Airway breathing circuits and clinical importants
Reading File
Finding Sources
Finding Sources
Searching the Web
airway breathing circuits anaesthesia clinical importance types
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Now I have comprehensive material from two major anesthesiology textbooks. Let me compile the complete answer.
Airway Breathing Circuits — Comprehensive Clinical Overview
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e
What Is a Breathing Circuit?
A breathing circuit connects the patient's airway to the anesthesia machine. Its core functions are to:
- Deliver oxygen and anesthetic gases to the patient
- Eliminate CO₂
- Serve as a low-resistance conduit with a reservoir to meet peak inspiratory flow demand
"Breathing systems provide the final conduit for the delivery of anesthetic gases to the patient." — Morgan & Mikhail, p.78
Classification of Breathing Systems
| Feature | Insufflation / Open-Drop | Mapleson | Circle |
|---|---|---|---|
| Complexity | Very simple | Simple | Complex |
| Control of anesthetic depth | Poor | Variable | Good |
| Scavenging ability | Very poor | Variable | Good |
| Heat & humidity conservation | No | No | Yes |
| Rebreathing of exhaled gases | No | No* | Yes* |
Depends on fresh gas flow rate
1. Insufflation
Anesthetic gases are blown across the patient's face without direct airway connection. Mainly used for inhalation induction in children who resist masks, and to prevent CO₂ accumulation under head drapes (flow >10 L/min of air).
Limitations: Cannot control ventilation; FiO₂ is unpredictable due to entrained room air.
2. Draw-Over Anesthesia
The patient's own inspiratory effort draws ambient air through a low-resistance vaporizer. Used where compressed gases are unavailable (e.g., battlefield, remote settings).
- Can be fitted with IPPV, CPAP, and PEEP capability
- O₂ supplement of 1 L/min gives FiO₂ ~30–40%; 4 L/min gives ~60–80%
- Greatest advantage: simplicity and portability
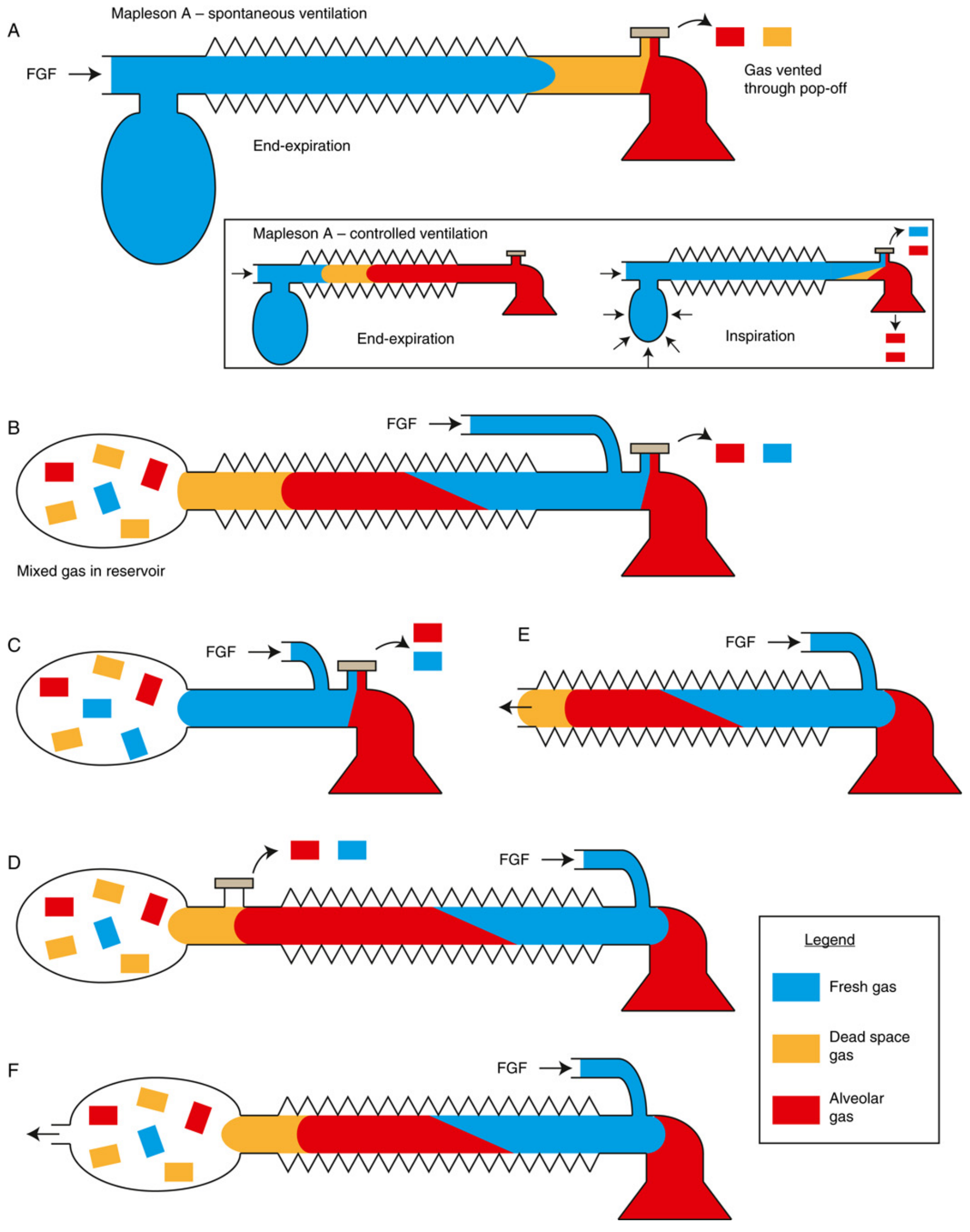
3. Mapleson Circuits (A–F)
Semi-open systems — no CO₂ absorber; CO₂ elimination depends on fresh gas washout. Components: fresh gas inlet, reservoir tubing, reservoir bag, expiratory APL (adjustable pressure-limiting) valve.
Mapleson Classification & FGF Requirements
| Circuit | Also Known As | Best For | FGF (Spontaneous) | FGF (Controlled) |
|---|---|---|---|---|
| A | Magill Circuit | Spontaneous ventilation | = Minute ventilation (~70 mL/kg/min) | 3× minute ventilation |
| B | — | Rarely used | 2× MV | 2× MV |
| C | Waters to-and-fro | Short procedures, ICU | 2× MV | 2× MV |
| D | — | Controlled ventilation | 3× MV | 1–2× MV |
| D (Bain) | Bain Circuit | Controlled ventilation | High FGF | 70 mL/kg/min |
| E | Ayre's T-piece | Pediatrics, spontaneous | 2.5–3× MV | — |
| F | Jackson–Rees | Pediatrics, controlled | 2–3× MV | 2–3× MV |
Key rule: Mapleson A = best for spontaneous breathing; Mapleson D/Bain = best for controlled ventilation. Swapping APL valve and FGF inlet positions converts an A into a D.
Clinical Importance of Mapleson Circuits
- Used for patient transport, ICU ventilation, procedural sedation, and preoxygenation outside the OR
- Bain circuit (coaxial Mapleson D): inner tube carries FGF inside outer expiratory tube — must check inner tube patency (Pethick test), because kinking of inner tube causes hypercapnia
- Mapleson E/F (T-piece): ideal in infants/neonates as no valves = minimal resistance; Jackson–Rees allows IPPV in pediatrics
- Disadvantage: High FGF requirements waste anesthetic agent, pollute OR, and lose patient heat and humidity
4. The Circle System
The most common system used in modern anesthesia. Uses unidirectional valves and a CO₂ absorber to allow rebreathing of exhaled gases safely.
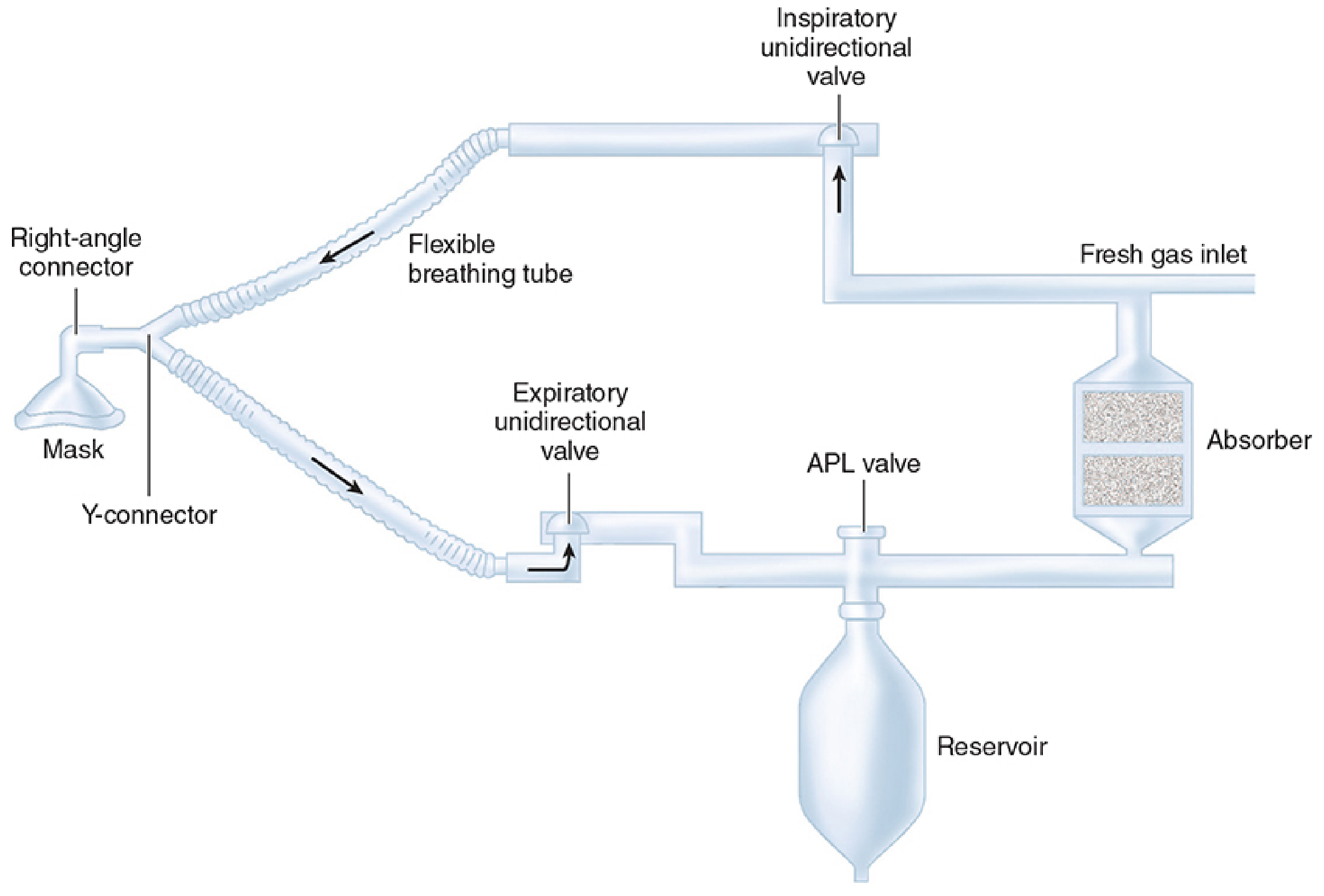
Components (7 Essential)
- CO₂ absorber (soda lime or calcium hydroxide lime)
- Fresh gas inlet
- Inspiratory unidirectional valve + inspiratory tube
- Y-connector (patient end)
- Expiratory unidirectional valve + expiratory tube
- APL (pop-off) valve
- Reservoir bag (1–3 L in adults)
CO₂ Absorption Chemistry (Soda Lime)
CO₂ + H₂O → H₂CO₃
H₂CO₃ + 2NaOH → Na₂CO₃ + 2H₂O + Heat
Na₂CO₃ + Ca(OH)₂ → CaCO₃ + 2NaOH
Soda lime (80% Ca(OH)₂) absorbs up to 23 L CO₂ per 100 g. A pH indicator dye changes color when exhausted.
Advantages of Circle System
- Stable inspired gas concentrations
- Conservation of anesthetic gases (economic)
- Conservation of respiratory heat and moisture
- Effective CO₂ elimination
- Prevention of OR pollution
Clinical Importance — Fresh Gas Flow Modes
| Mode | FGF | Features |
|---|---|---|
| High flow (>4 L/min) | Used at induction/emergence | Rapid control of anesthetic concentration, less rebreathing |
| Semi-closed (1–4 L/min) | Routine maintenance | Some rebreathing; waste gas vented via APL valve |
| Low-flow (<1 L/min) | Experienced practitioners | ≥50% gas rebreathing; reduced agent use, better humidification |
| Minimal-flow (≤0.5 L/min) | Specialized use | Maximum conservation; risk of CO accumulation, compound A |
| Closed | O₂ inflow = patient O₂ uptake | No venting; difficult to manage |
Disadvantages
- Greater size and less portable than Mapleson
- Complex → greater risk of disconnection or malfunction
- Unpredictable inspired concentrations at low FGF
- Absorbent complications: compound A (sevoflurane + dry absorbent), CO production (desflurane/enflurane + desiccated absorbent)
5. Resuscitation Systems (AMBU Bag / BVM)
A bag-valve-mask unit — contains a non-rebreathing valve (unlike Mapleson or circle systems). The patient valve vents exhaled gas to atmosphere through exhalation ports, preventing rebreathing.
- Delivers near 100% O₂ when reservoir attached
- FiO₂ ∝ O₂ flow rate; inversely ∝ minute ventilation
- Used for emergency ventilation, pre-oxygenation, and transport
- Risk: exhaled moisture can cause valve sticking; expired gas contaminates local environment
Safety Monitoring in Breathing Circuits
| Monitor | Purpose | Clinical Threshold |
|---|---|---|
| Oxygen analyzer | Detect hypoxic gas delivery | Alarm ≤18% FiO₂; last line of defense |
| Spirometer/respirometer | Measure exhaled tidal volume | Disconnection/leak detection |
| Pressure sensor | Continuous airway pressure | Alarm at high pressure, -10 cmH₂O, or 20-sec loss of pressure |
| CO₂ monitoring (capnography) | Rebreathing / circuit integrity | Detects esophageal intubation, disconnection |
| Flow sensors | Tidal and minute volume | Heated wire, ultrasonic, or differential pressure types |
Key Clinical Pearls
| Scenario | Circuit Choice | Reason |
|---|---|---|
| Adult spontaneous ventilation | Mapleson A or Circle | Mapleson A most efficient; Circle conserves heat |
| Adult controlled ventilation | Circle (low-flow) or Mapleson D/Bain | Bain efficient at 70 mL/kg/min FGF |
| Pediatric/neonatal anesthesia | Jackson–Rees (F) or Ayre's T-piece (E) | No valves = minimal resistance |
| Remote/battlefield anesthesia | Draw-over system | No compressed gas needed |
| Emergency ventilation | BVM (bag-valve-mask) | Simple, portable, high FiO₂ |
| OR head/neck surgery (local) | Insufflation | Avoids mask; prevents CO₂ accumulation under drapes |
| ICU transport | Mapleson C or D | Portable, simple |
Oxygen Flush Valve — Important Hazard
The oxygen flush valve delivers 35–75 L/min of O₂ directly to the breathing circuit at line pressure (45–55 psig), bypassing flowmeters and vaporizers.
⚠️ Clinical danger: Can cause barotrauma when patient is connected; may backflow into the low-pressure circuit and dilute inhaled anesthetic concentration. A protective rim limits unintentional activation.
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 78–100; Miller's Anesthesia, 10e, pp. 2318–2365
This is a shared conversation. Sign in to Orris to start your own chat.