroids (ICS) - Foundation of Therapy
- Examples: budesonide, fluticasone, beclomethasone, mometasone
- Mechanism: Inhibit phospholipase A2 → ↓ arachidonic acid → anti-inflammatory; decrease eosinophils, macrophages, T lymphocytes; reverse mucosal edema; inhibit leukotriene release
- After months of regular use: reduce airway hyperresponsiveness
- Adverse effects: Oropharyngeal candidiasis, hoarseness (local immune suppression)
- Prevention: use spacer + rinse mouth ("swish-and-spit") after each dose
- Systemic (IV methylprednisolone / oral prednisone): for severe exacerbations; short burst does not require a taper
B. Short-Acting β₂ Agonists (SABAs)
- Examples: albuterol (salbutamol), levalbuterol
- Onset: 5-15 minutes; duration: 3-6 hours
- Direct relaxation of airway smooth muscle via ↑ cAMP
- No anti-inflammatory effect - must NOT be used as monotherapy in persistent asthma
- Use: as-needed quick relief; prevention of exercise-induced bronchospasm
- Adverse effects: tachycardia, hyperglycemia, hypokalemia, hypomagnesemia, skeletal muscle tremors
C. Long-Acting β₂ Agonists (LABAs)
- Examples: salmeterol (slow onset), formoterol (rapid onset + long duration)
- Duration: ≥ 12 hours
- LABA monotherapy is CONTRAINDICATED in asthma - always combine with ICS
- ICS/formoterol (e.g., budesonide/formoterol) = preferred controller AND reliever
- Downregulation of β₂ receptors occurs with chronic use (GRK phosphorylation → β-arrestin internalization)
D. Anticholinergics
- Ipratropium (SAMA): Block vagally mediated smooth muscle contraction; slower onset than SABAs; add-on in acute severe exacerbations in ED; useful in COPD-asthma overlap
- Tiotropium (LAMA): Add-on for severe asthma with frequent exacerbations
- Adverse effects: xerostomia (dry mouth), bitter taste
E. Leukotriene Modifiers
- LTRAs - Montelukast, Zafirlukast: Block CysLT₁ receptors → prevent smooth muscle constriction, edema, eosinophil migration
- Zileuton: 5-Lipoxygenase inhibitor → blocks leukotriene synthesis
- Particularly useful in aspirin-sensitive asthma and when allergic rhinitis is a comorbidity
F. Theophylline
- Methylxanthine bronchodilator; rarely used now
- Replaced by β₂ agonists and ICS due to narrow therapeutic window
- Toxicity: seizures, potentially fatal arrhythmias
- CYP1A2/OAA substrate - numerous drug interactions
- Requires serum concentration monitoring when used chronically
G. Monoclonal Antibodies (Biologics) - Severe Persistent Asthma
| Drug | Target | Mechanism |
|---|---|---|
| Omalizumab | IgE | Binds free IgE → ↓ mast cell/basophil activation |
| Mepolizumab | IL-5 | ↓ Eosinophil recruitment, activation, survival |
| Benralizumab | IL-5 receptor | ↓ Eosinophil survival (rapid depletion) |
| Reslizumab | IL-5 | ↓ Eosinophil recruitment (IV) |
| Dupilumab | IL-4 / IL-13 | ↓ Proinflammatory cytokines, chemokines, IgE |
- Indicated for add-on therapy in severe persistent asthma poorly controlled on conventional therapy
- Adverse effects: anaphylaxis (rare), arthralgias, fever, rash, ↑ infection risk, new malignancies reported
13. Management of Acute Exacerbations
Severity Assessment
| Severity | FEV1/PEF | Features |
|---|---|---|
| Mild | ≥ 70% | Normal speech, no accessory muscle use |
| Moderate | 40-69% | Speaks in phrases, some accessory muscle use |
| Severe/Life-threatening | < 40% | Words only, cyanosis, altered consciousness, silent chest |
Acute Management (ED/Hospital)
- Inhaled SABA (albuterol via nebulizer) - repeated doses, first-line
- Ipratropium added to SABA - additional bronchodilation in ED
- Systemic corticosteroids (IV methylprednisolone or oral prednisone) - anti-inflammatory, reduce recovery time
- Supplemental oxygen - target SpO₂ ≥ 95%
- IV magnesium sulfate - for severe exacerbations not responding to initial therapy
- Heliox (helium-oxygen mixture) - reduces work of breathing in severe obstruction
- NIV (BiPAP) / Mechanical ventilation - last resort for respiratory failure
Danger Signs (Impending Respiratory Failure)
- Rising PaCO₂ (normalization of CO₂ in severe asthma = impending failure - these patients are normally hypocapnic)
- Decreasing SpO₂ despite O₂ therapy
- Exhaustion, altered mental status
- Silent chest
14. Special Considerations
Asthma in Pregnancy
- Affects ~4% of pregnant women
- One-third will have exacerbations during pregnancy
- Moderate-to-severe asthma increases risk of preterm labor, low birth weight, perinatal death, preeclampsia
- FEV1 and PEF remain unchanged in normal pregnancy; residual volume decreases
- Management: Same as non-pregnant patients; risks of uncontrolled asthma outweigh medication risks
Aspirin-Sensitive Asthma (Samter's Triad)
- Asthma + nasal polyps + aspirin/NSAID hypersensitivity
- Mechanism: COX inhibition → ↓ PGE₂ → ↑ leukotrienes (LTB4, C4, D4, E4)
- Treatment: leukotriene modifiers particularly effective; desensitization possible
15. Key Clinical Pearls
- Asthma should be considered in any patient with intermittent respiratory symptoms
- The absence of wheezing does NOT exclude asthma
- PEF values are lowest in the morning and vary >20% daily in uncontrolled asthma
- LABA monotherapy is contraindicated in asthma - always pair with ICS
- Rinse mouth after ICS to prevent oropharyngeal candidiasis
- Short corticosteroid bursts for exacerbations do NOT require a taper
- Up to 50% of childhood asthma remits in adolescence, but may return in adulthood
- A rising PaCO₂ in an acute attack = ominous sign - patient is fatiguing
Sources: Robbins & Cotran Pathologic Basis of Disease; Lippincott Illustrated Reviews: Pharmacology; Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume; Textbook of Family Medicine, 9e; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.