MI 3.6 - Malaria: Plasmodium species, life cycle, pathogenesis, lab diagnosis, treatment In competency ko mujhe apporba sastry book ke according conceptually samjhao poori detail me concepts and flowchart and pnemonics ke saath
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the key information and both life cycle diagrams. Now let me compose the comprehensive answer in Hindi/English (Hinglish) as requested, covering all aspects of the MI 3.6 competency with Apurba Sastry-style concepts, flowcharts, and mnemonics.
🦟 MI 3.6 - MALARIA: Complete Conceptual Guide
(Apurba Sastry Microbiology Style - Concepts + Flowcharts + Mnemonics)
🔑 TRIGGER WORDS (Exam Alert!)
Quotidian, Tertian, Quartan, Blackwater fever, Cerebral malaria, Benign tertian, Malignant tertian, Multiple ring forms, Gametocytes, Anopheles, Hypnozoites, Schuffner's dots
1. PLASMODIUM SPECIES - Overview
Plasmodia = Coccidian / Sporozoan (Apicomplexa) parasites of RBCs
Two hosts required:
- Definitive host = Mosquito (sexual reproduction)
- Intermediate host = Human (asexual reproduction)
5 Human Species - Mnemonic: "FKVOM"
Falciparum, Knowlesi, Vivax, Ovale, Malariae
| Species | Disease | Fever Periodicity | RBC Preference | Relapse? |
|---|---|---|---|---|
| P. falciparum | Malignant tertian malaria | 48 hrs (quotidian early) | ALL RBCs (any age) | No (no hypnozoites) |
| P. vivax | Benign tertian malaria | 48 hrs | Young RBCs (reticulocytes) | YES (hypnozoites) |
| P. ovale | Benign tertian malaria | 48 hrs | Young RBCs | YES (hypnozoites) |
| P. malariae | Quartan malaria | 72 hrs | Old RBCs | No (recrudescence possible) |
| P. knowlesi | Quotidian malaria | 24 hrs | Old RBCs | No |
Mnemonic for Fever Periodicity: "48-48-48-72-24"
V-O-F = 48 hrs (Tertian) | M = 72 hrs (Quartan) | K = 24 hrs (Quotidian)
2. LIFE CYCLE - Full Detail
DIAGRAM 1: Complete Life Cycle (Murray Medical Microbiology 9e)
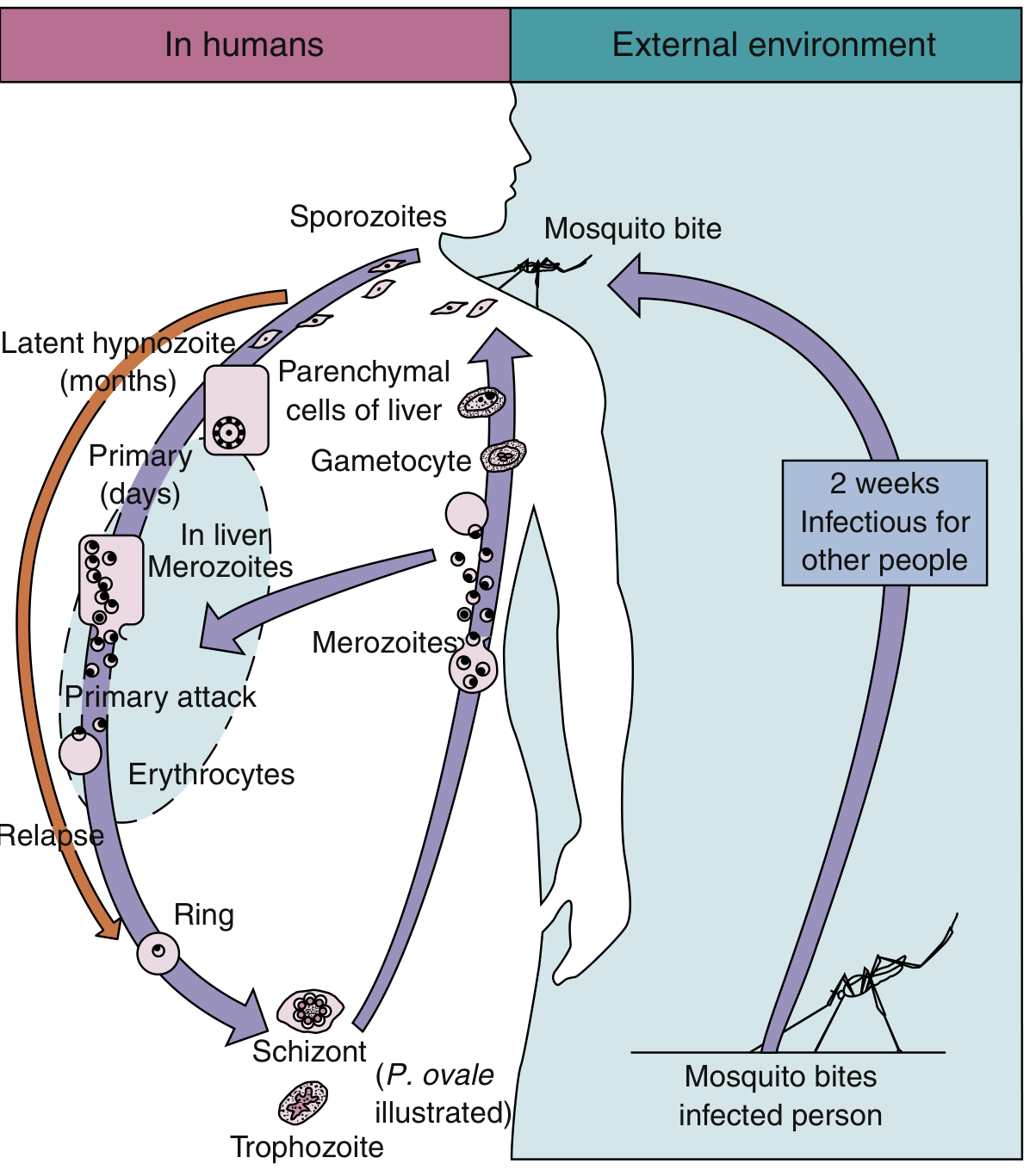
DIAGRAM 2: P. falciparum Molecular Pathogenesis (Robbins Pathology)

LIFE CYCLE FLOWCHART:
MOSQUITO STAGE (Sexual / Sporogonic Cycle)
|
| Female Anopheles bites infected human
| Ingests GAMETOCYTES
|
[In Mosquito Midgut]
Microgametocyte + Macrogametocyte
|
Fertilization → ZYGOTE
|
OOKINETE → OOCYST (in gut wall)
|
SPOROZOITES (in salivary gland)
| ~2 weeks in mosquito
↓
===========================
HUMAN STAGE (Asexual / Schizogonic Cycle)
===========================
STEP 1: MOSQUITO BITE
|
SPOROZOITES injected into human bloodstream
|
↓ (within minutes)
STEP 2: PRE-ERYTHROCYTIC / HEPATIC STAGE (Exoerythrocytic Schizogony)
|
Sporozoites → Travel to LIVER
Bind hepatocytes via:
- Thrombospondin-related adhesive protein (TRAP)
- Circumsporozoite protein (CSP)
→ bind Heparan sulfate proteoglycans on hepatocytes
|
Sporozoites → develop into LIVER SCHIZONTS → MEROZOITES
|
Duration: 5-15 days (depending on species)
|
P. vivax / P. ovale → Some sporozoites become HYPNOZOITES
(dormant, causes RELAPSE months-years later)
|
↓ Hepatocyte ruptures
STEP 3: ERYTHROCYTIC STAGE (Erythrocytic Schizogony)
|
MEROZOITES enter RBCs
(via Lectin-like molecule + Glycophorin/Sialic acid residue)
|
Inside RBC: Merozoite → RING FORM → TROPHOZOITE → SCHIZONT
|
Schizont bursts → releases 6-36 MEROZOITES + malarial pigment (hemozoin)
|
Simultaneous RBC lysis → FEVER PAROXYSM
|
Some merozoites → GAMETOCYTES (sexual forms)
|
↓ Mosquito picks up gametocytes → cycle restarts
Key Terms (Apurba Sastry Style):
- Schizogony = Asexual division in liver/RBC
- Sporogony = Sexual cycle in mosquito
- Hypnozoite = "Sleeping form" in liver (P. vivax, P. ovale only) - causes RELAPSE
- Recrudescence = Reactivation from persistent low-grade erythrocytic infection (P. malariae, P. falciparum) - NO hypnozoites
- Relapse vs Recrudescence: Relapse = from liver (hypnozoites); Recrudescence = from blood stage
3. PATHOGENESIS
A. FEVER PAROXYSM MECHANISM:
RBC Schizonts rupture synchronously
↓
Release: Merozoites + Hemozoin + Malarial toxins (GPI anchor)
↓
Macrophages activated → TNF-α, IL-1, IL-6 release
↓
HYPOTHALAMUS stimulated
↓
FEVER PAROXYSM (classic triad: Cold stage → Hot stage → Sweating stage)
B. COLD/ANEMIA STAGES:
- Cold stage (15-60 min): Intense shivering, temperature rises rapidly
- Hot stage (2-6 hrs): High fever 39-41°C, headache, vomiting
- Sweating stage (2-4 hrs): Profuse sweating, temperature falls → patient exhausted
C. P. FALCIPARUM PATHOGENESIS (Most Dangerous):
P. falciparum infects ALL ages of RBCs
↓
Parasitized RBCs express PfEMP1 (P. falciparum Erythrocyte Membrane Protein-1)
↓
PfEMP1 = KNOB formations on RBC surface
↓
Knobs bind endothelial receptors:
- ICAM-1 (Intercellular adhesion molecule-1)
- VCAM-1 (Vascular cell adhesion molecule-1)
- CD36
↓
CYTOADHERENCE → Parasitized RBCs SEQUESTER in deep capillaries
↓
Microvascular OBSTRUCTION
↓
CEREBRAL MALARIA (brain capillaries)
PLACENTAL MALARIA (placental capillaries)
RENAL FAILURE
D. COMPLICATIONS OF FALCIPARUM MALARIA - Mnemonic: "CRAB-H"
- C - Cerebral malaria (encephalopathy, coma, convulsions)
- R - Renal failure (acute tubular necrosis)
- A - Anemia (severe hemolytic)
- B - Blackwater fever (massive hemolysis → hemoglobinuria → "black" urine)
- H - Hypoglycemia + Hepatic dysfunction + Hyperparasitemia
E. WHY DO OTHER SPECIES PREFER CERTAIN RBCs?
| Species | RBC Preference | Mechanism |
|---|---|---|
| P. vivax | Young RBCs (reticulocytes) | Duffy antigen receptor (DARC) - merozoite binds Duffy Ag |
| P. ovale | Young RBCs | Similar to vivax |
| P. malariae | Old RBCs | Unknown receptor |
| P. falciparum | ALL RBCs | No selectivity → highest parasitemia |
Mnemonic: Africans with Duffy-negative RBCs are resistant to P. vivax (because P. vivax merozoite needs Duffy Ag to enter)
4. MORPHOLOGY / MICROSCOPY FEATURES
Key Distinguishing Features - Mnemonic: "FARMS"
| Feature | P. falciparum | P. vivax | P. ovale | P. malariae |
|---|---|---|---|---|
| RBC size | Normal/small | Enlarged | Enlarged/oval | Normal/small |
| Schuffner's dots | Absent (Maurer's clefts) | Present | Present | Absent |
| Ring forms | Multiple rings/cell, Applique (accolé) forms | Single ring | Single ring | Single ring |
| Banana-shaped gametocytes | YES (crescent/banana) | Round | Round | Round |
| Max merozoites | 24 | 16 | 8 | 8 |
| Schizont appearance | Rarely in peripheral blood | Rosette/Daisy head | Rosette | Rosette "daisy head" |
| Pigment | Black/dark hemozoin | Yellow-brown | Dark brown | Brown |
Mnemonic for Schuffner's Dots:
"VOS" has dots = Vivax + Ovale have Schuffner's dots | Falciparum = NO dots (Maurer's clefts instead)
Mnemonic for Gametocytes:
"Falciparum = Banana/Crescent" - Only one with crescent-shaped gametocyte - exam favorite!
5. EPIDEMIOLOGY
- Vector: Female Anopheles mosquito (bites at dusk/night)
- P. falciparum: Tropical/subtropical only
- P. vivax: Widest distribution (tropics + subtropics + some temperate areas); 80% cases in South America + Southeast Asia
- P. ovale: Primarily tropical Africa
- P. malariae: Same as others, less prevalent
- P. knowlesi: Malaysia, Southeast Asia (zoonotic - from macaque monkeys)
Other Modes of Transmission - Mnemonic: "MINT-C"
- M - Mosquito (main route)
- I - IV drug users (shared needles = "mainline malaria")
- N - Needle stick / Blood transfusion (transfusion malaria)
- T - Transplant (organ)
- C - Congenital (rare)
Note: Transfusion malaria has NO liver stage (no pre-erythrocytic phase), so no hypnozoites, no relapse from liver
6. LABORATORY DIAGNOSIS
FLOWCHART:
SUSPECTED MALARIA
|
↓
1st LINE: PERIPHERAL BLOOD SMEAR
┌─────────────────────────────────┐
│ THICK SMEAR THIN SMEAR │
│ (Screening - (Species │
│ more sensitive) ID - more │
│ specific) │
└─────────────────────────────────┘
|
GIEMSA STAIN / LEISHMAN STAIN
|
Look for: Ring forms, trophozoites,
schizonts, gametocytes, Schuffner's dots
|
↓
2nd LINE: RAPID DIAGNOSTIC TESTS (RDTs)
- Antigen detection (HRP-2 for P. falciparum)
- PfHRP2 (Histidine-rich protein 2) - falciparum specific
- pLDH (Parasite Lactate dehydrogenase) - all species
- Aldolase - pan-malarial antigen
|
↓
OTHER METHODS:
- QBC (Quantitative Buffy Coat) - acridine orange stain, fluorescence
- PCR - gold standard for species ID, drug resistance genes
- Serology (ELISA, IFA) - not for acute diagnosis, epidemiological surveys only
GOLD STANDARD = THICK BLOOD SMEAR + GIEMSA STAIN
When to collect blood?
- During or just after a fever spike - maximum ring forms in peripheral blood at this time
- P. falciparum: Only ring forms + gametocytes in peripheral blood (schizonts sequestered in organs)
- Multiple smears (every 6-12 hrs x 3) if initial negative
RDT Key Points:
| Antigen | Detects | Notes |
|---|---|---|
| HRP-2 | P. falciparum only | Can persist for 2 weeks post-treatment (false positive) |
| pLDH | All species | Clears quickly after treatment |
| Aldolase | All species (pan-malarial) | Less sensitive |
7. TREATMENT
TREATMENT FLOWCHART:
MALARIA CONFIRMED
|
├──── P. falciparum ──────────────────────────────────┐
| │
└──── P. vivax / P. ovale / P. malariae ──────────┐ │
│ │
↓ ↓
NON-FALCIPARUM (vivax/ovale/malariae):
CHLOROQUINE (blood schizonticide)
+ PRIMAQUINE (for vivax/ovale only - kills hypnozoites = prevents relapse)
Check G6PD status before giving PRIMAQUINE (causes hemolysis in G6PD deficiency)
FALCIPARUM - UNCOMPLICATED:
Artemisinin-based Combination Therapy (ACT):
- Artemether + Lumefantrine (Coartem) - 1st line in India
- Artesunate + Amodiaquine
- Artesunate + Mefloquine
- Artesunate + Sulfadoxine-Pyrimethamine (AASP)
NOTE: No primaquine needed (no hypnozoites) except single dose for gametocyte kill
FALCIPARUM - SEVERE / COMPLICATED:
IV Artesunate (drug of choice)
OR IV Quinine + Doxycycline (if artesunate not available)
+ Supportive care (ICU, blood transfusion, etc.)
Drug Classification by Action Site - Mnemonic: "Blood, Liver, Both"
| Drug | Acts on | Species |
|---|---|---|
| Chloroquine | Erythrocytic (blood schizonticide) | vivax, ovale, malariae, sensitive falciparum |
| Artemisinin / Artesunate | Erythrocytic (all stages) | All species; rapid action |
| Primaquine | Liver (hypnozoites) + gametocytes | vivax, ovale (prevents relapse) |
| Quinine / Quinidine | Erythrocytic | falciparum (parenteral for severe) |
| Mefloquine | Erythrocytic | falciparum |
| Doxycycline | Erythrocytic (slow) | falciparum (adjunct) |
| Atovaquone-Proguanil (Malarone) | Erythrocytic + liver | falciparum (prophylaxis + treatment) |
Special Situations:
- Pregnancy: Quinine + Clindamycin (1st trimester); ACT (2nd/3rd trimester)
- G6PD deficiency: Avoid Primaquine (causes hemolysis); use weekly Primaquine slowly if needed
- Chloroquine resistance: Widespread in P. falciparum; also seen increasingly in P. vivax
8. PROPHYLAXIS
| Drug | Use |
|---|---|
| Chloroquine (weekly) | Sensitive areas (not falciparum endemic) |
| Doxycycline (daily) | All malaria-endemic areas including resistant falciparum |
| Mefloquine (weekly) | Chloroquine-resistant areas |
| Atovaquone-Proguanil (daily) | Short trips to resistant areas |
Personal Protection: Bed nets (LLIN) + Repellents (DEET) + Clothing + Avoid peak biting hours (dusk to dawn)
9. PROTECTIVE FACTORS AGAINST MALARIA
Mnemonic: "SHED G"
- S - Sickle cell trait (HbAS) - P. falciparum cannot thrive
- H - HbC, HbE - protective
- E - Elliptocytosis / Hereditary spherocytosis
- D - Duffy antigen negativity - protects against P. vivax
- G - G6PD deficiency - some protection against falciparum
10. QUICK EXAM SUMMARY - HIGH YIELD FACTS
| Fact | Answer |
|---|---|
| Most dangerous species | P. falciparum (malignant tertian) |
| Only crescent-shaped gametocytes | P. falciparum |
| Hypnozoites (relapse) | P. vivax + P. ovale |
| Longest incubation | P. malariae (18-40 days) |
| 72-hr fever cycle | P. malariae (quartan) |
| 24-hr fever cycle | P. knowlesi (quotidian) |
| Blackwater fever | P. falciparum complication |
| Cerebral malaria | P. falciparum (PfEMP1 + ICAM-1/CD36/VCAM-1) |
| Drug for hypnozoites | Primaquine |
| Contra in G6PD deficiency | Primaquine |
| Gold standard diagnosis | Thick blood smear + Giemsa stain |
| Falciparum in blood smear only | Ring forms + Crescent gametocytes (schizonts absent) |
| Schuffner's dots | Vivax + Ovale |
| Maurer's clefts | Falciparum |
| RDT for falciparum | HRP-2 antigen |
| Severe malaria treatment | IV Artesunate |
| Vaccine antigen used | Circumsporozoite protein (RTS,S vaccine - "Mosquirix") |
11. ONE-LINE MNEMONICS SUMMARY
| Mnemonic | What it helps remember |
|---|---|
| FKVOM | 5 species: Falciparum, Knowlesi, Vivax, Ovale, Malariae |
| "VOS has dots" | Vivax + Ovale = Schuffner's dots |
| "Banana for Falciparum" | Crescent/banana gametocyte = P. falciparum |
| "Vivax Loves Young" | Vivax prefers young RBCs via Duffy antigen |
| "Malariae is Old" | Malariae prefers old RBCs |
| "CRAB-H" | Complications of falciparum malaria |
| "MINT-C" | Routes of transmission |
| "SHED G" | Protective factors against malaria |
| "PfEMP1 = Knob = Stuck" | Cytoadherence mechanism in falciparum |
| "Primaquine = Liver killer" | Only drug that kills hypnozoites (prevents relapse) |
| 48-48-48-72-24 | Fever cycles: V,O,F = 48 |
Sources: Murray's Medical Microbiology 9e (Murray, Rosenthal, Pfaller), Robbins & Kumar Basic Pathology, Tietz Textbook of Laboratory Medicine 7th Ed. - All concepts align with Apurba Sastry's Essentials of Medical Parasitology coverage of MI 3.6 competency.
This is a shared conversation. Sign in to Orris to start your own chat.