what is diffrence between cerebral amyloid angiopathy and acerebral amyloid angipathy related inflamation /
Reading File
Finding Sources
Searching PubMed
"cerebral amyloid angiopathy" AND "CAA-related inflammation"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to provide a thorough, well-structured answer. Here is the complete comparison:
Cerebral Amyloid Angiopathy (CAA) vs. CAA-Related Inflammation (CAA-ri)
These two conditions share the same underlying substrate - beta-amyloid deposition in vessel walls - but differ fundamentally in pathophysiology, clinical presentation, MRI findings, and treatment.
1. Shared Pathological Basis
Both conditions arise from deposition of beta-amyloid (Aβ) in the media and adventitia of small and medium-sized cortical and leptomeningeal arteries. CAA-ri (also called amyloid beta-related angiitis, or ABRA) is best understood as an inflammatory response mounted against this vascular amyloid, rather than a separate disease.
2. Cerebral Amyloid Angiopathy (CAA)
Pathophysiology
- Amyloid deposits in vessel walls cause luminal narrowing, fibrinoid necrosis, and microaneurysm formation
- Vessel wall weakening and microaneurysm rupture lead to hemorrhage
- The mechanism is primarily structural/vascular, not inflammatory
Age and Demographics
- Rare before age 55; prevalence rises steeply with age (up to 60% in unselected autopsies >90 years)
- Associated with Alzheimer disease histopathology in ~50% of cases; clinical dementia in 10-30%
Clinical Presentation
- Lobar intracerebral hemorrhage (ICH) - often multiple, recurrent, in normotensive elderly patients
- Transient focal neurological episodes (TFNEs) / "amyloid spells" - caused by cortical spreading depression from convexal subarachnoid hemorrhage or superficial siderosis
- Cognitive decline - gradual, progressive
- Seizures are less prominent as a presenting feature
MRI Findings
- Multiple lobar cerebral microbleeds (CMBs) on gradient echo or SWI
- Cortical superficial siderosis (hemosiderin deposits along cortical surface)
- Convexal subarachnoid hemorrhage
- White matter hyperintensities (T2/FLAIR) from ischemic small vessel disease
- Findings tend to be bilateral and relatively symmetric
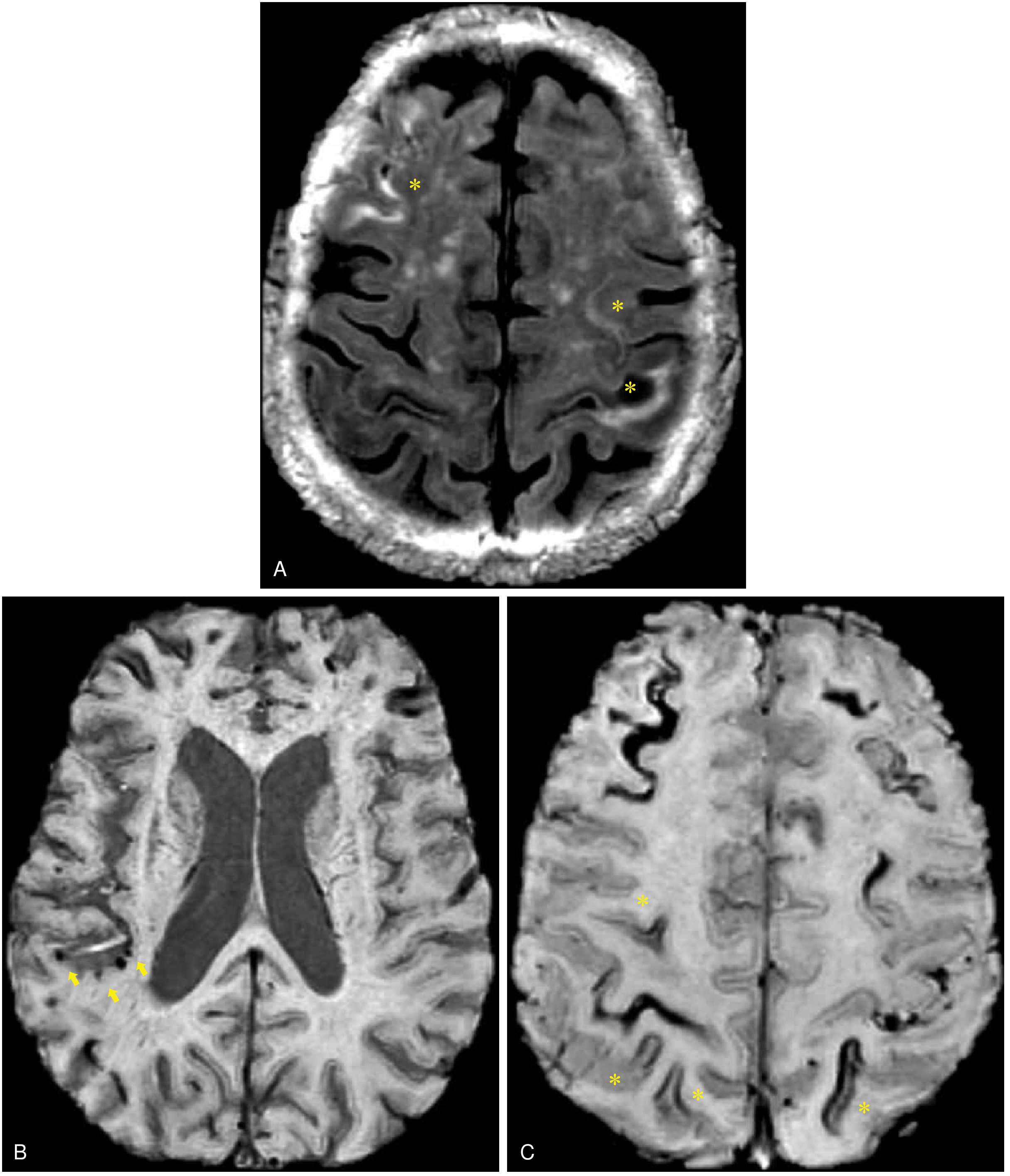
Fig. 66.6 - Bradley and Daroff's Neurology in Clinical Practice: FLAIR (A) bihemispheric convexal subarachnoid hemorrhage; SWI (B) cortical microbleeds; SWI (C) cortical superficial siderosis - a classic CAA constellation.
Diagnostic Criteria
The Modified Boston Criteria (Table 66.1) grade certainty as: Definitive (autopsy), Probable with pathology (tissue biopsy), Probable (clinical + MRI), or Possible (clinical + MRI). Key MRI criteria include age ≥55 and multiple lobar/cortical hemorrhages or superficial siderosis.
Treatment
- No specific disease-modifying therapy for CAA itself
- Avoid anticoagulants (high hemorrhage risk); antiplatelet decisions are individualized
- ICH managed supportively
- TFNEs: trial of topiramate, valproate, or gabapentin (targeting cortical spreading depression), tapered after 1-3 months
- ICH recurrence rate: 5-10% per year (vs. ~2%/year for hypertensive deep ICH)
3. CAA-Related Inflammation (CAA-ri)
Pathophysiology
- CAA-ri represents an immune-mediated inflammatory response directed against vascular amyloid deposits
- Two histological subtypes:
- Perivascular inflammation - lymphocytic infiltration around vessels (more common, better prognosis)
- Transmural granulomatous angiitis (ABRA) - granulomatous inflammation through the vessel wall (more aggressive)
- The inflammation causes vasogenic edema, white matter injury, and blood-brain barrier disruption
Age and Demographics
- Age ≥40 years (notably younger cutoff than CAA, which typically manifests after 55)
- Rare overall; considered a rare manifestation of CAA
Clinical Presentation (rapid onset - the key distinguishing feature)
- Subacute/acute onset of:
- New headaches
- Seizures (prominent)
- Rapid cognitive decline or dementia
- Behavioral changes
- Focal neurological deficits
- The rapid, subacute course contrasts with the more chronic, slowly progressive course of pure CAA
- Symptoms are not directly attributable to an acute ICH
MRI Findings (key distinguishing feature)
- Asymmetric subcortical white matter hyperintensities (FLAIR/T2) - often unilateral or markedly asymmetric
- White matter changes extend to U-fibers (immediately subcortical white matter), reflecting vasogenic edema
- Multiple cortico-subcortical hemorrhagic lesions still present (CMBs, macrobleeds, cortical superficial siderosis) - reflecting underlying CAA
- Contrast enhancement of white matter lesions may be seen (reflects inflammation and BBB breakdown)
- The combination of asymmetric edematous WMH + hemorrhagic CAA markers is the diagnostic hallmark
Diagnostic Criteria (Table 66.2 - Auriel et al., 2016)
| Level | Key Requirements |
|---|---|
| Probable CAA-ri | Age ≥40 + ≥1 clinical feature (headache, cognitive change, focal deficits, seizures) + asymmetric WMH extending to U-fibers on MRI + ≥1 hemorrhagic lesion (macrobleed, CMB, or cortical superficial siderosis) + no other cause |
| Possible CAA-ri | Same but biopsy not required; one criterion relaxed |
| Definitive | Tissue biopsy confirming perivascular or transmural inflammation with amyloid-laden vessels |
Note: A biopsy is NOT required for probable CAA-ri if the clinical + MRI picture is convincing.
Treatment - and this is the most clinically important difference
- Immunosuppressive therapy is the mainstay - CAA itself does NOT respond to and does NOT require immunosuppression
- First line: IV methylprednisolone 1 g/day for 3-5 days, followed by oral prednisone with a taper over months
- Refractory cases: add cyclophosphamide, azathioprine, or mycophenolate mofetil
- Clinical and radiographic findings are often completely reversible with treatment - this reversibility strongly supports the diagnosis
- Most cases are monophasic, but relapses occur in up to one-third of patients (Kinnecom et al., 2007) - requiring long-term maintenance immunosuppression
4. Side-by-Side Comparison Table
| Feature | CAA | CAA-ri |
|---|---|---|
| Core pathology | Structural amyloid vessel wall damage | Immune-mediated inflammation against vascular amyloid |
| Age of onset | Typically >55, common >70 | ≥40 years |
| Onset speed | Chronic, gradual | Subacute to acute |
| Dominant symptoms | Lobar ICH, transient focal episodes, gradual dementia | Headache, seizures, rapid cognitive decline, focal deficits |
| White matter on MRI | Bilateral symmetric periventricular/deep WMH | Asymmetric, extends to U-fibers (vasogenic edema pattern) |
| Hemorrhagic lesions | Lobar CMBs, superficial siderosis, convexal SAH | Same markers present, but not the primary acute change |
| Enhancement on MRI | Absent | May be present (inflammation) |
| CSF | Usually normal or mildly abnormal | Elevated protein, pleocytosis in some |
| Reversibility | Not reversible; progressive | Often completely reversible with treatment |
| Treatment | Supportive; manage hemorrhage risk | Immunosuppression (corticosteroids +/- steroid-sparing agents) |
| Anticoagulation | Contraindicated | Contraindicated |
| Prognosis | Progressive; 5-10% annual ICH recurrence | Good if treated early; relapse in ~33% |
5. Clinical Pearl
The single most important practical point: if an elderly patient presents with acute/subacute headache, seizures, and rapidly progressive cognitive decline, and MRI shows asymmetric white matter edema extending to U-fibers plus microbleeds - think CAA-ri first, not just CAA. This distinction matters because CAA-ri is treatable with immunosuppression and carries a much better prognosis if recognized early, whereas treating it as pure CAA (doing nothing immunosuppressive) would miss a potentially reversible condition.
Sources:
- Bradley and Daroff's Neurology in Clinical Practice (Chapter 66), pp. 1427-1429
- Recent reviews: Inflammatory CAA - broad clinical spectrum (de Souza & Tasker, 2023, J Clin Neurol); Neuroinflammation in CAA (van den Brink et al., 2024, EBioMedicine); International CAA Association guidelines (Cordonnier et al., 2025)
Find recent research on CAA-ri relapse rates and long-term immunosuppressive strategies
Reading File
Searching PubMed
"CAA-related inflammation" AND relapse
Searching PubMed
"cerebral amyloid angiopathy" AND immunosuppression AND treatment
Searching the Web
CAA-related inflammation relapse rate long-term immunosuppression 2023 2024 2025
Reading Article
PMID: 40721902
Reading Article
PMID: 40281535
Reading Article
PMID: 41066717
Reading Article
PMID: 40426643
Reading Article
PMID: 40791767
Reading Article
PMID: 40149580
Reading Web Page
https://discovery.ucl.ac.uk/id/eprint/10211857/1/cordonnier-…
I now have comprehensive, detailed data from the most current sources. Here is the full synthesized answer:
CAA-ri: Relapse Rates and Long-Term Immunosuppressive Strategies - Recent Evidence (2021-2026)
1. Relapse Rates - What the Data Shows
The most current data comes from the 2025 International CAA Association / World Stroke Organization (WSO) Scientific Statement (Cordonnier et al., 2025 - PMID: 40721902), which synthesizes all available case series:
- 80-88% of patients achieve favorable short-term functional recovery with initial immunosuppressive therapy
- Despite this, relapses occur in 38-40% of patients over 3 years - a substantially higher rate than the older "one-third" figure quoted from Kinnecom et al. (2007) in previous textbooks
- A key finding: abrupt discontinuation of IV corticosteroid pulse therapy carries a hazard ratio of 4.68 (95% CI 1.57-13.93; p=0.006) for relapse compared to a slow oral taper - making the taper strategy critical, not just the initial dose
This is a clinically critical update: the relapse risk is higher than previously recognized, and how you stop steroids matters as much as how you start them.
2. Risk Factors for Relapse
Based on the current evidence base (Seifert et al., 2025 - PMID: 40281535):
| Factor | Effect on Relapse Risk |
|---|---|
| Abrupt steroid discontinuation | HR 4.68 - strongly increases risk |
| Slow oral taper over 3-6 months | Strongly reduces risk |
| More severe baseline CAA radiological burden | Associated with worse prognosis |
| Granulomatous/ABRA histology | More aggressive course vs. perivascular type |
| Iatrogenic CAA (iCAA-ri) | Particularly poor response to steroids, higher mortality |
3. Current Treatment Protocols (2025 Guidelines)
The WSO/International CAA Association 2025 Scientific Statement provides the most up-to-date graded recommendations:
First-Line: Corticosteroids (Strong Recommendation)
Induction:
- IV methylprednisolone 1 g/day for 5 days (some centers use 3 days)
- Alternative: high-dose oral methylprednisolone if IV not feasible
Oral taper regimen (explicitly detailed in the guideline):
- Start at 1 mg/kg/day (max 60 mg; reduced to max 40 mg for patients >70 years)
- Reduce by 5 mg every 1-2 weeks until 10 mg/day is reached
- At 10 mg: perform a repeat MRI before proceeding with the final taper
- Final taper: 1 mg/month (very slow final phase)
- Total taper duration: typically 3-6 months, potentially longer if relapse risk is high
Standard supportive co-prescriptions:
- Blood pressure monitoring
- Gastrointestinal protection (PPI)
- Bone protection (calcium/vitamin D, bisphosphonate)
- Infection prevention (PCP prophylaxis)
- Screening for hypoadrenalism and osteoporosis
Second-Line: Steroid-Sparing Immunosuppressants (Weak Recommendation)
Indicated when:
- Limited response to corticosteroids
- Poor tolerability of steroids (common in elderly)
- Relapse during steroid taper or after discontinuation
- Diagnosis is secure (confirmed CAA-ri)
Agents used (from case reports and expert practice):
| Agent | Evidence |
|---|---|
| Cyclophosphamide | Case reports, clinical improvement; used as most aggressive option |
| Azathioprine | Case reports, clinical improvement; steroid-sparing maintenance |
| Mycophenolate mofetil (MMF) | Case reports, clinical improvement; increasingly favored for long-term maintenance |
| Methotrexate | Case reports |
| Rituximab | Efficacy unknown - guideline states further research required (Weak Rec.) |
| IVIG / plasma exchange | Efficacy unknown - further research required (Weak Rec.) |
The guideline explicitly states that no agent has been tested in controlled trials - all second-line recommendations are based on case reports and expert opinion. Local protocols should guide choice.
4. Monitoring Response to Treatment
The 2025 guidelines specify that response should be monitored with:
- Serial neurological and cognitive examination
- Repeat MRI (particularly at the 10 mg/day steroid taper checkpoint and at treatment completion)
- Blood test monitoring (glucose, blood pressure, bone/adrenal markers)
- Both clinical improvement AND radiological improvement on MRI (reversal of asymmetric WMH) should be used to gauge treatment adequacy
5. An Emerging Subtype: Iatrogenic CAA-ri (iCAA-ri)
A 2025 multicenter observational study (Storti et al. - PMID: 41066717) characterized a distinct aggressive subtype:
- Occurs in patients with prior neurosurgery (mean surgical age 17.2 years; CAA-ri onset 44.7 years later at mean age 61.8)
- Thought to arise from prion-like transmission of Aβ via contaminated cadaveric dura or surgical instruments
- 2 of 6 patients died within months of CAA-ri onset despite immunosuppression - suggesting worse prognosis than spontaneous CAA-ri
- Highlights that not all CAA-ri responds equally to steroids
6. The ARIA Connection - A Paradigm Shift
Both Seifert et al. (2025) and Weidauer & Hattingen (2025 - PMID: 40149580) highlight a major conceptual advance:
Spontaneous CAA-ri is now seen as a human model of iatrogenic ARIA-E (amyloid-related imaging abnormalities - edema type) triggered by anti-amyloid therapies (lecanemab, donanemab, aducanumab). This has two practical implications:
- CSF anti-Aβ autoantibodies are now recognized as highly specific biomarkers for CAA-ri - their measurement may guide diagnosis without biopsy and risk-stratify AD patients before starting amyloid immunotherapy
- PET imaging with 11C-PK11195 (microglial activation tracer) may offer future utility in monitoring neuroinflammatory activity in CAA-ri, though not yet in routine clinical use
7. What Remains Unknown - Key Evidence Gaps
| Gap | Current Status |
|---|---|
| Optimal duration of immunosuppression | No consensus; generally 3-6 months minimum, longer if relapsing |
| When to use second-line vs. first-line only | No objective decision criteria; expert opinion |
| Role of rituximab, IVIG, plasma exchange | Unknown - guideline explicitly calls for research |
| Biomarkers to predict relapse | CSF anti-Aβ autoantibodies promising but not validated prospectively |
| Long-term outcomes beyond 3 years | Data severely limited; further study justified per 2025 guideline |
| Optimal second-line agent (azathioprine vs. MMF vs. cyclophosphamide) | No head-to-head comparisons; case report level only |
Summary of Key Evidence
| Paper | Year | Level | Key Finding |
|---|---|---|---|
| Cordonnier et al. (WSO/ICAAA Scientific Statement) | 2025 | Practice Guideline | Relapse 38-40% at 3 years; abrupt steroid stop HR 4.68 for relapse; taper regimen specified |
| Seifert et al. | 2025 | Review | CAA-ri as autoimmune encephalopathy; CSF anti-Aβ autoantibodies as diagnostic/predictive biomarker; no standardized second-line protocols |
| Storti et al. (iCAA-ri multicenter) | 2025 | Observational | iCAA-ri subset: severe course, poor steroid response, high mortality |
| Wang et al. | 2025 | Retrospective cohort (n=13) | >70% favorable outcome with timely immunotherapy; CSF AD biomarkers abnormal in all |
| Ali et al. | 2025 | Case series | Variable treatment response; early treatment beneficial |
| Weidauer & Hattingen | 2025 | Review | CAA-ri/ARIA-E connection; Boston 2.0 criteria update |
Bottom line: The 38-40% 3-year relapse rate is higher than older estimates. The 2025 international guidelines now explicitly warn against abrupt steroid discontinuation (HR 4.68 for relapse) and mandate a slow, MRI-guided taper. Second-line agents (azathioprine, MMF, cyclophosphamide) have clinical support from case reports but no controlled trials exist - the field urgently needs prospective multicenter cohort data.
This is a shared conversation. Sign in to Orris to start your own chat.