
inbound3793860350324885817.jpg
Tell me diagnosis and treatment protocol
Reading File
Finding Sources
Searching PubMed
"atrial fibrillation"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Searching PubMed
"atrial fibrillation" AND "guideline"
Reading File
Searching Images
atrial fibrillation ECG no P waves irregularly irregular
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data. Here is the complete answer.
ECG Diagnosis: Atrial Fibrillation (AF)
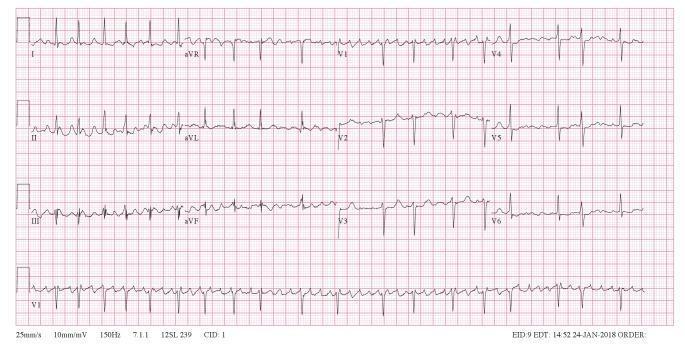
ECG Features (P-Wave Analysis)
| Feature | Finding |
|---|---|
| P waves | Absent — replaced by rapid, chaotic fibrillatory (f) waves at 300–600 impulses/min |
| Baseline | Irregularly undulating (coarse or fine f-waves, best seen in leads II, III, aVF, and V1) |
| Ventricular rhythm | Irregularly irregular — hallmark of AF |
| QRS complexes | Narrow (normal ventricular conduction via AV node) unless aberrancy or BBB coexists |
| Ventricular rate | Typically 100–150 bpm in uncontrolled AF; can exceed 200 bpm if accessory pathway present |
The video asks you to "comment on P wave" — the answer is: P waves are absent, replaced by fibrillatory waves due to disorganized atrial electrical activity from multiple micro-reentry circuits.
Classification
- Paroxysmal — self-terminating (<7 days, usually <48 hrs)
- Persistent — requires cardioversion to restore sinus rhythm
- Permanent — no further attempts to restore sinus rhythm planned
Common Causes
- Hypertensive heart disease (most common)
- Ischemic heart disease / cardiomyopathy
- Valvular disease (especially mitral)
- Congestive heart failure
- Hyperthyroidism
- Pulmonary embolism
- Alcohol (holiday heart syndrome)
- Idiopathic / lone AF
Treatment Protocol
Step 1 — Assess Hemodynamic Stability
Hemodynamically unstable (hypotension, pulmonary edema, active ischemia, altered consciousness):
→ Immediate synchronized DC cardioversion (100–200 J biphasic)
Hemodynamically stable → proceed with steps below.
Step 2 — Rate Control (First Priority)
Target resting heart rate ≤110 bpm (lenient) or ≤80 bpm (strict, for symptomatic patients).
| Agent | Route | Notes |
|---|---|---|
| Metoprolol (beta-blocker) | IV/PO | First-line; avoid in decompensated HF |
| Diltiazem (CCB) | IV/PO | Effective and titratable; avoid in HF with reduced EF |
| Verapamil (CCB) | IV/PO | Avoid in HF |
| Digoxin | IV/PO | Useful in HF + AF; slower onset |
| Amiodarone | IV | When other agents fail or in hemodynamic compromise |
⚠️ Do NOT use AV-nodal blockers (beta-blockers, CCBs, digoxin) if pre-excitation / WPW syndrome is suspected (very fast rates >200 bpm, wide QRS) — use procainamide or cardioversion.
Step 3 — Rhythm Control (When Appropriate)
Cardioversion is safe if:
- AF duration ≤48 hours, OR
- Patient already on therapeutic anticoagulation, OR
- TEE shows no left atrial thrombus
If AF >48 hours without anticoagulation → anticoagulate for ≥3 weeks before elective cardioversion, then continue for ≥4 weeks after.
Pharmacologic Cardioversion (Stable AF ≤48 hrs)
| Drug | Dose | Caution |
|---|---|---|
| Ibutilide | 0.015–0.02 mg/kg IV over 10–15 min | Highest conversion rate; avoid in structural/ischemic heart disease |
| Procainamide | 30–50 mg/min IV, up to 18–20 mg/kg | First-line if accessory pathway suspected |
| Amiodarone | 150 mg IV over 10–15 min, then infusion | Safe in structural heart disease |
| Flecainide | 300 mg PO ("pill-in-pocket") | Contraindicated in structural/ischemic heart disease |
| Propafenone | 600 mg PO | Same contraindication as flecainide |
Electrical Cardioversion
- Success rates higher than pharmacologic conversion
- 100–200 J biphasic, synchronized
- Up to 50% of new-onset AF converts spontaneously within 24 hours
Step 4 — Anticoagulation (Stroke Prevention)
Calculate CHA₂DS₂-VASc score:
| Factor | Points |
|---|---|
| CHF | 1 |
| Hypertension | 1 |
| Age ≥75 | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA history | 2 |
| Vascular disease | 1 |
| Age 65–74 | 1 |
| Sex (female) | 1 |
- Score ≥2 (men) or ≥3 (women): Anticoagulation recommended
- Score 1 (men) or 2 (women): Consider anticoagulation
- Score 0 (men): No therapy needed
Anticoagulant Options
| Drug | Notes |
|---|---|
| Apixaban (DOAC) | Preferred — lowest bleeding risk |
| Rivaroxaban / Edoxaban / Dabigatran | DOACs; no INR monitoring needed |
| Warfarin | INR target 2.0–3.0; used in valvular AF (rheumatic MS) — DOACs not validated here |
DOACs are preferred over warfarin for non-valvular AF (similar or better stroke prevention, less bleeding). For rheumatic mitral stenosis + AF, use warfarin (DOACs are not indicated).
Step 5 — Long-term / Maintenance Rhythm Control
- Catheter ablation (pulmonary vein isolation): Preferred for symptomatic paroxysmal AF; superior to antiarrhythmic drugs in HF patients
- Antiarrhythmic drugs for maintaining sinus rhythm:
- Flecainide / Propafenone — no structural heart disease
- Sotalol — with caution (proarrhythmic)
- Amiodarone — most effective; use when others fail (toxicity profile limits long-term use)
- Left atrial appendage closure (e.g., WATCHMAN device): For patients who cannot tolerate anticoagulation
Key Reference
2023 ACC/AHA/ACCP/HRS Guideline for AF Management — Joglar JA et al., Circulation, 2024 (PMID 38033089)
- Rosen's Emergency Medicine, Chapter 65
- Braunwald's Heart Disease, Chapter 66
- Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.