tmj
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough overview of the TMJ:
Temporomandibular Joint (TMJ)
Anatomy
The TMJ is a synovial joint formed by the mandibular condyle articulating with the mandibular (glenoid) fossa of the temporal bone, just anterior to the external auditory canal.
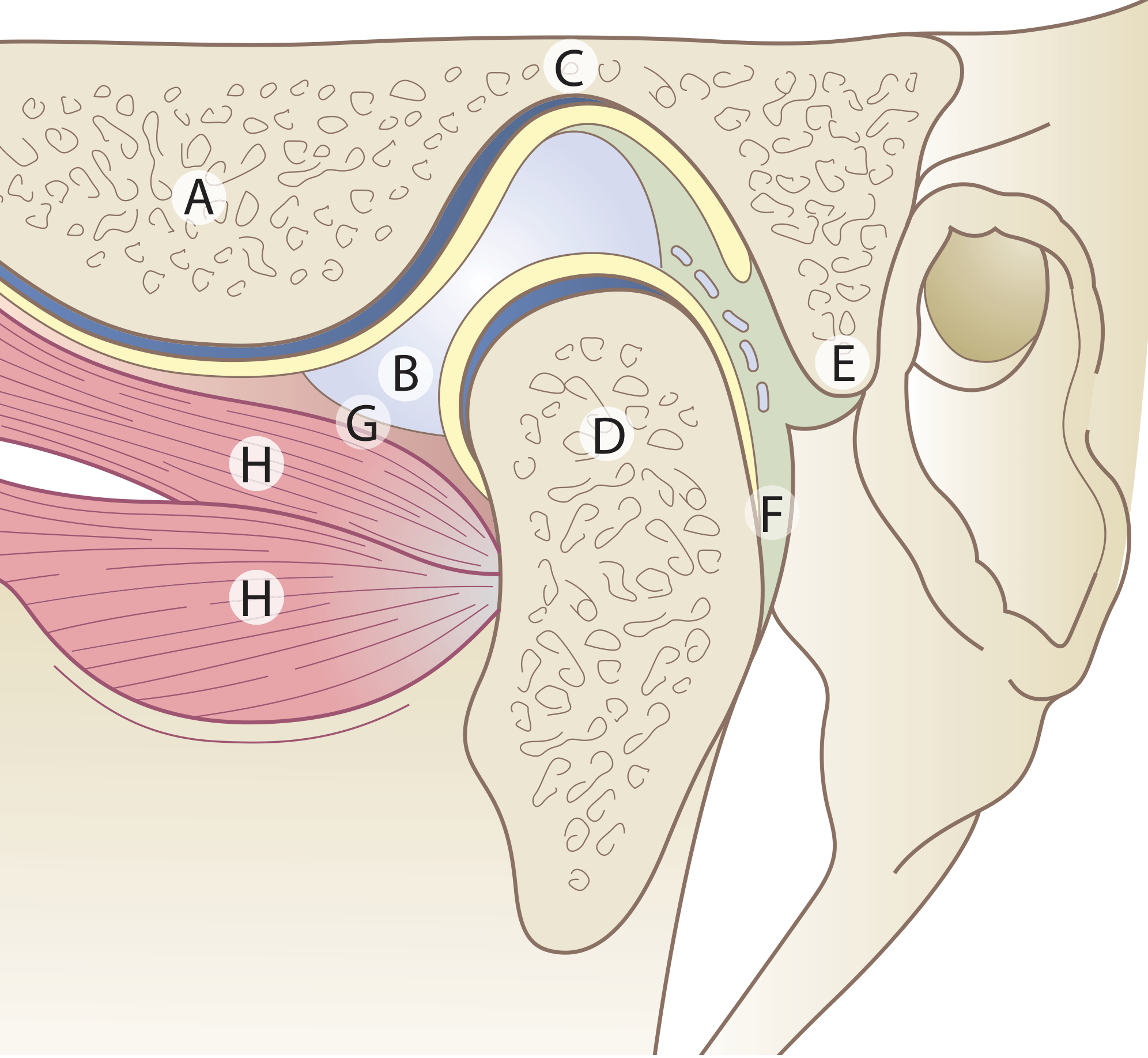
TMJ cross-section: A=Articular eminence, B=Articular disc, C=Mandibular fossa, D=Condyle, E=Upper (fibro-elastic) lamina, F=Lower (non-elastic) lamina, G=Capsule, H=Lateral pterygoid muscle (Scott-Brown's Otorhinolaryngology)
Unique features of the TMJ
- Divided joint space - an intra-articular disc separates the cavity into upper and lower compartments
- Fibrous (not hyaline) articular cartilage - reflects the joint's intramembranous development
- Secondary condylar cartilage - present in the condyle head until adolescence
- Tooth-influenced movement - unlike other synovial joints
Biomechanics
- Lower compartment: hinge (rotation) movement - dominates during normal mouth opening
- Upper compartment: gliding (translational) movement - occurs with wide opening as the condyle-disc complex slides anteriorly along the articular eminence
- Normal maximal mouth opening: 3-6 cm (measured between upper and lower incisors)
Key Structures
| Structure | Detail |
|---|---|
| Articular disc (meniscus) | Dense fibrous, avascular centrally; concavo-convex superiorly, concave inferiorly |
| Capsule | Thin, slack; attached above to the mandibular fossa, below to the neck of the condyle; lined internally by synovial membrane |
| Synovial fluid | Contains proteoglycans; subatmospheric pressure at rest, greatly elevated during mastication |
| Condylar neck | Common mandible fracture site; has the pterygoid fovea for lateral pterygoid attachment |
| Lateral pterygoid | Key muscle; upper head attaches to the disc, lower head to the condyle |
Temporomandibular Disorder (TMD)
Definition
TMD is defined as "aching in the muscles of mastication, sometimes with occasional brief severe pain on chewing, often associated with restricted jaw movement and clicking or popping sounds."
Risk Factors / Etiology
- Jaw clenching and grinding (bruxism), often stress-related
- Fatigue/spasm of head, neck, and masticatory muscles
- Tooth malocclusion (less common than previously thought)
- Inflammatory arthritis (RA, OA, infectious arthritis)
- Emotional stress
- Excessive gum chewing or prolonged wide mouth opening
Clinical Features
- Pain anterior to the auricular canal, may radiate to ear, eye, face, head, and neck
- Pain worse with jaw movement (chewing, yawning, laughing)
- Joint sounds: clicking, popping, or crepitus on range of motion
- Restricted jaw movement
- Headache, facial pain, or earache may be presenting complaints
Examination
- Palpate just anterior to the external auditory canal while patient opens/closes and moves jaw side to side
- Assess for asymmetry (suggests unilateral involvement)
- Measure incisor separation for vertical range (normal 3-6 cm)
Differential Diagnosis
Pulpitis, odontogenic infection, headache, otitis media, sinusitis, parotitis, trigeminal neuralgia, tumors, neuromuscular disorders
TMJ Dislocation
- Condyle travels anterior to the articular eminence and locks there
- Masseter, internal pterygoid, and temporalis go into spasm - causing trismus
- Usually bilateral; unilateral dislocation causes jaw deviation to the opposite side
- Causes: extreme mouth opening (yawning), prolonged dental procedures, trauma, dystonic drug reactions
- Recurrent dislocations are common
Reduction Technique
Thumbs placed intraorally lateral to the lower molars; pressure applied downward and backward over the molar ridge near the jaw angle until the condyle clears the articular eminence and muscle contraction returns the jaw to normal position.
TMD Management
| Approach | Details |
|---|---|
| First-line | NSAIDs, heat (15 min sessions), or cold therapy |
| Soft diet | Reduce mechanical stress on the joint |
| Bite guards/splints | Especially for bruxism; shown effective up to 6 months |
| Cyclobenzaprine | Muscle relaxant, given at night |
| Behavioral modification | Jaw relaxation techniques |
| Isometric exercises | Jaw opening, lateral deviation, jaw thrusting |
| Occlusal adjustment | If malocclusion is contributing |
| Hyaluronate injection | Insufficient evidence |
| Surgery | Reserved for severe, refractory cases |
Systemic Arthritis and the TMJ
- Many arthritides affect the TMJ, including juvenile and adult RA
- In children, TMJ involvement can cause micrognathia from arrested mandibular bone growth
- TMD is thought by some to be a form of myofascial pain, similar to fibromyalgia
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 41
- ROSEN's Emergency Medicine, Ch. 56
- Firestein & Kelley's Textbook of Rheumatology, Ch. on Joint Examination
- Textbook of Family Medicine 9e, Appendix 32-6
This is a shared conversation. Sign in to Orris to start your own chat.