Excellent material gathered. Here is the full synthesis:
Acute Ischemic Stroke: Imaging and Management
Pathophysiology in Brief
Ischemic stroke results from vessel occlusion by thromboembolism or atherosclerotic plaque, causing focal brain ischemia. Two zones form:
- Ischemic core: irreversibly infarcted (CBF <10 mL/100g/min) - dead within minutes
- Penumbra: ischemic but not yet infarcted (CBF 10-20 mL/100g/min) - potentially salvageable with reperfusion
The entire premise of imaging and management is: identify and save the penumbra before it joins the core.
IMAGING
The "Code Stroke" CT Protocol
The standard imaging triage for acute stroke is a 3-step CT protocol performed simultaneously as a single rapid acquisition:
1. Non-contrast CT (NCCT) → exclude hemorrhage, assess ASPECTS
2. CT Angiography (CTA) → identify LVO, assess collaterals
3. CT Perfusion (CTP) → core vs penumbra mismatch (selected patients)
MRI (particularly DWI) is an alternative when available without delaying treatment.
1. Non-Contrast CT (NCCT) - First and Always
Primary purpose: Exclude hemorrhagic stroke (absolute contraindication to thrombolysis and thrombectomy).
Early ischemic signs on NCCT (appear within 3-6 hours, may be subtle):
| Sign | Appearance | Significance |
|---|
| Hyperdense MCA sign | Bright white MCA on unenhanced CT | Acute thrombus in MCA - suggests LVO |
| Hyperdense basilar sign | Bright basilar artery | Basilar artery occlusion |
| Loss of grey-white differentiation | Blurring of insular ribbon, lentiform nucleus | Early cytotoxic edema |
| Sulcal effacement | Loss of cortical sulci | Early cerebral swelling |
| "Dot sign" | Hyperdense dot in sylvian fissure branches | Distal MCA branch thrombus |
"Large cortical infarcts might not be detected by NCCT up to 3 hours from onset, and around 40% of infarcts can be missed by 24 hours."
ASPECTS Score (Alberta Stroke Program Early CT Score)
The ASPECTS system scores early ischemic changes in the MCA territory on NCCT. The brain is divided into 10 regions (M1-M6 cortical + C caudate, L lentiform, IC internal capsule, I insula):
- Each region scores 1 point if normal
- Subtract 1 point for each region showing early ischemic change
- Score 10 = no ischemic change (ideal)
- Score ≤7 = poor prognosis for independent recovery
- Score ≥6 traditionally required for thrombectomy eligibility (now reassessed - see below)
Posterior circulation ASPECTS (pc-ASPECTS) is also increasingly used but requires further validation.
2. CT Angiography (CTA) - Identify the Occlusion
CTA from aortic arch to vertex is performed immediately after NCCT. This is now considered standard in all acute stroke patients.
What CTA provides:
- Identifies the large vessel occlusion (LVO) site: ICA terminus, M1, M2, basilar artery, etc.
- Collateral circulation grading - good collaterals = larger salvageable penumbra = more time for treatment
- Rules out underlying vascular lesions (dissection, stenosis)
- CTA source images (CTA-ASPECTS) are superior predictors of final infarct size compared to NCCT-ASPECTS, because they directly show the degree of collateral perfusion
3. CT Perfusion (CTP) - Core vs Penumbra Mismatch
CTP measures four parameters:
| Parameter | What it measures | Core/Penumbra |
|---|
| CBF (Cerebral Blood Flow) | ml/100g/min | Core = severely reduced (<30% contralateral) |
| CBV (Cerebral Blood Volume) | ml/100g | Core = CBV markedly reduced |
| MTT (Mean Transit Time) | Seconds | Penumbra = prolonged |
| Tmax (Time to peak) | Seconds | Penumbra = Tmax >6 seconds |
Mismatch = Tmax >6s region (at-risk territory) MINUS CBF core (infarcted territory). A large mismatch means large salvageable penumbra - the patient benefits from reperfusion.
Used for patient selection in:
- Extended thrombolysis window (4.5-9 hours) - EXTEND trial
- Late-window thrombectomy (6-24 hours) - DAWN and DEFUSE-3 trials
4. MRI - More Sensitive, Used When Available
MRI is more sensitive than NCCT for early infarct detection, but logistics (time, availability, contraindications) often make CT the primary tool.
DWI (Diffusion-Weighted Imaging) - Most Important Sequence
- Detects ischemic core within minutes of onset - the earliest sequence to show infarction
- Restricted diffusion (bright on DWI, dark on ADC map) = cytotoxic edema from Na-K ATPase failure
- Sensitivity ~80-95% for acute infarction (note: false negatives exist, especially in posterior fossa, small lacunes, and hyperacute <6 hours)
- DWI-FLAIR mismatch: DWI bright + FLAIR normal = stroke likely within 4.5 hours (used in WAKE-UP trial for unknown-onset stroke treatment)
MRI Sequences in Acute Stroke
| Sequence | Role |
|---|
| DWI | Identify ischemic core (minutes to hours) |
| ADC map | Confirm restricted diffusion (dark = true infarct) |
| FLAIR | Edema, old infarcts; DWI-FLAIR mismatch for timing |
| GRE/SWI | Hemorrhage (microbleeds, hemorrhagic transformation), thrombus |
| MRA | Non-contrast vessel imaging - identifies LVO |
| PWI (perfusion) | Core-penumbra mismatch (DWI-PWI mismatch) |
| T2 | Chronic infarcts, white matter disease |
5. Imaging Sequence Summary by Time Window
| Time from onset | Imaging Protocol | Purpose |
|---|
| 0-6 hours ("early window") | NCCT + CTA ± CTP | Rule out ICH, identify LVO for thrombectomy |
| 4.5-9 hours (extended tPA) | NCCT + CTP or DWI-FLAIR MRI | Mismatch for IV tPA eligibility |
| 6-24 hours (late thrombectomy) | NCCT + CTA + CTP or DWI MRI | Clinical-imaging or perfusion mismatch for thrombectomy (DAWN/DEFUSE-3 criteria) |
| Unknown onset ("wake-up stroke") | MRI DWI-FLAIR mismatch | Proxy for <4.5h onset (WAKE-UP trial) |
MANAGEMENT
Emergency Assessment - "Time is Brain"
Every 1 minute of untreated LVO = ~1.9 million neurons lost. Key targets:
- Door-to-needle time (IV tPA): <60 minutes
- Door-to-groin puncture (thrombectomy): <90 minutes
Immediate steps:
- Airway, breathing, circulation - stabilize
- Blood glucose (hypoglycemia mimics stroke - treat if <60 mg/dL)
- NCCT + CTA (CT protocol as above)
- 12-lead ECG (AF is common stroke cause)
- IV access, bloods: FBC, coagulation, metabolic panel
- NIHSS scoring
A. Intravenous Thrombolysis (IV tPA / Alteplase)
Mechanism: Alteplase (rt-PA) activates plasminogen to plasmin, dissolving the fibrin clot systemically.
Dose: 0.9 mg/kg (max 90 mg); 10% as IV bolus, remainder over 60 minutes.
Time windows:
| Window | Evidence | Notes |
|---|
| 0-3 hours | NINDS (1995) - landmark trial | FDA approved; maximum benefit |
| 3-4.5 hours | ECASS-III (2008) | Extended benefit; some additional exclusions apply |
| 4.5-9 hours | EXTEND trial (2019) | Requires CTP mismatch showing salvageable tissue |
| Unknown onset | WAKE-UP trial (2018) | Requires DWI+ / FLAIR- MRI mismatch |
"The EXTEND study randomized patients presenting between 4.5 and 9 hours after onset - favorable outcome at 90 days was present in more patients in the alteplase group (35.4% vs 29.5%)." - Fuster and Hurst's The Heart, 15th Ed.
Key tPA Contraindications
| Absolute Contraindications | Relative Contraindications |
|---|
| Intracranial hemorrhage on CT | Recent surgery (<14 days) |
| Ischemic stroke within 3 months | Major trauma (<14 days) |
| Active internal bleeding | Anticoagulant use (INR >1.7, heparin with elevated PTT) |
| Severe head trauma (<3 months) | Blood glucose <50 or >400 mg/dL |
| Platelet count <100,000 | Large infarct (ASPECTS ≤3) |
| BP >185/110 mmHg (uncontrolled) | Recent MI |
Note on Tenecteplase: Emerging as an alternative to alteplase - single IV bolus (0.25 mg/kg), similar efficacy, more convenient; gaining traction in guidelines (2024 ESO, AHA/ASA updates).
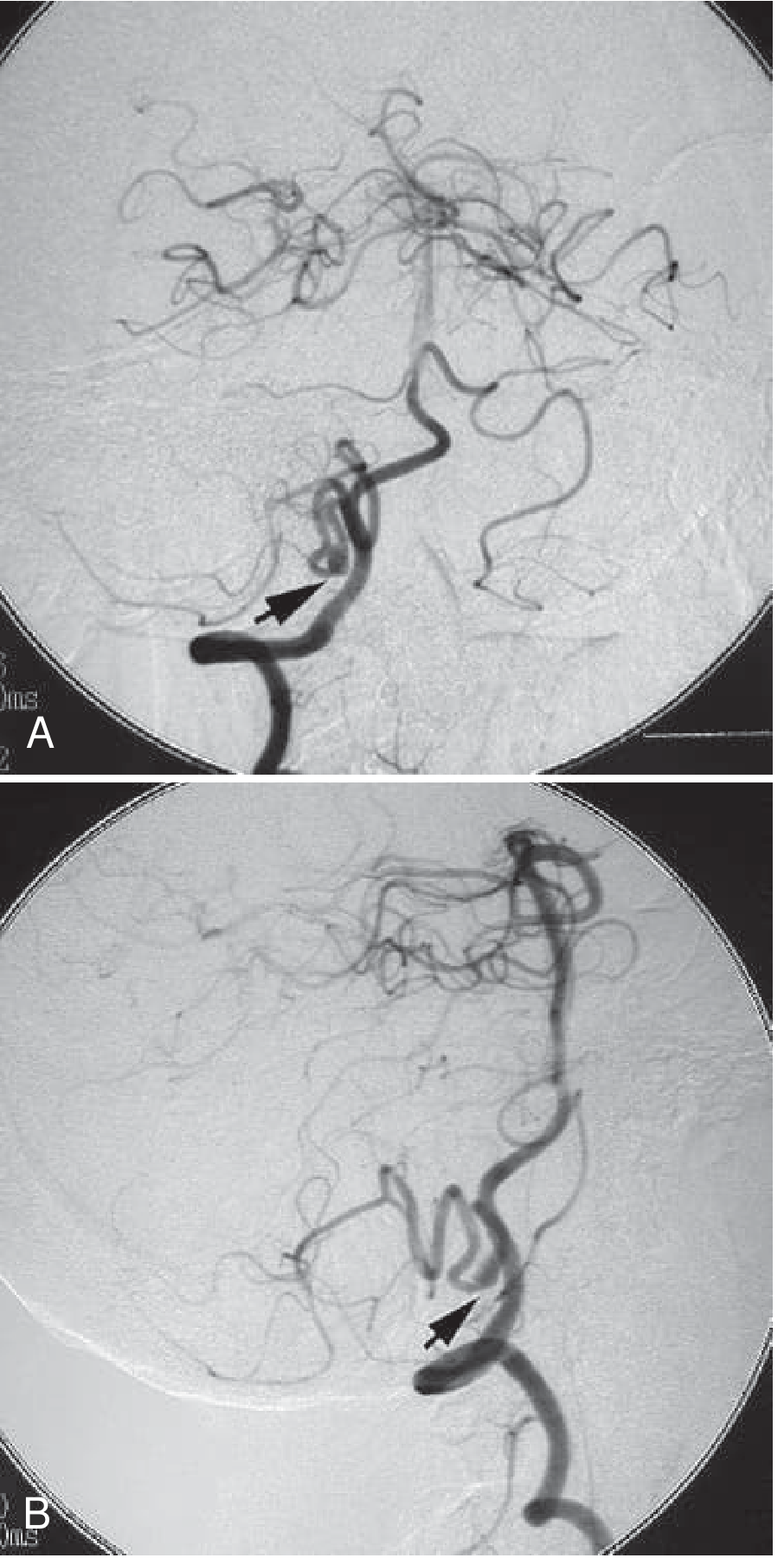
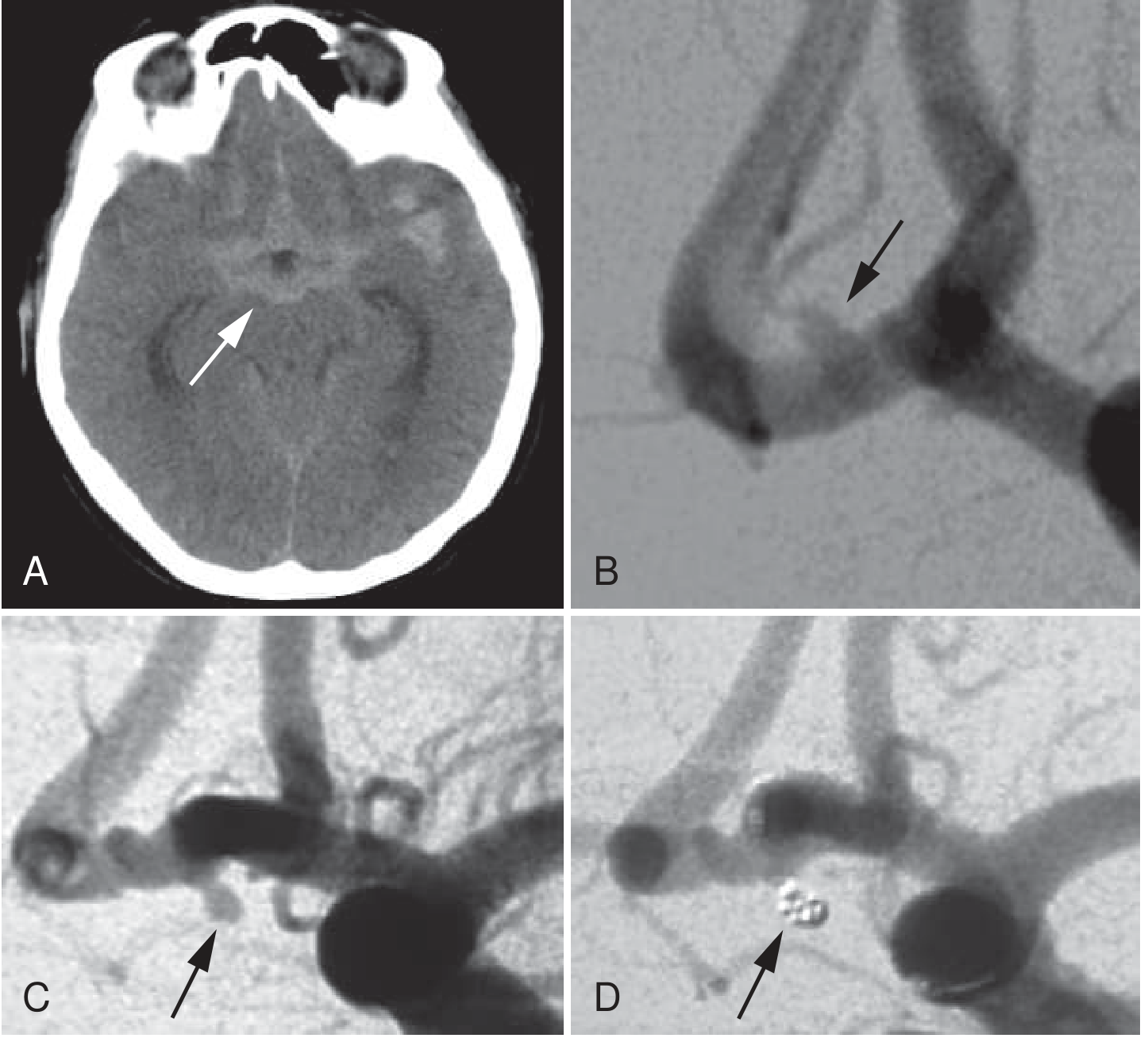
B. Mechanical Thrombectomy (MT) - LVO Stroke
Thrombectomy is now the standard of care for LVO stroke - one of the most effective interventions in modern medicine with an NNT of 2.6 to reduce disability by one mRS level (HERMES meta-analysis).
Devices:
- Stent retrievers (Solitaire, Trevo): deployed beyond the clot, then withdrawn with clot engaged in mesh
- Large-bore aspiration catheters (Penumbra): direct suction thrombectomy - equivalent to stent retrievers in ASTER and COMPASS trials
- Often combined: aspiration + stent retriever ("Solumbra technique")
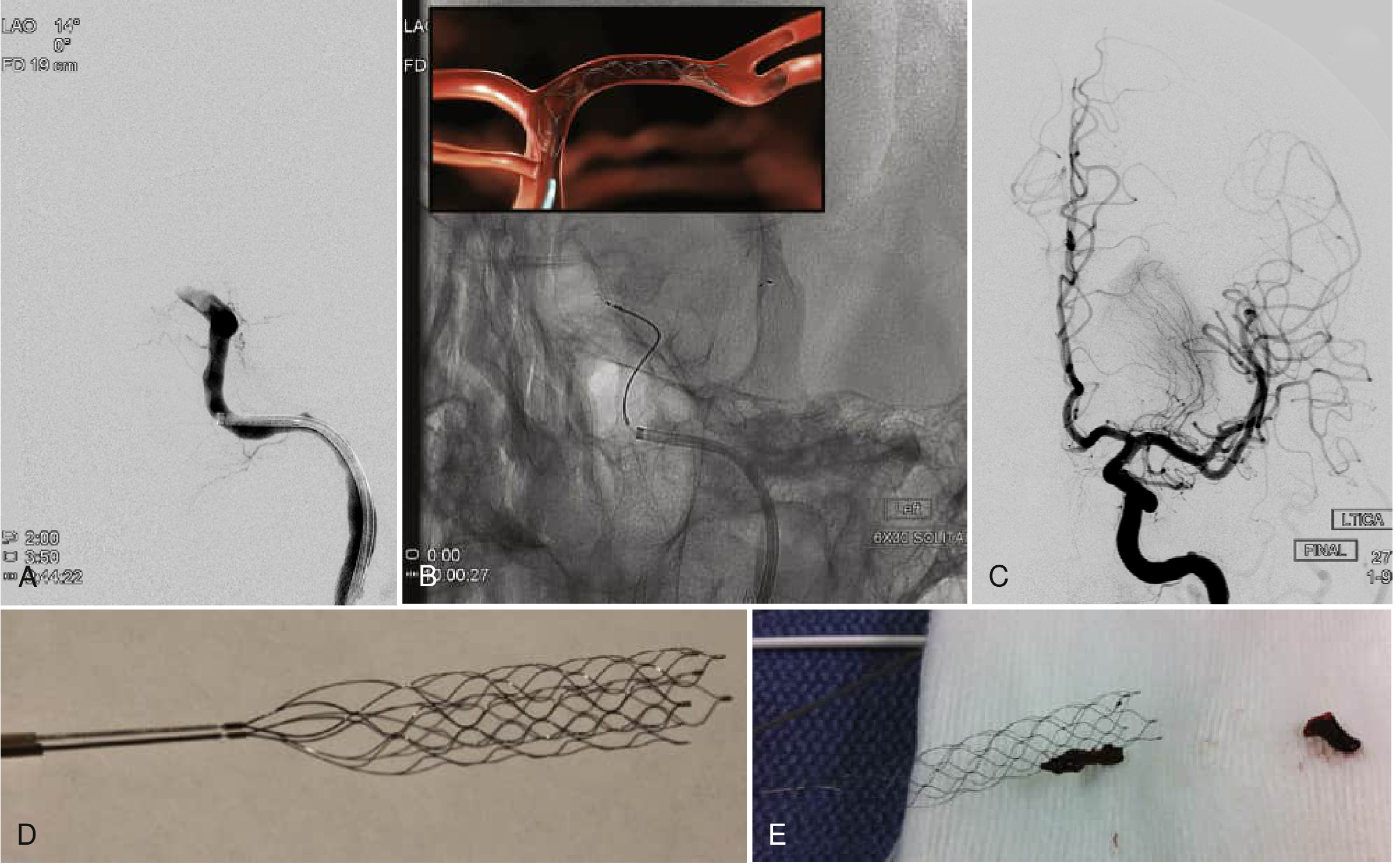
Endovascular mechanical thrombectomy: (A) Left ICA terminal occlusion on DSA; (B) Solitaire stent retriever deployed in LCA under fluoroscopy; (C) Complete recanalization of ICA and MCA post-thrombectomy; (D-E) Solitaire FR device with retrieved clot fragments. (Fuster & Hurst's The Heart, 15th Ed.)
Thrombectomy Time Windows and Criteria
Early window (0-6 hours): Five landmark 2015 trials (MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, EXTEND-IA) established benefit. Selection: NIHSS ≥6, confirmed LVO on CTA, ASPECTS ≥6, good functional baseline (mRS 0-2).
Late window (6-24 hours) - DAWN and DEFUSE-3:
| Trial | Window | Selection | Key Result |
|---|
| DAWN (2018) | 6-24 h | Clinical-infarct mismatch (NIHSS vs core volume by CTP/DWI); ICA or M1 occlusion | mRS 0-2: 49% vs 13% (NNT=2.8); stopped early for efficacy |
| DEFUSE-3 (2018) | 6-16 h | Perfusion mismatch: core <70mL, Tmax>6s:core ratio ≥1.8; NIHSS ≥6 | mRS 0-2: 45% vs 17% (P<0.001) |
"Patients who present in this delayed window are thought to be slow progressors, with leptomeningeal collaterals that help sustain salvageable brain tissue." - Fuster and Hurst's The Heart, 15th Ed.
Large core thrombectomy (new 2023-2024 evidence):
Previously, ASPECTS ≤5 or large infarct core was considered a contraindication. Four recent trials (TENSION, SELECT-2, ANGEL-ASPECTS, LASTE, all 2023) demonstrated benefit of thrombectomy even with ASPECTS 3-5 and core volumes up to 100 mL - expanding eligibility significantly. Guidelines are now being updated to reflect this.
"First pass effect" - achieving complete recanalization in a single device pass - is strongly associated with better clinical outcomes and is now a benchmark for device performance.
C. Blood Pressure Management
- Pre-tPA: Must lower BP to <185/110 mmHg before administration (IV labetalol or nicardipine); maintain <180/105 for 24h after
- No thrombolysis/thrombectomy candidate: Permissive hypertension up to 220/120 mmHg for 24-48h (allows autoregulation in penumbra)
- Post-thrombectomy (successful recanalization): Target <180/105 mmHg to reduce risk of reperfusion hemorrhage
- 2025 ESO update (PMID 42095756): Reaffirms cautious approach to BP lowering in acute phase
D. Antiplatelet Therapy
- No LVO/thrombolysis: Aspirin 300 mg loading dose within 48 hours (IST and CAST trials)
- Post-tPA: Hold antiplatelet and anticoagulants for 24 hours (re-image first to exclude hemorrhagic transformation)
- TIA/minor stroke: Dual antiplatelet therapy (aspirin + clopidogrel) for 21 days (POINT and CHANCE trials)
E. Neuroprotective / Supportive Measures
| Intervention | Target | Rationale |
|---|
| Glucose control | 140-180 mg/dL | Both hyper- and hypoglycemia worsen outcome |
| Temperature | Normothermia (<37.5°C) | Hyperthermia expands infarct |
| Oxygen | SpO2 >94%; avoid hyperoxia | Supplemental O2 only if hypoxic |
| Positioning | Head of bed 0-30° (flat preferred acutely) | Maximize CBF to penumbra |
| Anticoagulation | Avoid in first 24-48h | Hemorrhagic transformation risk |
| DVT prophylaxis | Compression stockings; LMWH after 24-48h | Immobility risk |
F. Functional Outcomes (Modified Rankin Scale)
| mRS | Description |
|---|
| 0 | No symptoms |
| 1 | Minimal symptoms, no disability |
| 2 | Slight disability but independent |
| 3 | Moderate disability - walks independently, needs some help |
| 4 | Moderately severe - unable to walk, needs assistance |
| 5 | Severe - bedridden, incontinent |
| 6 | Dead |
mRS 0-2 = "good functional outcome" is the primary endpoint in all stroke trials.
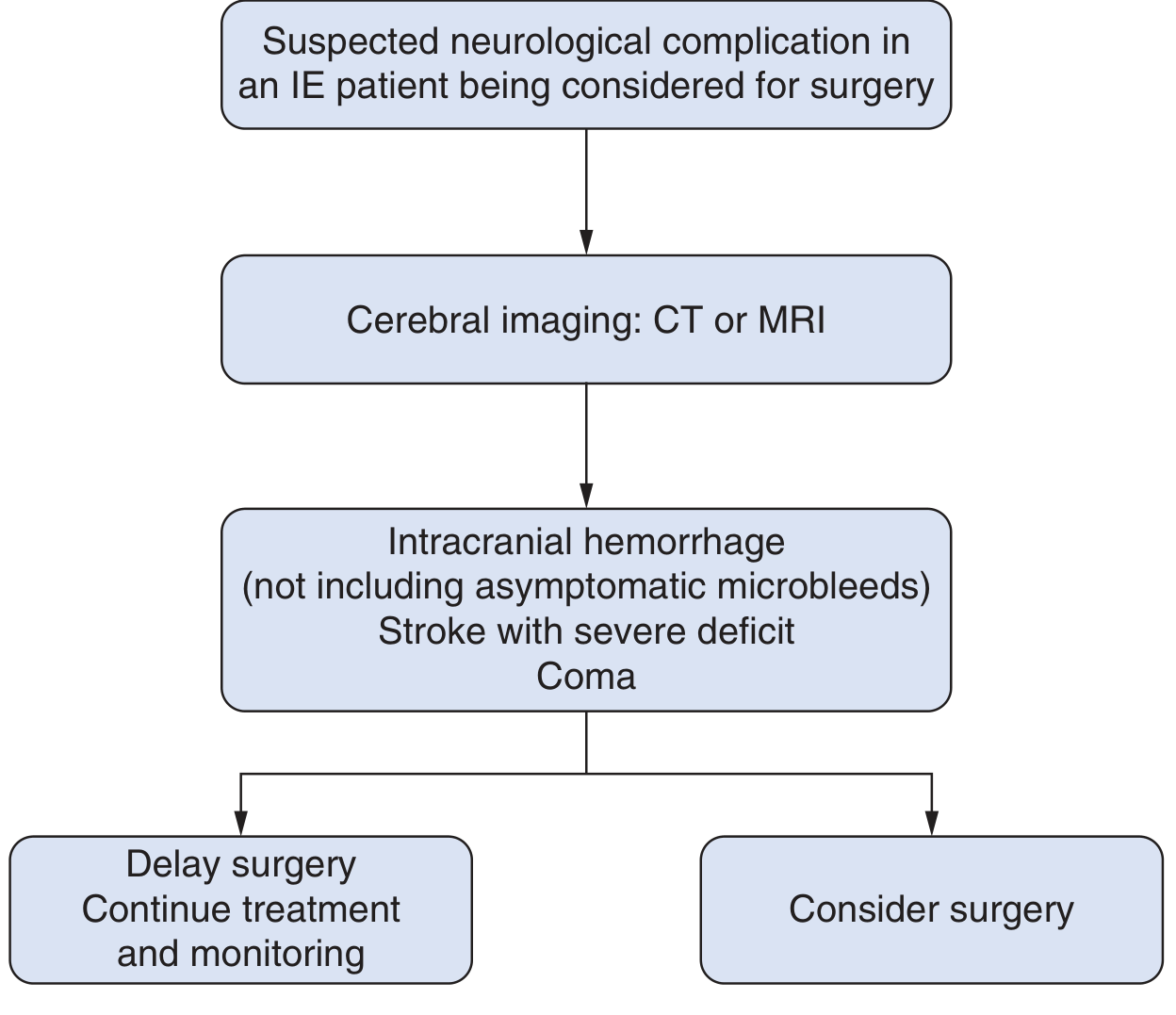
Summary Algorithm
Suspected AIS
↓
NCCT (immediate) → Hemorrhage? → YES → Treat hemorrhagic stroke
↓ NO
ASPECTS score + CTA
↓
LVO identified?
├─ YES → IV tPA (if eligible, no contraindications) + Thrombectomy
│ ↑ 0-24h depending on mismatch imaging
└─ NO → IV tPA alone (if <4.5h, or 4.5-9h with CTP mismatch)
Aspirin 300mg if no tPA/thrombectomy
↓
Supportive care: BP, glucose, temp, O2
Early rehab: physio, OT, speech therapy
Secondary prevention: antiplatelet/anticoagulant, statin, risk factor control
Sources: Bradley and Daroff's Neurology in Clinical Practice; Fuster and Hurst's The Heart 15th Ed.; Canadian Stroke Best Practices 2024; AHA/ASA Guidelines; PMC: Current state of imaging in acute ischemic stroke 2025; DAWN trial (Nogueira et al. 2018); DEFUSE-3; HERMES meta-analysis; ESO 2025 BP guidelines (PMID 42095756)