Describe abg and how it's done ✅
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
arterial blood gas radial artery puncture technique
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Arterial Blood Gas (ABG)
What Is an ABG?
An arterial blood gas (ABG) is a blood test that directly measures the partial pressures of oxygen (PaO₂) and carbon dioxide (PaCO₂), serum pH, and calculated bicarbonate (HCO₃⁻) from an arterial blood sample. It is the gold standard for assessing oxygenation, ventilation, and acid-base status — information that cannot be fully obtained from venous blood or pulse oximetry alone.
"Obtaining a value for arterial PO₂ by analysis of an arterial blood gas is the gold standard for determining oxygenation." — Murray & Nadel's Textbook of Respiratory Medicine
What Does ABG Measure?
| Parameter | Normal Range | What It Reflects |
|---|---|---|
| pH | 7.35 – 7.45 | Acid-base balance |
| PaO₂ | 80 – 100 mmHg | Oxygenation |
| PaCO₂ | 35 – 45 mmHg | Ventilation (CO₂ elimination) |
| HCO₃⁻ | 21 – 27 mEq/L | Metabolic (renal) acid-base component |
| SaO₂ | 95 – 100% | Oxygen saturation of hemoglobin |
Modern ABG analyzers also commonly report lactate, total hemoglobin, and serum electrolytes.
How it works technically:
- The pH electrode measures the potential difference between a reference solution and the sample at 37 °C.
- The PCO₂ electrode allows CO₂ to react chemically, producing H⁺ ions whose concentration generates a measurable voltage.
- HCO₃⁻ is then calculated from the measured pH and PCO₂ using the Henderson-Hasselbalch equation — it is not directly measured.
Why ABG Over Pulse Oximetry?
Pulse oximetry only measures oxygen saturation — not PaO₂, PaCO₂, or pH. Due to the sigmoid oxyhemoglobin dissociation curve, saturation can appear normal (>95%) while PaO₂ is already significantly falling or PaCO₂ is rising dangerously. On supplemental oxygen, pulse oximetry completely loses the ability to detect hypoventilation — a critically important limitation. ABG is also the only way to detect carboxyhemoglobin, methemoglobin, and to calculate the alveolar-arterial (A-a) gradient.
Indications
- Respiratory distress or failure
- Acid-base disorders (metabolic or respiratory)
- Monitoring ventilator settings (ICU)
- Pre-operative assessment in significant lung disease
- Suspected CO poisoning or methemoglobinemia
- Confirm hypoxia or hypercapnia suggested by other monitoring
- Guide weaning from mechanical ventilation
How It's Done (Procedure)
Site Selection
The radial artery is the preferred site because:
- Superficial and easy to palpate
- No adjacent vein or major nerve at risk of injury
- Excellent collateral circulation from the ulnar artery
Order of preference: Radial → Brachial → Femoral
Avoid the femoral artery for routine sampling (hidden bleeding risk); reserve the brachial artery for emergencies (poor collateral circulation; risk of median nerve damage).
Radial Artery Anatomy
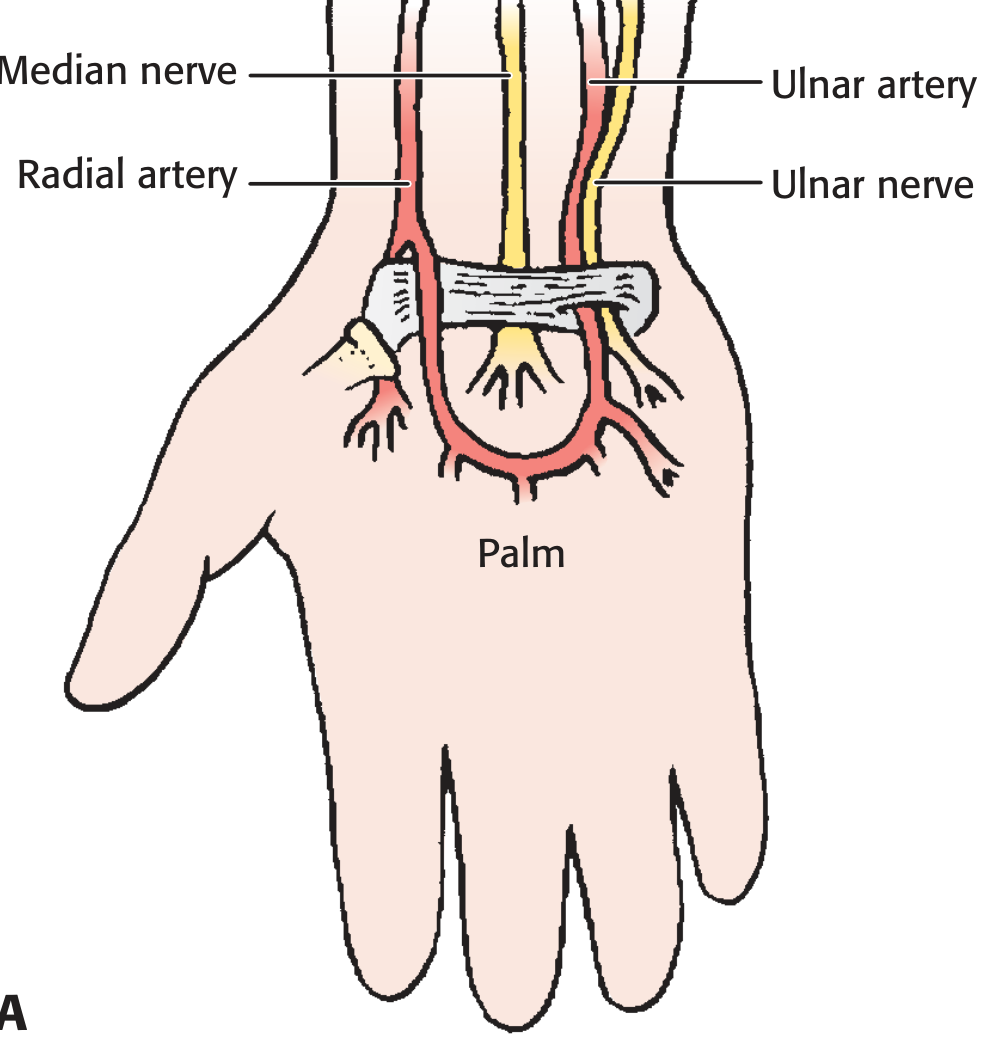
Anatomy of the wrist — the radial artery lies lateral to the flexor carpi radialis tendon, with good collateral flow from the ulnar artery via the palmar arch.
Step-by-Step Technique
1. Modified Allen Test (pre-procedure)
Compress both the radial and ulnar arteries while the patient makes a fist until the hand blanches. Release the ulnar artery — the hand should flush (pink) within 5–15 seconds, confirming adequate collateral circulation. This is mandatory before radial artery puncture.
2. Equipment
- Pre-heparinized ABG syringe (or standard 3 mL syringe flushed with heparin)
- 22–25 gauge needle (23–25 gauge preferred; smaller = fewer complications)
- Antiseptic (chlorhexidine or povidone-iodine + 70% isopropyl alcohol)
- Sterile gloves, gauze
- Crushed ice or ice-water slurry for sample transport
- Optional: 1–2% lidocaine without epinephrine for local anesthesia
Important: Use only a small amount of heparin. Heparin has a very low pH — excess heparin causes falsely abnormal ABG results.
3. Patient Positioning
Place the wrist in slight dorsiflexion (extension) with the arm supinated. Do not over-extend — this can obliterate the pulse.
4. Identify the Artery
Palpate the radial pulse just proximal to the transverse wrist crease, between the radial styloid and the flexor carpi radialis tendon. Mark the site with a fingernail indentation. Clean with antiseptic and allow to dry. Infiltrate lidocaine subdermally if the patient is awake and the situation permits.
5. Puncture
- Insert the needle bevel-up at a 30–45° angle to the skin, directed toward the pulse.
- Apply continuous gentle suction on the plunger while advancing.
- Pulsatile, bright red blood flashback into the hub confirms arterial entry.
- Collect 1–3 mL of blood.
If resistance (bone) is met, withdraw the needle very slowly with continuous suction — the tip may re-enter the arterial lumen on the way out.
6. Post-Procedure
- Remove the needle, immediately expel any air bubbles, and cap the syringe.
- Apply firm pressure for at least 5 minutes (longer in anticoagulated patients) to prevent hematoma.
- Label the sample with patient ID, FiO₂, time, and temperature.
- Transport on ice to the lab immediately (metabolic activity of WBCs continues consuming O₂ at room temperature).
Contraindications
- Infection, burn, trauma, or disturbed anatomy at the intended site
- Absent collateral circulation (failed Allen test)
- AV fistula or shunt in the same limb
- Severe coagulopathy (relative)
Complications
| Complication | Notes |
|---|---|
| Hematoma | Most common; minimized by firm post-procedure pressure |
| Arterial spasm | Usually resolves spontaneously |
| Thrombosis | Risk increases with repeated punctures at same site |
| Infection | Rare with proper aseptic technique |
| Nerve injury | Rare; minimized by correct site selection |
Key Pitfalls That Alter Results
- Air bubbles in the syringe → falsely high PaO₂ / low PaCO₂
- Excess heparin → falsely low pH
- Delay in analysis or failure to ice sample → O₂ consumed by WBCs, CO₂ produced → falsely low PaO₂, high PaCO₂, low pH
- Venous contamination → lower PO₂ and pH
- Patient hyperventilating from pain → falsely normal PCO₂ (use lidocaine to reduce this)
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 437–440; Murray & Nadel's Textbook of Respiratory Medicine; Tintinalli's Emergency Medicine; Henry's Clinical Diagnosis and Management by Laboratory Methods; Pfenninger and Fowler's Procedures for Primary Care.
Define ECG , disease, & change
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have all the content needed for a comprehensive answer. Let me compile it.
Electrocardiogram (ECG)
Definition
An electrocardiogram (ECG) is a recording of the electrical potentials generated by the heart and detected at the surface of the body. When a cardiac impulse passes through the heart, electrical current spreads from the myocardium into surrounding tissues and a small portion reaches the skin surface. Electrodes placed on the skin on opposite sides of the heart detect these potential differences, and the recording is the ECG.
"If electrodes are placed on the skin on opposite sides of the heart, electrical potentials generated by the current can be recorded; the recording is known as an electrocardiogram (ECG)." — Guyton & Hall Textbook of Medical Physiology
Electrocardiography allows simultaneous recording of myocardial activation from multiple vantage points on the body's surface, enabling analysis of electrical activation in different myocardial regions. It was first introduced by Einthoven in the early 1900s and remains largely unchanged in principle today. With AI-assisted interpretation, it is becoming increasingly accurate for certain disease conditions.
Normal Cardiac Activation & ECG Waveforms
The Conduction System (what the ECG reflects)
- SA node (high lateral right atrium) → spontaneous depolarization → spreads across both atria
- → AV node (physiologic conduction delay)
- → Bundle of His → Left & Right Bundle Branches → Purkinje fibers
- → Ventricular muscle depolarization → contraction
Normal ECG Waveforms
| Wave/Interval | What It Represents | Normal Value |
|---|---|---|
| P wave | Atrial depolarization | <120 ms, upright in I, II |
| PR interval | AV nodal conduction delay | 120–200 ms |
| QRS complex | Ventricular depolarization | <120 ms |
| ST segment | Period between ventricular depolarization and repolarization | Isoelectric (at baseline) |
| T wave | Ventricular repolarization | Concordant with QRS |
| QT interval | Total ventricular electrical activity | QTc < 440 ms (men), < 460 ms (women) |
The P wave is a depolarization wave; the T wave is a repolarization wave. The QRS complex is much larger in voltage than the P wave due to the greater ventricular muscle mass.
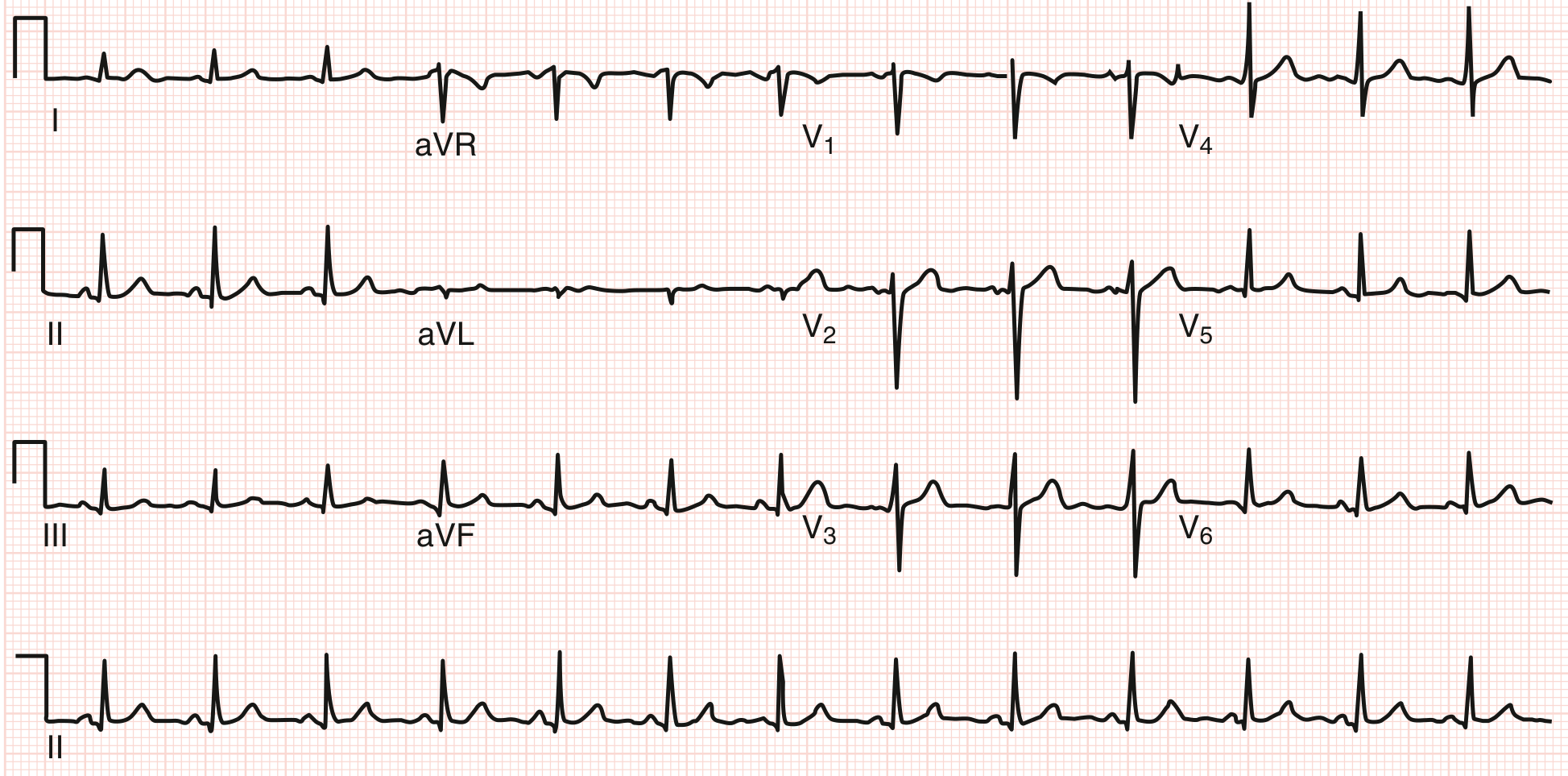
The 12 Leads
A standard ECG uses 12 leads to view the heart from multiple angles:
- Limb leads (I, II, III): Bipolar; measure differences between limb electrodes
- Augmented limb leads (aVR, aVL, aVF): Unipolar; compare each limb to a combined reference
- Precordial leads (V1–V6): Unipolar chest leads; define activation across the transverse plane
Normal orientation: P waves and QRS are positive in I, II, III, aVF; negative in aVR. In the precordial leads, QRS transitions from predominantly negative (V1) to positive (V5–V6), with the transition point normally at V3–V4.
Normal frontal axis: −30° to +90°
Systematic Approach to ECG Interpretation
- Heart rate (normal 60–100 bpm)
- Rhythm: regular vs. irregular; identify P waves
- P-QRS relationship
- Intervals: PR, QRS duration, QT/QTc
- QRS axis
- P wave morphology and axis
- QRS progression in precordial leads (transition point)
- ST segments (regional groupings)
- T waves (regional groupings)
ECG Changes in Disease
1. Myocardial Ischemia / Infarction (ACS)
| Phase | ECG Change |
|---|---|
| Hyperacute (first minutes) | Tall peaked "hyperacute" T waves |
| STEMI (complete occlusion) | ST elevation ≥1 mm in ≥2 contiguous leads + reciprocal ST depression |
| Evolving MI | ST elevation → T wave inversion → Q wave formation (pathological Q = ≥0.04 s wide, >1/4 R height) |
| NSTEMI / UA (partial occlusion) | ST depression ± T wave inversion; no ST elevation |
| Posterior MI | ST depression V1–V3 (mirror image); tall R in V1 |
"If the involved coronary artery is totally occluded by a fresh thrombus, the patient's ECG reveals ST segment elevation… If the coronary artery is partially occluded, the ECG does not show ST segment elevation." — Goldman-Cecil Medicine
Localizing the infarct territory:
| Leads with changes | Territory | Artery |
|---|---|---|
| II, III, aVF | Inferior | RCA |
| V1–V4 | Anterior/Septal | LAD |
| I, aVL, V5–V6 | Lateral | LCx |
| V4R (right-sided) | Right ventricle | RCA proximal |
2. Conduction Abnormalities / Bundle Branch Blocks
| Block | QRS Duration | Key Features |
|---|---|---|
| RBBB | ≥120 ms | rSR' ("rabbit ears") in V1; wide S in I, V6 |
| LBBB | ≥120 ms | Broad notched R in V5/V6/I; no septal q; discordant ST-T changes throughout |
| LAFB | <120 ms | Left axis deviation −45° to −90°; qR in aVL |
| LPFB | <120 ms | Right axis +90° to +180°; rS in I, qR in III |
| 1st degree AV block | Normal | PR >200 ms |
| 2nd degree AV block (Mobitz I) | Normal | Progressive PR lengthening → dropped QRS (Wenckebach) |
| 2nd degree AV block (Mobitz II) | Often wide | Fixed PR, sudden dropped QRS — risk of complete block |
| 3rd degree AV block | Wide (escape) | No relationship between P waves and QRS |
3. Arrhythmias
| Condition | ECG Findings |
|---|---|
| Atrial fibrillation | Irregularly irregular RR; absent P waves; fibrillatory baseline |
| Atrial flutter | Regular "sawtooth" flutter waves at ~300 bpm; typically 2:1 or 4:1 block |
| SVT (AVNRT) | Narrow QRS tachycardia, 150–250 bpm; P waves hidden in or just after QRS |
| WPW syndrome | Short PR <120 ms; delta wave (slurred QRS onset); wide QRS |
| VT | Wide QRS tachycardia (≥120 ms); AV dissociation; fusion beats |
| VF | Chaotic disorganized activity; no recognizable QRS |
4. Chamber Hypertrophy
| Condition | ECG Findings |
|---|---|
| Left ventricular hypertrophy (LVH) | Deep S in V1–V2 + tall R in V5–V6 (Sokolow: >35 mm; Cornell: S in V3 + R in aVL >28 mm men, >20 mm women); repolarization changes (ST depression, T inversion) in lateral leads |
| Right ventricular hypertrophy (RVH) | Right axis deviation; tall R in V1; deep S in V5–V6 |
| Left atrial enlargement (LAE) | Broad notched P ("P mitrale") in II; biphasic P in V1 with wide negative terminal component |
| Right atrial enlargement (RAE) | Tall, peaked P >2.5 mm in II ("P pulmonale") |
5. Pericarditis
- Stage 1: Diffuse concave ST elevation in most leads except aVR and V1 (where there is ST depression); PR depression
- Stage 2–4: ST normalizes → T wave inversion → resolution
- Key distinction from MI: diffuse (not regional), concave shape, PR depression, no reciprocal changes in the usual pattern
6. Electrolyte & Metabolic Changes
| Condition | ECG Change |
|---|---|
| Hyperkalemia | Peaked narrow T waves → PR prolongation → wide QRS → sine wave pattern → VF/asystole |
| Hypokalemia | Flattened T waves, prominent U waves, ST depression, QT prolongation |
| Hypercalcemia | Short QT interval |
| Hypocalcemia | Long QT interval |
| Digoxin effect | "Reverse tick" ST depression (sagging); T wave flattening/inversion; short QT |
| Digoxin toxicity | Arrhythmias (especially PAT with block, VT) |
| Hypothermia | Osborn (J) waves (positive deflection at J point); bradycardia; QT prolongation |
7. Other Conditions
| Condition | ECG Change |
|---|---|
| Pulmonary embolism | Sinus tachycardia (most common); S1Q3T3 pattern; new RBBB; T inversion V1–V4 |
| COPD/Pulmonary hypertension | Right axis deviation; RVH; low voltage; P pulmonale |
| Pericardial effusion/tamponade | Low voltage QRS; electrical alternans (alternating QRS axis) |
| Long QT syndrome | QTc >440–460 ms; risk of torsades de pointes |
| Early repolarization | ST elevation in lateral/inferior leads; more common in young athletes; benign variant but slightly elevated risk of idiopathic VF |
Sources: Goldman-Cecil Medicine, Ch. 42 (Electrocardiography); Guyton & Hall Textbook of Medical Physiology, Ch. 11; Braunwald's Heart Disease; Murray & Nadel's Textbook of Respiratory Medicine; Roberts and Hedges' Clinical Procedures in Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.