Prophylaxis of migrane kd tripathi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have enough rich content now. Let me compile the comprehensive answer on migraine prophylaxis as covered by KD Tripathi-style pharmacology texts (using Lippincott, Katzung, Bradley & Daroff as authoritative sources).
Prophylaxis of Migraine - KD Tripathi Style
Indications for Prophylaxis
Prophylactic (preventive) therapy is indicated when:
- Attacks occur 2 or more times per month
- Headaches are severe, prolonged, or disabling (impair daily functioning)
- Acute abortive therapy is contraindicated, overused, or ineffective
- Headaches are complicated by serious neurologic signs (hemiplegic migraine, migraine with prolonged aura)
- Menstrual migraine with predictable timing
The goal is to reduce attack frequency, severity, and duration by at least 50%.
Drugs Used in Migraine Prophylaxis
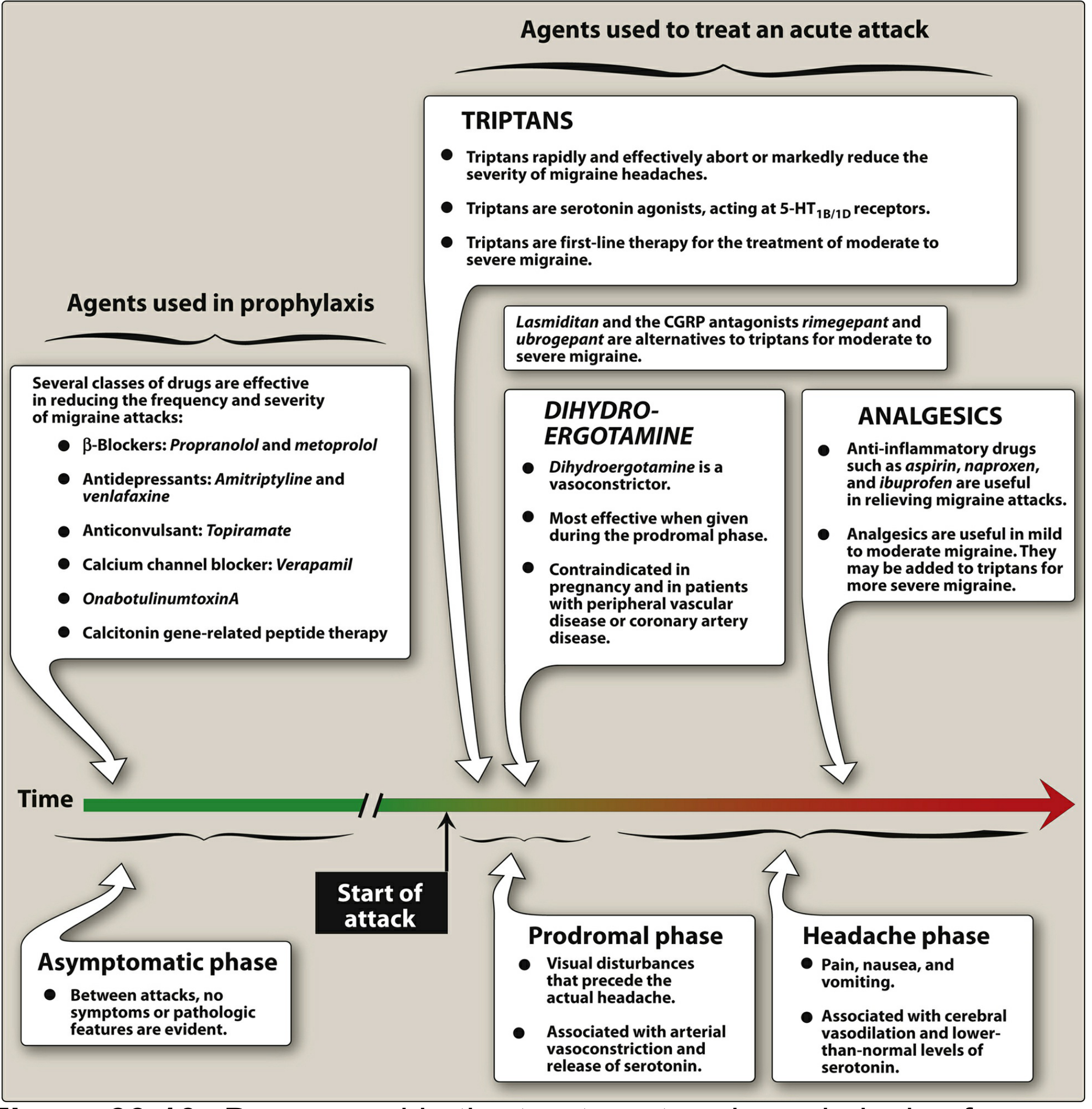
1. Beta-Blockers (Drugs of Choice)
Propranolol and metoprolol are the first-line drugs of choice for migraine prophylaxis.
| Drug | Dose |
|---|---|
| Propranolol | 40-240 mg/day in divided doses |
| Metoprolol | 100-200 mg/day |
| Timolol | 20-40 mg/day (FDA approved) |
| Atenolol | 50-100 mg/day |
| Nadolol | 20-240 mg/day |
Mechanism: Blockade of beta-adrenergic receptors reduces trigeminovascular activation and sympathetic tone. Also modulate serotonergic transmission.
Note: Beta-blockers with intrinsic sympathomimetic activity (ISA) like pindolol are not effective for migraine prophylaxis.
Contraindications: Asthma, COPD, heart block, depression, diabetes (masks hypoglycemia).
2. Antiepileptic Drugs (AEDs)
Valproate / Divalproex Sodium (Sodium Valproate)
- Dose: 500-1750 mg/day in divided doses
- 50% of patients show ≥50% reduction in migraine frequency
- Mechanism: Enhances GABA, reduces cortical hyperexcitability and neurogenic inflammation
- Side effects: Sedation, weight gain, hair loss, tremor, increased liver enzymes, thrombocytopenia, neural tube defects (teratogenic)
- Contraindicated in pregnancy (neural tube defects)
Topiramate
- Dose: 75-200 mg/day (start at 15-25 mg/week, titrate slowly)
- Evidence from large randomized controlled trials
- Mechanism: Blocks Na+ channels, enhances GABA, blocks kainate/AMPA glutamate receptors, inhibits carbonic anhydrase
- Side effects: Cognitive impairment ("dopamax"), paresthesia, weight loss, kidney stones (calcium phosphate)
- Slow titration essential to avoid precipitating depression
Gabapentin
- Dose: 900-2400 mg/day
- Limited evidence; useful when migraine co-exists with neuropathic pain, back pain, or peripheral neuropathy
- Side effects: Dizziness, sedation
3. Tricyclic Antidepressants (TCAs)
Amitriptyline is the most studied and widely used.
- Dose: 10-150 mg at night
- Effective even in patients without depression
- Mechanism: Blocks serotonin and norepinephrine reuptake; also has antihistamine and anticholinergic effects
- Side effects: Sedation, dry mouth, urinary retention, weight gain, cardiac arrhythmias
- Also used: Nortriptyline (better tolerated, fewer anticholinergic effects)
SNRIs: Venlafaxine (75-150 mg/day) is an alternative, particularly in patients with comorbid anxiety/depression.
Note: SSRIs (fluoxetine, sertraline) have limited evidence for migraine prophylaxis.
4. Calcium Channel Blockers
Flunarizine (not available in USA)
- Dose: 5-10 mg at night
- Very effective - reduces both frequency and severity
- Drug of choice in many countries (India, Europe)
- Mechanism: Non-selective calcium channel blocker + dopamine D2 antagonist
- Side effects: Weight gain, sedation, depression, extrapyramidal symptoms (parkinsonism with long-term use)
Verapamil
- Has modest efficacy in migraine prophylaxis
- Particularly useful in migraine with aura and cluster headaches
- Dose: 240-480 mg/day
Note: Nifedipine and amlodipine are less effective.
5. OnabotulinumtoxinA (Botox)
- Approved for chronic migraine (≥15 headache days/month for >3 months)
- Given as 31 fixed-site injections (155 units) into head/neck muscles every 12 weeks
- Mechanism: Inhibits release of CGRP and substance P from peripheral sensory nerve terminals
- Supported by two large multicenter placebo-controlled RCTs (PREEMPT 1 & 2)
6. CGRP-Targeted Therapies (Newer Agents)
Calcitonin gene-related peptide (CGRP) plays a key role in migraine pathophysiology. Blocking CGRP or its receptor is a major advance in migraine prevention.
Anti-CGRP Monoclonal Antibodies
| Drug | Target | Route | Frequency |
|---|---|---|---|
| Erenumab | CGRP receptor | SC | Monthly |
| Galcanezumab | CGRP ligand | SC | Monthly |
| Fremanezumab | CGRP ligand | SC | Monthly or quarterly |
| Eptinezumab | CGRP ligand | IV | Quarterly |
- Reserved for patients inadequately controlled by oral agents
- Very expensive; used as second-line when oral prophylaxis fails
Oral CGRP Receptor Antagonists (Gepants)
- Atogepant and Rimegepant - approved for prevention of migraine
- Administered orally, well tolerated
- Side effects: nausea, somnolence (low incidence)
7. Serotonin Antagonists (Older Agents)
Methysergide (no longer available in USA/Canada)
- Historically very effective; peripheral serotonin antagonist + central agonist
- Serious side effect: retroperitoneal, pulmonary, and cardiac fibrosis (drug holiday every 6 months was mandatory)
Cyproheptadine
- Peripheral serotonin + H1-antihistamine antagonist
- Primarily used in pediatric migraine
- Available as syrup for children who cannot swallow tablets
- Side effects: Drowsiness, significant weight gain
8. Other Agents
| Agent | Dose | Notes |
|---|---|---|
| Riboflavin (B2) | 400 mg/day | Small RCT showed efficacy; minimal side effects; effect takes 3 months |
| Magnesium | 600 mg/day (chelated or slow-release) | Mixed evidence; diarrhea, gastric irritation |
| Butterbur (Petasites) | 150 mg/day | Evidence from clinical trials but potential hepatotoxicity |
| Coenzyme Q10 | 300 mg/day | Some evidence; well tolerated |
| Aspirin/NSAIDs | 325 mg every other day | Modest benefit; especially for menstrual migraine |
Perimenstrual (Cyclic) Prophylaxis for Menstrual Migraine
For women with predictable menstrual migraines, short-course perimenstrual prophylaxis (days -3 to +3 of cycle) can be used:
- NSAIDs: Naproxen sodium 550 mg BD, mefenamic acid 250 mg TDS, ketoprofen 75 mg TDS
- Triptans: Frovatriptan (long t½ of 27 hours - preferred), naratriptan, zolmitriptan
- Ergots: Ergotamine tartrate + caffeine 1 mg qhs
Summary Table - First Line vs Second Line
| Category | Drug | Status |
|---|---|---|
| Beta-blocker | Propranolol, Metoprolol | 1st line (DOC) |
| AED | Topiramate, Valproate | 1st line |
| TCA | Amitriptyline | 1st line |
| Ca2+ channel blocker | Flunarizine, Verapamil | 2nd line |
| SNRI | Venlafaxine | 2nd line |
| Botox | OnabotulinumtoxinA | Chronic migraine only |
| Anti-CGRP mAb | Erenumab, Galcanezumab | Refractory cases |
| Oral gepants | Atogepant, Rimegepant | Newer; preventive use |
Key Points for Exams (KD Tripathi Style)
- Drug of choice for migraine prophylaxis = Propranolol (a non-selective beta-blocker without ISA)
- Valproate is contraindicated in pregnancy - risk of neural tube defects
- Flunarizine causes weight gain + extrapyramidal symptoms (depression, parkinsonism)
- Topiramate causes weight loss - useful in obese patients; but can cause cognitive blunting
- Amitriptyline is effective even in non-depressed migraineurs
- Methysergide can cause fibrosis (retroperitoneal, pulmonary, cardiac) - requires 1-month drug holiday every 6 months
- Cyproheptadine is preferred in children (syrup formulation)
- CGRP monoclonal antibodies are the newest class - given SC monthly; reserved for refractory cases
- Beta-blockers with ISA (pindolol, acebutolol) are NOT effective
- Prophylaxis is considered successful if attack frequency reduces by ≥50%
Sources: Lippincott Illustrated Reviews Pharmacology, p.1324; Katzung's Basic and Clinical Pharmacology, 16th ed., p.456; Bradley and Daroff's Neurology in Clinical Practice, pp.2479-2482
This is a shared conversation. Sign in to Orris to start your own chat.