fracture
Asking for Preferences
Reading File
Finding Sources
Searching the Web
fracture types classification orthopedics overview
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
fracture types classification transverse oblique spiral comminuted greenstick
Loading Image
Loading Image
Reading File
I now have thorough content from authoritative textbooks. Here is the comprehensive overview:
Fracture Types & Classification
Fractures are classified along several overlapping axes: temporality, skin integrity, fracture pattern, anatomic location, displacement, and special categories (pediatric, pathologic, stress).
1. By Temporality
| Term | Definition |
|---|---|
| Acute | Sharp, well-defined fracture edges; clear injury mechanism |
| Subacute | Callus formation beginning; blunted edges; weeks old |
| Chronic / Nonunion | ≥6 months; sclerotic bone ends; persistent motion at site |
2. By Skin Integrity
- Closed — fracture does not communicate with the external environment
- Open (compound) — fracture communicates with the outside; graded by the Gustilo-Anderson Classification:
| Grade | Features |
|---|---|
| I | Wound <1 cm, clean, simple transverse or short oblique pattern |
| II | Wound 1–10 cm, moderate soft tissue injury |
| IIIa | Adequate soft tissue coverage despite large wound |
| IIIb | Periosteal stripping, requires local/free flap coverage |
| IIIc | Vascular injury requiring repair |
Note: the definitive Gustilo grade is assigned only in the operating room after full debridement. — Sabiston Textbook of Surgery
3. By Fracture Pattern
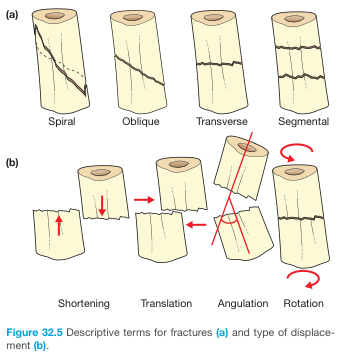
| Pattern | Description | Mechanism |
|---|---|---|
| Transverse | Perpendicular to long axis | Direct blow; 3-point bending |
| Oblique | Angulated across long axis | Angulation force |
| Spiral | Torsional; winds around shaft | Rotational/twisting force |
| Comminuted | >2 fragments | High-energy; axial loading |
| Butterfly | Separate wedge fragment at fracture site | Combined bending + compression |
| Segmental | Two distinct fracture lines isolating a middle segment | High energy |
Pattern also informs stability: oblique and spiral fractures are more prone to displacement than transverse ones.
4. By Anatomic Location
Within a long bone:
- Epiphysis — articular end (between physis and joint surface)
- Metaphysis — between epiphysis and diaphysis; cancellous bone, better vascularized
- Diaphysis (shaft) — dense cortical bone, less vascular → slower healing
- Intraarticular — extends into the joint surface; requires anatomic reduction to prevent post-traumatic arthritis
- Supracondylar / Intercondylar — proximal to or between the condyles
Location along the bone is also described as proximal, middle, or distal third — the basis of the AO/OTA classification.
5. By Displacement
| Type | Description |
|---|---|
| Shortening | Fragments overlap, reducing bone length |
| Translation | Lateral shift of distal fragment |
| Angulation | Angular deformity at fracture site |
| Rotation | Rotational malalignment |
| Impaction | Fragments driven into each other; often appears as a dense (sclerotic) line rather than a lucency (classic in femoral neck fractures) |
6. Special Fracture Categories
Pathologic & Insufficiency Fractures
- Pathologic — through abnormal bone (tumor, infection, Paget disease)
- Insufficiency / Fragility — through osteoporotic bone under normal or minimal load
- Stress fracture — repetitive submaximal loading in normal bone (e.g., metatarsal in runners); vs. insufficiency fracture which occurs in abnormal bone under normal loads
Occult Fractures
Radiographically invisible on plain films; diagnosed by MRI or CT. Divided into:
- Occult-complete — both cortices disrupted but not seen on X-ray
- Trabecular / bone contusion — microtrabecular injury without cortical break
Avulsion Fractures
A ligament or tendon pulls off its bony insertion. Clinically important because they signal ligamentous instability (e.g., Segond fracture = avulsion at lateral tibial plateau → >95% predictive of ACL rupture).
7. Pediatric-Specific Fractures
Children's bones are more plastic, have thicker periosteum, and have open physes — producing injury patterns unique to this age group:
| Type | Description |
|---|---|
| Plastic deformation | Bone angulates without a visible fracture line; cortex does not break |
| Torus (buckle) | Axial load buckles the cortex; one-sided |
| Greenstick | Incomplete cortical disruption + plastic deformation on opposite side |
| Physeal (Salter-Harris) | Involves the growth plate; risk of growth disturbance |
Salter-Harris Classification (physeal fractures):
| Type | Pattern | Risk of growth disturbance |
|---|---|---|
| I | Through physis only | Low |
| II | Through physis + metaphysis (most common) | Low |
| III | Through physis + epiphysis (intraarticular) | Moderate |
| IV | Through metaphysis + physis + epiphysis | High |
| V | Crush of physis | High |
8. Universal Classification: AO/OTA System
The AO/OTA (Arbeitsgemeinschaft für Osteosynthesefragen / Orthopedic Trauma Association) system provides a unified alphanumeric classification for the entire skeleton:
- Bone identified by number (e.g., 3 = femur)
- Segment (1 = proximal, 2 = diaphysis, 3 = distal)
- Type A = simple (single fracture line); B = wedge/butterfly; C = complex/comminuted
- Further subgroups grade severity and comminution
This system facilitates research, communication, and surgical planning across institutions.
Sources:
- Sabiston Textbook of Surgery, pp. 760–762
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 442
- Grainger & Allison's Diagnostic Radiology, pp. 1137–1138
- Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.