Ancylostoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have a comprehensive, well-illustrated picture of Ancylostoma. Let me compile the full answer.
Ancylostoma (Hookworm)
Taxonomy and Species
Ancylostoma is a genus of parasitic nematodes (roundworms) in the family Ancylostomatidae. The clinically important species include:
| Species | Primary Host | Disease in Humans |
|---|---|---|
| A. duodenale | Humans | Hookworm disease (Old World hookworm) |
| Necator americanus | Humans | Hookworm disease (New World hookworm) |
| A. ceylanicum | Dogs/cats | Can cause true intestinal infection in humans |
| A. caninum | Dogs | Eosinophilic enteritis (Australia) |
| A. braziliense | Dogs/cats | Cutaneous larva migrans |
While Necator americanus is technically a separate genus, it is classified alongside A. duodenale as the two main agents of human hookworm disease (ancylostomiasis).
Epidemiology
-
Over 700 million people are infected with hookworms globally; approximately 460 million cases by some estimates
-
Prevalence is highest in sub-Saharan Africa and Asia
-
Endemic in tropical/subtropical zones between 45°N and 30°S of the equator - the larval stage cannot withstand freezing temperatures
-
A. duodenale predominates in northern Africa, the Middle East, southern Europe, and parts of Asia ("Old World hookworm")
-
N. americanus has a more widespread distribution in the Americas, tropical Africa, and Southeast Asia ("New World hookworm")
-
Approximately 44 million pregnant women are infected worldwide
-
Risk factors: poor sanitation, barefoot walking, use of human excrement as fertilizer
-
Yamada's Textbook of Gastroenterology, p. 3117; Park's Textbook of Preventive and Social Medicine, p. 284
Life Cycle
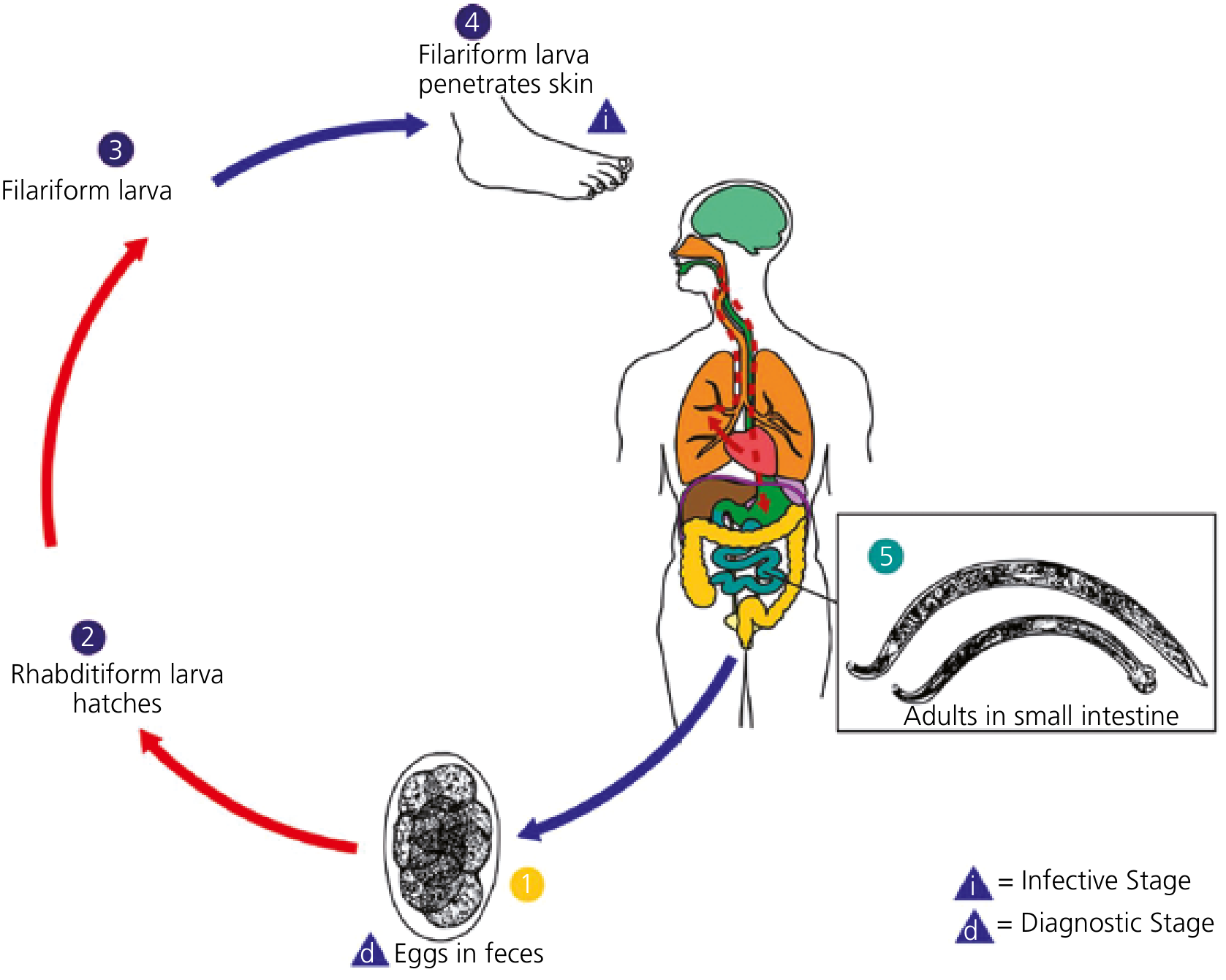
Step-by-step:
- Eggs in feces (diagnostic stage) - Adult female worms in the small intestine produce thousands of eggs daily: A. duodenale ~10,000-30,000 eggs/day; N. americanus ~5,000-10,000 eggs/day. Eggs pass with stool into soil.
- Rhabditiform larva hatches - In warm, moist soil, eggs embryonate and hatch within 1-2 days, releasing non-infective rhabditiform larvae.
- Filariform larva - The rhabditiform larva molts twice over 5-10 days in soil to become the infective third-stage filariform larva. These can survive in shaded, moist soil for up to 1 month.
- Skin penetration (infective stage) - Filariform larvae penetrate exposed skin (usually the feet), enter the venous circulation, and travel to the pulmonary vasculature. (A. duodenale can also be transmitted orally.)
- Lung migration - Larvae penetrate alveoli, ascend the bronchial tree to the trachea, are coughed up and swallowed.
- Adult worms in small intestine - Larvae mature in the small intestine over 5-9 weeks. Adults inhabit the proximal small intestine (mainly the jejunum), attaching to intestinal villi. A. duodenale survives ~1 year; N. americanus survives 3-5 years.
- Goldman-Cecil Medicine, p. 3477
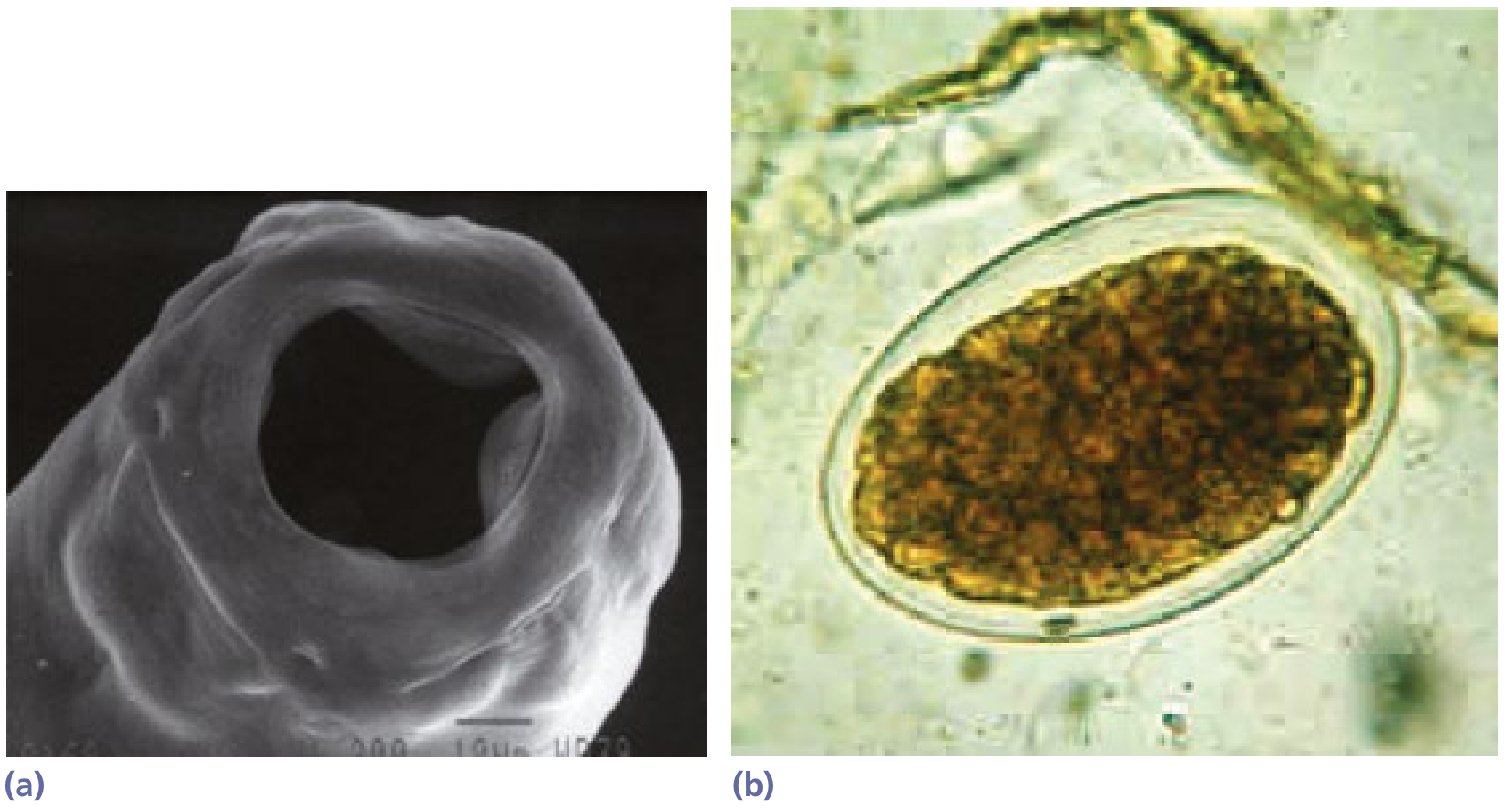
Morphology and Pathobiology
-
Adult worms measure 7-13 mm in length; males slightly smaller than females
-
Anterior end is dorsally curved (hence "hookworm")
-
Attachment mechanism: A. duodenale has cutting teeth; N. americanus has a rounded cutting plate
-
Each worm aspirates a plug of intestinal villus tissue, secretes anticoagulant and anti-platelet enzymes, and ingests blood - moving to fresh villi several times per minute
-
Blood loss per worm per day: N. americanus = 0.03-0.1 mL; A. duodenale = 0.15-0.26 mL (A. duodenale causes significantly more blood loss)
-
Hemoglobinases within the worm's digestive canal degrade host hemoglobin as a nutrient source
-
The major pathology is gastrointestinal blood loss → iron deficiency anemia
-
Goldman-Cecil Medicine, p. 3477; Yamada's Textbook of Gastroenterology, p. 3117
Clinical Manifestations
1. Ground Itch (Skin entry)
- Pruritic, erythematous, papular rash - typically on hands/feet - representing a hypersensitivity reaction at the site of larval skin penetration
2. Cutaneous Larva Migrans (CLM)
- Caused by zoonotic hookworms (A. caninum, A. braziliense) that penetrate human skin but cannot complete the life cycle
- Intensely pruritic, erythematous, serpiginous (snake-like) tracks on feet, legs, buttocks
- Tracks advance a few mm to cm per day; vesiculobullous lesions may form; self-resolves within weeks to months
3. Pulmonary Phase (Larval migration)
- Dry cough, sore throat, wheezing, low-grade fever
- Wakana syndrome (oral ingestion of A. duodenale larvae) - pharyngeal irritation, cough, dyspnea, hoarseness, nausea, vomiting
4. Intestinal Phase - Hookworm Disease
-
Heavy infections (≥2000 eggs/gram of feces) cause iron deficiency anemia: weakness, palpitation, dizziness, dyspnea, fatigue, headache
-
Hypoproteinemia and anasarca with very heavy worm burdens (protein loss)
-
Gastrointestinal symptoms per se are uncommon; the main disease is anemia
-
Endoscopy shows punctate mucosal erosions and pooling of blood in the small bowel lumen
-
Children are most vulnerable to chronic sequelae: stunted growth, cognitive impairment, malnutrition
-
Goldman-Cecil Medicine, p. 3477-3478
Diagnosis
-
Stool microscopy - identification of characteristic thin-shelled, oval eggs containing segmented larvae (4-8 cells at the time of passage); this is the gold standard
-
Quantitative stool examination (e.g., Kato-Katz technique) to estimate worm burden
-
PCR - highly sensitive and specific; currently available only in specialized/research laboratories
-
Peripheral eosinophilia is typically present
-
CBC may reveal hypochromic microcytic anemia
-
Serum albumin may be low in heavy infections
-
No need to differentiate between hookworm species clinically
-
Yamada's Textbook of Gastroenterology, p. 3118; Goldman-Cecil Medicine, p. 3478
Treatment
| Infection | First-line | Alternatives |
|---|---|---|
| Hookworm (A. duodenale / N. americanus) | Albendazole 400 mg daily x 3 days | Tribendimidine 400 mg once; Mebendazole 500 mg daily or 100 mg bid x 3 days; Pyrantel pamoate 11 mg/kg x 3 days (max 1 g/day) |
| Cutaneous larva migrans (A. caninum, A. braziliense) | Ivermectin 200 μg/kg once | Albendazole 400 mg daily x 3 days |
-
Iron supplementation (with folic acid) is essential for anemia treatment
-
Treat hypoproteinemia and hypereosinophilia as needed
-
Goldman-Cecil Medicine, p. 3479 (Table 327-1); Park's Textbook, p. 287
Prevention and Control
Primary prevention:
- Proper sanitary disposal of human excreta
- Provision of safe water and food hygiene
- Wearing protective footwear (the single most effective individual measure)
- Health education on use of sanitary latrines
Secondary prevention / WHO Mass Drug Administration (MDA):
-
Periodic deworming of at-risk groups without individual diagnosis in endemic areas:
- Preschool children, school-aged children
- Women of childbearing age (including pregnant women in 2nd/3rd trimester)
- Adults in high-risk occupations (tea-pickers, miners)
-
Once yearly if community prevalence >20%; twice yearly if >50%
-
Drugs used: albendazole (400 mg single dose) or mebendazole (500 mg single dose)
-
Park's Textbook of Preventive and Social Medicine, p. 287
Key Comparison: A. duodenale vs N. americanus
| Feature | A. duodenale | N. americanus |
|---|---|---|
| Common name | Old World hookworm | New World hookworm |
| Geography | Europe, Middle East, N. Africa, S. Asia | Americas, tropical Africa, SE Asia (more widespread) |
| Buccal cavity | 2 pairs of cutting teeth | Cutting plates (semilunar) |
| Egg output | ~28,000/day | ~10,000/day |
| Daily blood loss/worm | 0.15-0.26 mL | 0.03-0.1 mL |
| Lifespan in host | ~1 year | 3-5 years |
| Route of infection | Skin AND oral | Skin only |
| Size | Slightly larger | Slightly smaller |
Sources: Goldman-Cecil Medicine (9780323930345); Yamada's Textbook of Gastroenterology (9781119600169); Park's Textbook of Preventive and Social Medicine (9789382219163)
This is a shared conversation. Sign in to Orris to start your own chat.