rheumatoid arthritis according to davidson 24th edition
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND ("treatment"[MeSH Terms] OR "diagnosis"[MeSH Terms])
Finding Sources
Searching PubMed
"rheumatoid arthritis" AND management
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material. Let me compose the full answer.
Note on your request: Davidson's Principles and Practice of Medicine, 24th Edition is not available in this textbook library. The most current and authoritative internal medicine references available are Goldman-Cecil Medicine (International Edition) and Harrison's Principles of Internal Medicine, 22nd Edition (2025). The content below draws from both, which share a very high degree of overlap with Davidson's coverage of RA, and reflects current clinical standards.
Rheumatoid Arthritis
Sources: Goldman-Cecil Medicine (International Edition); Harrison's Principles of Internal Medicine, 22e (2025)
Definition
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease of unknown etiology that primarily targets synovial tissues. While the joint is the primary target, systemic inflammation underlies a variety of coexistent comorbidities including cardiovascular disease, osteoporosis, cognitive dysfunction, psychiatric illness, and cancer.
Epidemiology
- Global prevalence: 0.5-1% of adults
- Women are affected ~3x more than men before menopause
- Overall annualized incidence: ~40/100,000 in women, ~20/100,000 in men
- Can occur at any age; prevalence increases with each decade
- Extreme geographic variation: near-zero prevalence in some rural Nigerian cohorts vs. ~5% in certain Native American populations (Chippewa, Yakima, Inuit)
- Incidence may be declining, possibly related to reduced smoking rates
Pathobiology
Genetics
- Monozygotic twin concordance: 12-15%; dizygotic twins: 2-5%
- Heritability: ~60%
- Polygenic disorder with >100 identified SNPs - most implicate immune genes
- ~40% of genetic risk in the HLA region
- Key HLA-DR alleles: DRB*0401, DRB*0404, DRB*0101, DRB*1402 - all share the "shared epitope" in the peptide-binding groove
- Non-HLA loci include PTPN22, CTLA-4, STAT4, PADI4
Environmental Factors
- Smoking is the strongest environmental risk factor; causes citrullination of proteins in the lung
- Periodontal disease, gut and respiratory microbiome alterations implicated
- Female sex hormones, vitamin D deficiency, obesity also contribute
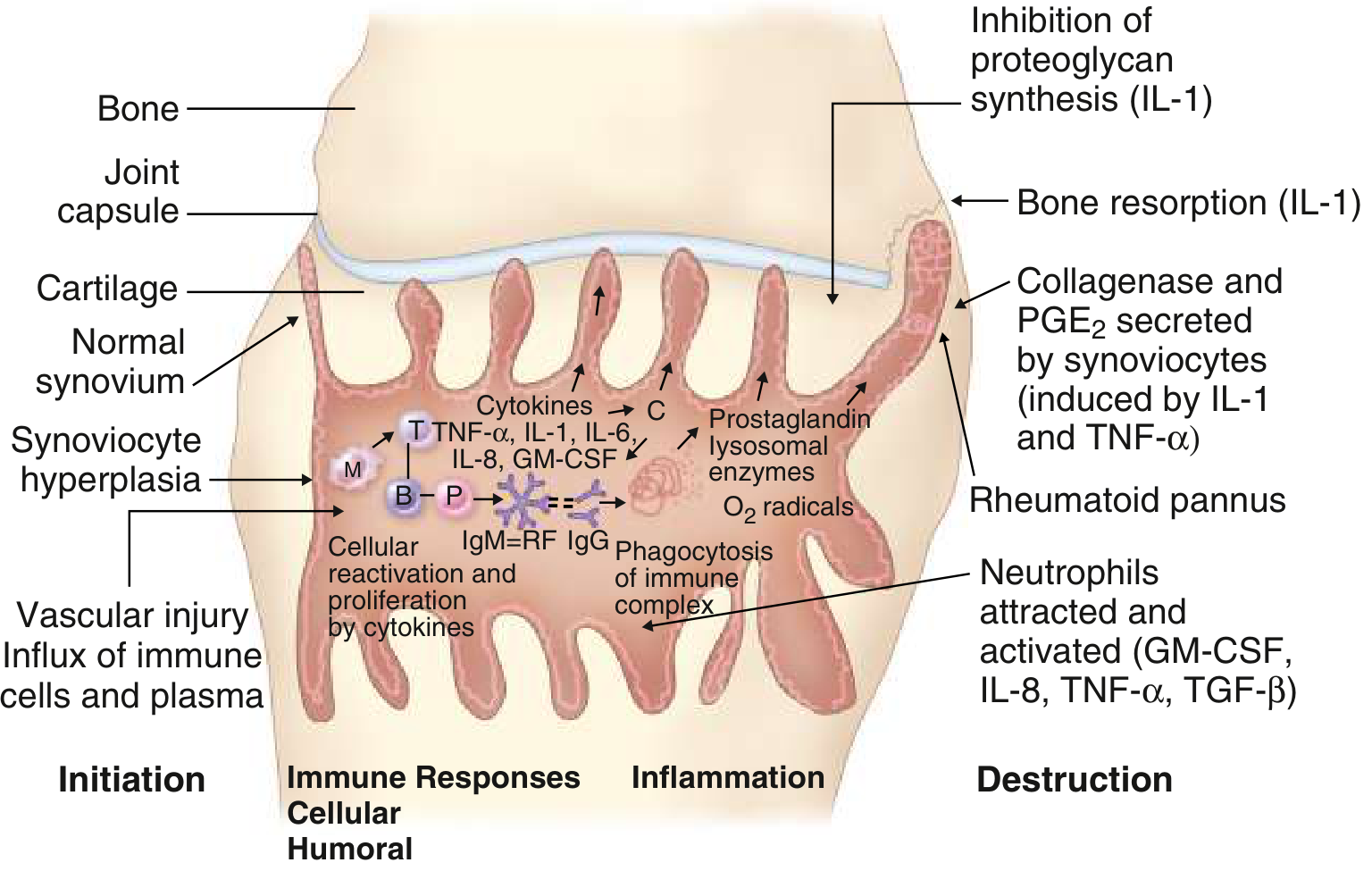
Pathogenesis
The disease progresses through recognizable stages:
1. Loss of Tolerance (Pre-clinical phase, up to 10 years before clinical disease)
- Citrullination or acetylation of self-proteins triggers autoantibody formation
- Anti-citrullinated protein antibodies (ACPAs/anti-CCP) appear years before clinical arthritis
- Rheumatoid factor (RF) - IgM anti-IgG antibody - also appears early
2. Synovial Inflammation
- T cells (especially CD4+ Th17 and Th1 cells), B cells, macrophages, mast cells, and fibroblast-like synoviocytes (FLS) accumulate in the synovium
- Key cytokines: TNF-α, IL-1, IL-6, IL-17, GM-CSF, IL-8
- RF and ACPAs form immune complexes that activate complement, promote macrophage activation via FcR binding, and activate osteoclasts
3. Joint Destruction
- FLS are partially transformed cells with anchorage independence, loss of contact inhibition, and TLR expression; they release MMPs (MMP1, MMP3, MMP13) and prostanoids, attacking the cartilage-pannus junction
- Osteoclasts - activated by RANKL, IL-1, TNF, IL-17 - cause the characteristic periarticular bone erosions
- "Bone edema" on MRI precedes visible erosions on X-ray
4. Systemic Comorbidities
- Circulating cytokines and immune complexes activate endothelium, accelerate atherosclerosis, drive systemic osteoporosis, fatigue, and depression
Clinical Features
Articular Manifestations
Onset: Usually insidious over weeks to months; occasionally acute. Morning stiffness lasting >1 hour is a hallmark.
Joint pattern:
- Typically starts in small joints of hands (MCP, PIP) and feet (MTP)
- DIP joints are spared (distinguishing from OA and psoriatic arthritis)
- Symmetric polyarthritis is characteristic
- Later: wrists, knees, elbows, ankles, hips, shoulders
- Cervical spine (C1-C2) commonly involved - atlantoaxial subluxation can cause myelopathy
Deformities in advanced disease:
- Ulnar deviation of MCP joints
- Swan-neck deformity (PIP hyperextension, DIP flexion)
- Boutonniere deformity (PIP flexion, DIP hyperextension)
- Z-thumb deformity
- Baker's cyst (popliteal synovial cyst)

Other joints:
- Temporomandibular, cricoarytenoid (hoarseness, rarely acute respiratory distress), sternoclavicular joints may be involved
Extra-articular Manifestations
More common in RF/ACPA-positive seropositive patients:
| System | Manifestation |
|---|---|
| Skin | Subcutaneous nodules (~20%), small vessel vasculitis (brown digital infarcts) |
| Lung | Pleuritis, interstitial lung disease, pulmonary nodules, Caplan syndrome (with pneumoconiosis) |
| Heart | Pericarditis, accelerated atherosclerosis, ↑ cardiovascular mortality |
| Eye | Keratoconjunctivitis sicca (secondary Sjogren), scleritis, episcleritis |
| Neurologic | Carpal tunnel syndrome, tarsal tunnel syndrome, mononeuritis multiplex, cervical myelopathy |
| Haematologic | Anaemia of chronic disease, thrombocytosis (active disease), thrombocytopenia (Felty) |
| Felty syndrome | Triad: RA + splenomegaly + neutropenia (in severe seropositive disease; now rare) |
| Systemic | Fatigue, weight loss, low-grade fever |
Diagnosis
Classification Criteria (2010 ACR/EULAR)
Used as both classification and diagnostic aids:
| Domain | Score |
|---|---|
| Joint involvement | 1 large joint = 0; 2-10 large joints = 1; 1-3 small joints = 2; 4-10 small joints = 3; >10 joints (at least 1 small) = 5 |
| Serology (RF or ACPA) | Negative = 0; low positive = 2; high positive (>3× ULN) = 3 |
| Acute-phase reactants (CRP or ESR) | Normal = 0; abnormal = 1 |
| Duration of symptoms | <6 weeks = 0; ≥6 weeks = 1 |
Score ≥6 = definite RA
Note: DIP joints, first MTP joints, and first carpometacarpal joints are excluded from the joint count.
Laboratory Findings
- RF positive in ~75% of patients; associated with more severe disease and extra-articular features
- RF is non-specific - also positive in SLE, Sjogren, hepatitis, endocarditis, etc.
- ACPA (anti-CCP antibodies) - highly specific (~96%), appear early; even in first weeks of arthritis suggests more aggressive RA
- ESR and CRP elevated (reflect disease activity)
- Full blood count: normochromic normocytic anaemia, thrombocytosis in active disease
- Seronegative RA: ~25-30% with true RA are RF and ACPA negative
- Synovial fluid: turbid, WBC 5,000-50,000/mm³ (predominantly neutrophils), low glucose, low complement
Imaging
- X-ray: Periarticular osteoporosis (early), joint space narrowing, marginal erosions (later - at MCP, wrist); cervical spine subluxation
- MRI: Most sensitive for early synovitis and bone erosions - "bone edema" predates X-ray changes
- Ultrasound: Confirms synovitis and erosions in early disease; power Doppler shows active vascularity
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Osteoarthritis | DIP involvement, Heberden/Bouchard nodes, negative RF, mechanical pain |
| Systemic lupus erythematosus | Non-erosive arthritis, multi-organ, ANA positive |
| Psoriatic arthritis | DIP involvement, skin/nail changes, dactylitis, RF negative |
| Gout | Tophi, hyperuricemia, strongly positive birefringent crystals |
| Reactive arthritis | Preceded by infection, asymmetric, lower limb, HLA-B27 |
| Viral arthritis | Self-limited (2-3 weeks), exposure history, may have RF |
| Sjogren syndrome | Dry eyes/mouth prominent, anti-Ro/La antibodies |
Management
Principles
- Early, aggressive therapy to prevent joint damage and disability
- Treat-to-target (T2T) - aim for low disease activity or remission
- Frequent modification of DMARD therapy if target not achieved
- Individualization of therapy
- Minimize chronic glucocorticoid use
- Combination DMARD therapy where appropriate
Monitoring Disease Activity
Composite indices used:
- DAS-28 (Disease Activity Score - 28 joints)
- SDAI (Simplified Disease Activity Index)
- CDAI (Clinical Disease Activity Index)
- ACR 20/50/70 improvement criteria (used in trials)
- RAPID3 (Routine Assessment of Patient Index Data)
Step 1: NSAIDs
- Role: Adjunctive - symptom control only, no disease modification
- Mechanism: Non-selective COX-1/COX-2 inhibition
- Minimize chronic use due to GI and renal toxicity
Step 2: Glucocorticoids
- "Bridge therapy" while waiting for DMARD effect (weeks to months)
- Short bursts (1-2 weeks) for acute flares
- Chronic low-dose: prednisone 5-10 mg/day only if DMARD therapy inadequate
- Avoid prednisone >10 mg/day for articular disease
- Always combine with a DMARD; osteoporosis prophylaxis mandatory (bisphosphonates - avoid in women of childbearing age)
Step 3: Conventional (Synthetic) DMARDs
| Drug | Dose | Key Points |
|---|---|---|
| Methotrexate (MTX) | 7.5-25 mg PO/SQ once weekly | First-choice DMARD; folic acid supplementation required |
| Hydroxychloroquine | 200-400 mg daily (5 mg/kg) | Mild disease; monitor for retinal toxicity |
| Sulfasalazine | 500 mg → 2 g/day (divided) | Useful alone or in triple therapy |
| Leflunomide | 10-20 mg once daily | Alternative/add-on to MTX |
| Azathioprine | 1-2.5 mg/kg/day | Reserved for special situations |
Oral triple therapy (HCQ + MTX + SSZ) is an effective alternative to biologics for early RA.
Step 4: Biologic DMARDs
Used when conventional DMARDs fail:
| Class | Drug | Dose/Route |
|---|---|---|
| Anti-TNF-α | Adalimumab | 40 mg SQ every 2 weeks |
| Etanercept | 50 mg SQ weekly | |
| Infliximab | 3-5 mg/kg IV at 0, 2, 6 weeks, then q4-8 wk (with MTX) | |
| Certolizumab | 400 mg SQ at weeks 0, 2, 4 → 200 mg q2 wk | |
| Golimumab | 50 mg SQ monthly | |
| Anti-IL-6R | Tocilizumab | 4→8 mg/kg IV q4 wk; or SQ 162 mg q1-2 wk |
| Anti-CD20 | Rituximab | 2 × 1000 mg IV (2 wk apart) q16-24 wk + MTX |
| CTLA-4-Ig (co-stimulation blockade) | Abatacept | 500-1000 mg IV q4 wk (weight-based) |
Key points:
- MTX + anti-TNF is superior to MTX alone for both symptoms and radiographic progression
- Switching to abatacept may be more effective than switching between anti-TNF agents after failure
- Screen for TB (latent TB), hepatitis B/C before starting biologics
Step 5: Targeted Synthetic DMARDs (JAK Inhibitors)
| Drug | Dose |
|---|---|
| Tofacitinib | 5 mg PO twice daily |
| Baricitinib | 2 or 4 mg PO once daily |
| Upadacitinib | 15 mg PO once daily |
JAK inhibitors block intracellular signaling downstream of multiple cytokine receptors. Use with caution due to risks of VTE, serious infections, and cardiovascular events (particularly in patients >65 years or with CV risk factors).
Treatment Algorithm (ACR 2021 Guidelines)
DMARD-naive with moderate/high disease activity
↓
Start METHOTREXATE (±short-term glucocorticoids as bridge)
↓ (reassess at 3-6 months)
Inadequate response?
↓
Add HCQ + SSZ (triple therapy) OR Add biologic (anti-TNF ± MTX) OR Non-TNF biologic ± MTX
↓
Inadequate response to anti-TNF?
↓
Switch to another anti-TNF OR Switch to non-TNF biologic (abatacept, rituximab, tocilizumab) OR JAK inhibitor
Target: remission (DAS-28 <2.6; SDAI ≤3.3; or Boolean criteria) or low disease activity (DAS-28 <3.2)
Prognosis
- Most patients have a lifelong, fluctuating course
- Predictors of worse outcome: high RF/ACPA titers, elevated CRP/ESR, early erosions, high burden of joint involvement
- Increased mortality mainly from accelerated cardiovascular disease
- Preclinical RA trials: some DMARDs may delay but not yet prevent disease onset
Recent Evidence
Two recent reviews supplement the above:
- Rheumatoid arthritis: key clinical features and challenges (2024) - DI Matteo A, Emery P, Panminerva Med [PMID: 39621317]
- Management strategies in rheumatoid arthritis (2024) - Konzett V, Aletaha D, Nat Rev Rheumatol [PMID: 39448800]
These reviews do not contradict the above guidelines but emphasize the evolving role of JAK inhibitors and cardiovascular risk monitoring.
Note: Davidson's 24th Edition is not in the library. This answer draws from Goldman-Cecil Medicine (International Edition) and Harrison's 22e (2025), which are the most current internal medicine references available and cover RA in equivalent depth.
This is a shared conversation. Sign in to Orris to start your own chat.