Renal cell carcinoma for 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I have everything needed. Here is the comprehensive 10-mark answer on Renal Cell Carcinoma:
Renal Cell Carcinoma (RCC)
Definition
Renal cell carcinoma (RCC) is a group of malignant epithelial neoplasms arising from the renal tubular epithelium, located predominantly in the cortex. It is not a single entity but a collection of distinguishable tumors, each with a characteristic morphology and genetic profile. RCC accounts for 80-85% of all primary malignant renal neoplasms and 2-3% of all adult cancers. Classically known as "hypernephroma" or "clear cell carcinoma," it is now understood to encompass several subtypes.
Epidemiology
- Sixth most common cancer in men, ninth most common in women
- Male: Female ratio = 2:1 to 3:1
- Peak incidence in the 6th-7th decade of life
- Over 75,000 new cases diagnosed annually in the US; ~14,000 deaths/year
- Highest incidence in Black Americans; lowest in Asians/Pacific Islanders
Risk Factors:
- Cigarette smoking (most modifiable risk factor; risk decreases ~20 years after cessation)
- Obesity (risk rises with increasing BMI)
- Hypertension and diuretic use
- Acquired polycystic kidney disease (complication of chronic dialysis) - 30-fold increased risk
- Pre-existing renal disease: polycystic kidney disease, horseshoe kidney, chronic renal failure on hemodialysis
- Occupational exposure to cadmium
- Genetic predisposition (VHL disease, hereditary papillary RCC)
Classification and Pathogenesis
RCC is classified into three major subtypes based on morphology and molecular genetics:
1. Clear Cell Carcinoma (65% of RCC)
- Most common subtype; derived from the proximal convoluted tubule
- Accounts for ~90% of all metastases from RCC
- Molecular hallmark: Loss/inactivation of both copies of the VHL (von Hippel-Lindau) gene on chromosome 3p25
- In VHL disease (autosomal dominant), germline mutation of VHL predisposes to bilateral, multifocal clear cell RCC in 40-60% of patients
- Without VHL protein, hypoxia-inducible factors (HIFs) are not degraded, remaining high even under normoxic conditions
- HIFs stimulate VEGF expression, driving angiogenesis and tumor vascularization
- HIF also collaborates with MYC to alter cellular metabolism and promote growth
- Recent genomic studies also show frequent loss-of-function mutations in genes regulating histone methylation (epigenomic changes)
2. Papillary Renal Cell Carcinoma (10-15% of RCC)
- Frequently multifocal and bilateral; tends to present at an early stage
- Unifying feature: Genetic abnormalities activating MET (tyrosine kinase receptor on chromosome 7q)
- Sporadic form: increased MET copy number or somatic activating mutations in MET
- Familial form: germline activating MET mutations
- Accounts for ~25% of total tumors but only 10% of metastases - more indolent than clear cell
3. Chromophobe Renal Cell Carcinoma (5% of RCC)
- Arises from intercalated cells of collecting ducts
- Characterized by multiple losses of entire chromosomes, leading to extreme hypoploidy
- Generally has a favorable prognosis
- Cells have eosinophilic (pale, chromophobe) cytoplasm with distinct cell membranes and perinuclear haloes
Morphology
Gross:
- Clear cell carcinoma: Large, solitary, spherical mass (3-15 cm), arising in the cortex; cut surface is yellow to orange due to abundant cytoplasmic lipid and glycogen, with areas of hemorrhage and cystic change
- Tumor may fungate through the calyceal system into the ureter
- Classic feature: Invasion of the renal vein, with tumor growing as a solid column - may extend all the way into the inferior vena cava and even into the right heart
- Papillary RCC: Less vividly yellow (lower lipid content); shows necrosis, hemorrhage, cystic degeneration
- Chromophobe RCC: Tan-brown gross appearance
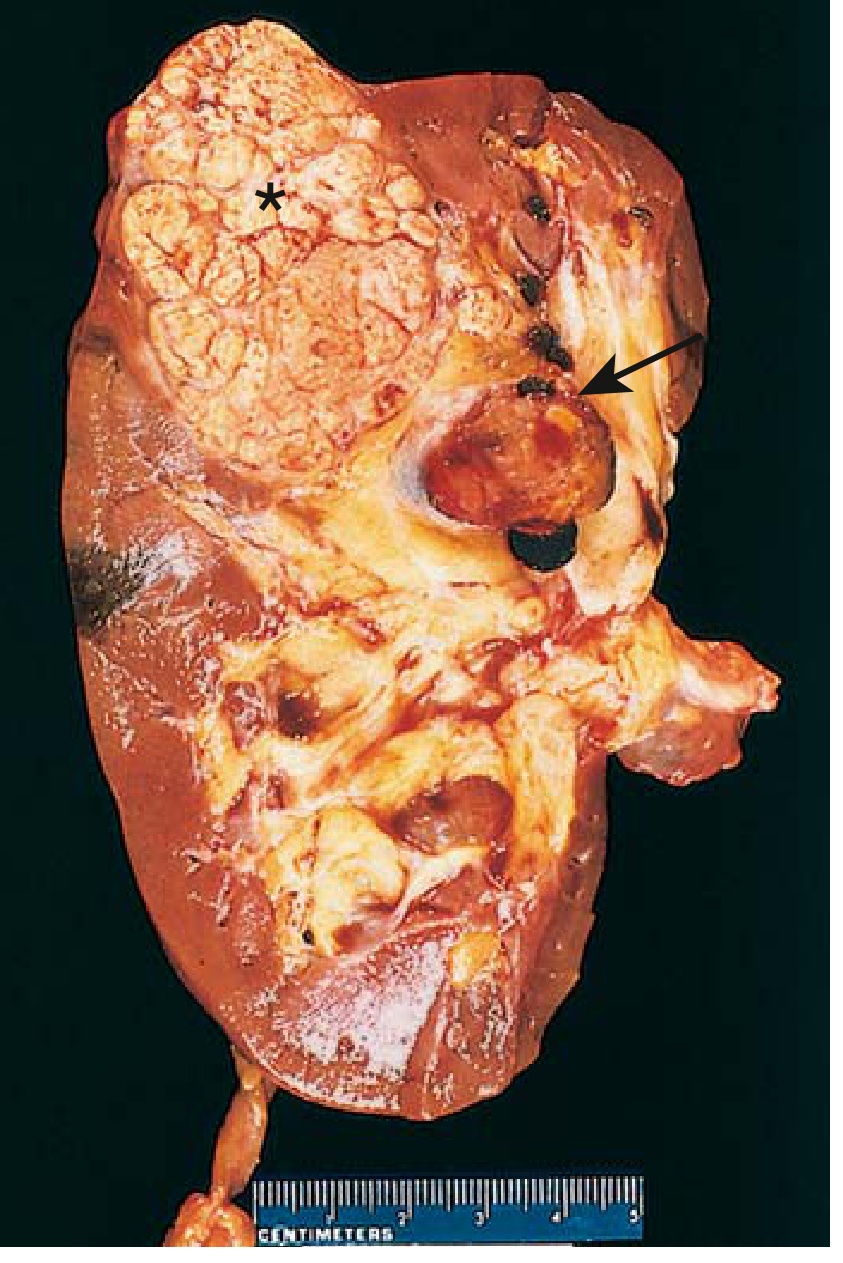
FIG: Cross-section of kidney showing clear cell RCC (asterisk) - yellowish-orange spherical neoplasm in upper pole, with tumor thrombus in dilated renal vein (arrow). (Robbins & Kumar Basic Pathology)
Microscopic:
- Clear cell type (A): Cells with vacuolated, clear cytoplasm (lipid and glycogen dissolved out) and distinct cell membranes; arranged in nests separated by delicate fibrovascular stroma; small, round nuclei
- Papillary type (B): Cuboidal to low columnar cells lining papillae with fibrovascular cores; cuboidal cells with eosinophilic to clear cytoplasm
- Chromophobe type (C): Eosinophilic cytoplasm mixed with pale granular cells; very prominent distinct cell membranes, perinuclear haloes
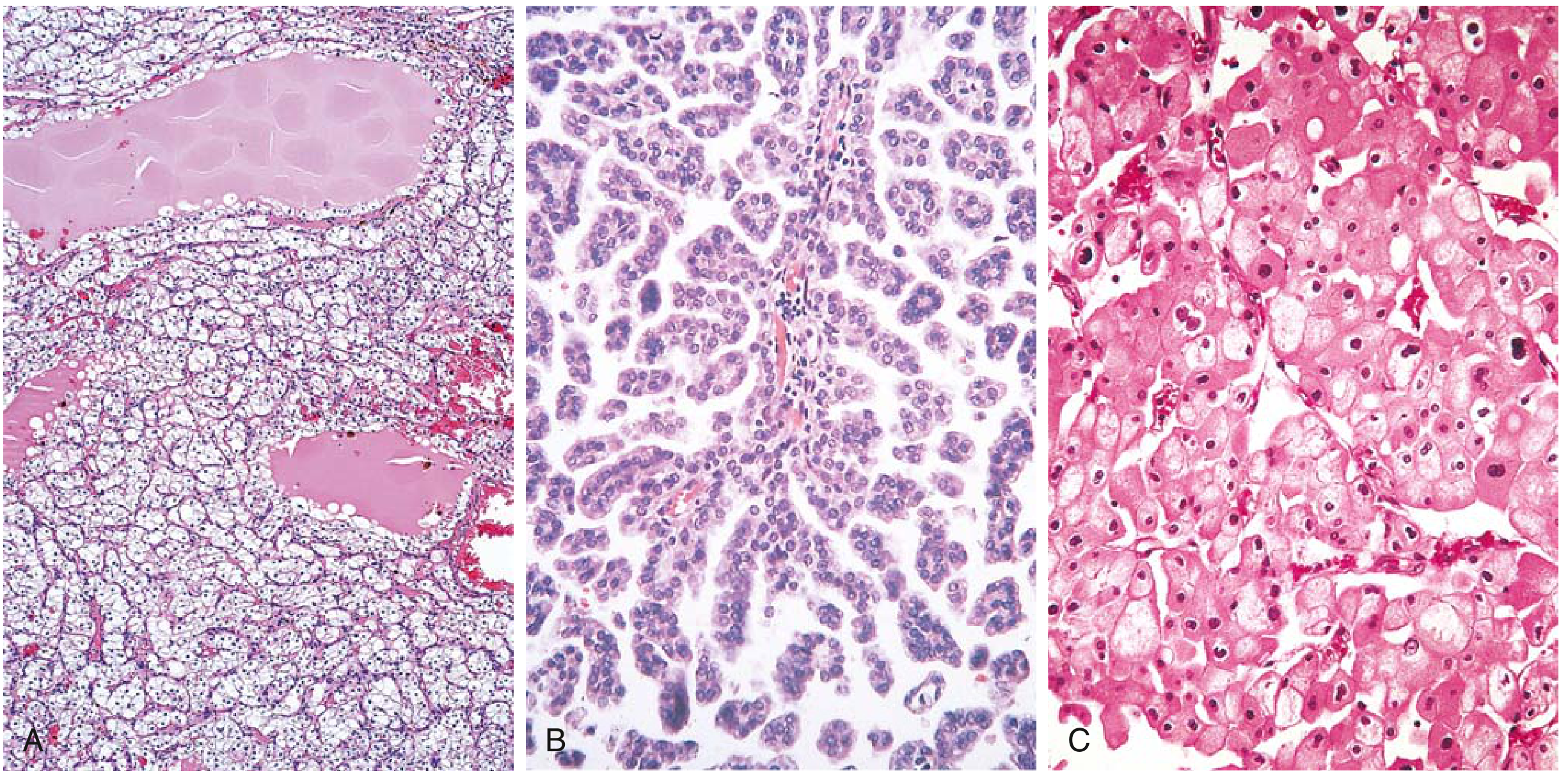
FIG: RCC histological subtypes - (A) Clear cell, (B) Papillary, (C) Chromophobe. (Robbins & Kumar Basic Pathology)
Clinical Features
The classic triad is:
- Painless hematuria (gross or microscopic)
- Palpable flank/abdominal mass
- Dull flank pain
However, all three are present simultaneously in only 10% of cases. Hematuria is the single most frequent presenting symptom (>50% of cases); it is typically intermittent and macroscopic over a background of persistent microscopic hematuria.
Many tumors today are detected incidentally on imaging (CT/MRI done for other reasons).
Paraneoplastic Manifestations (important for exam!)
RCC is notorious for producing systemic effects distant from the tumor:
| Paraneoplastic Feature | Mechanism | Frequency |
|---|---|---|
| Anemia | Chronic disease / blood loss | 52% |
| Erythrocytosis/Polycythemia | Ectopic erythropoietin production | 4-10% |
| Hypercalcemia | PTHrP production | 13% |
| Hypertension | Renin production | 3% |
| Fever / night sweats | Cytokine (IL-6) secretion | 8% |
| Hepatic dysfunction (Stauffer syndrome) | Non-metastatic hepatopathy | 32% |
| Cushing syndrome | ACTH production | Rare |
| Weight loss / malaise | Systemic | 19-23% |
Metastatic patterns: Lungs (most common), bone, liver, brain, contralateral kidney. Occasionally presents as a pathological fracture or lung nodule before the primary is discovered.
Diagnosis
Imaging:
- Ultrasound: Initial screening; can differentiate solid from cystic, but low sensitivity for small lesions
- Multiphasic contrast-enhanced CT (gold standard): Best for evaluating solid lesions; done in pre-contrast, arterial (~25 sec), nephrographic (~90 sec), and excretory phases. Key: enhancement on nephrographic phase differentiates malignant from benign
- Clear cell RCC: Avid enhancement in corticomedullary phase; becomes hypoenhancing in nephrographic phase
- Papillary RCC: Hypointense on T2-weighted MRI; hypoenhancing on all contrast phases
- Chromophobe RCC: Avid corticomedullary enhancement, less than clear cell
- MRI: Preferred when contrast is contraindicated (poor renal function); excellent for delineating venous thrombus extension into renal vein/IVC; helpful for complex cysts
Workup:
- CBC, chemistry profile (liver function, calcium, creatinine)
- CT chest, abdomen, pelvis
- Bone scan if: advanced disease, hypercalcemia, bone pain, elevated alkaline phosphatase
- Staging by TNM system (AJCC 8th edition)
TNM Staging
| Stage | T | N | M |
|---|---|---|---|
| I | T1 (≤7 cm, confined to kidney) | N0 | M0 |
| II | T2 (>7 cm, confined to kidney) | N0 | M0 |
| III | T1-T3, N1 or T3 (extends into major veins/perinephric tissue) | N0 or N1 | M0 |
| IV | T4 (beyond Gerota's fascia) or any T/N | Any | M1 |
T3 sub-stages (important):
- T3a: Extends into renal vein/segmental branches, or perinephric fat
- T3b: Extends into vena cava below diaphragm
- T3c: Extends into vena cava above diaphragm or invades IVC wall
Treatment
Localized Disease (Stages I-III)
- Partial nephrectomy (nephron-sparing surgery): Preferred for tumors ≤7 cm; provides equivalent local control and survival to radical nephrectomy while preserving renal function; open or laparoscopic technique
- Radical nephrectomy: Preferred for large, centrally located tumors; tumors replacing most of the parenchyma; tumors with regional adenopathy; tumors extending into the IVC; can be open or laparoscopic
- Ipsilateral adrenal gland removed; regional lymph node dissection is optional/controversial
- Adjuvant therapy: RCC is resistant to both radiation and cytotoxic chemotherapy
- Sunitinib (VEGF tyrosine kinase inhibitor) or pembrolizumab (anti-PD-1) recommended for high-risk cases after nephrectomy
Metastatic Disease (Stage IV)
- ~30% of patients present with metastatic disease; another 20-30% relapse after surgery
- First-line systemic therapy: Anti-PD-1 checkpoint inhibitors + tyrosine kinase inhibitors (TKIs):
- Nivolumab + cabozantinib or nivolumab + ipilimumab (anti-CTLA-4) - significantly superior to sunitinib monotherapy
- Pembrolizumab + axitinib or pembrolizumab + lenvatinib - recommended in all risk groups
- mTOR inhibitors: Everolimus, temsirolimus - used for previously treated patients
- Belzutifan (HIF-2α inhibitor) - useful for VHL-mutation associated tumors
- Radiation therapy: Palliative role for bone and brain metastases
- Metastasectomy: May extend survival in selected patients (disease-free interval >1 year, solitary lung metastasis)
Prognosis
| Stage | 5-Year Survival |
|---|---|
| Stage I (localized, ≤7 cm) | 90-95% |
| Stage II-III | 40-70% |
| Stage IV (metastatic) | <10% |
Prognostic factors: tumor size, histologic grade (Fuhrman/WHO-ISUP grading), pathologic stage, venous involvement, and histologic subtype (clear cell > papillary/chromophobe in terms of aggressiveness).
Sources:
- Robbins & Kumar Basic Pathology, Chapter 12 (Kidney)
- Goldman-Cecil Medicine, Chapter 182 (Renal Cell Carcinoma)
- National Kidney Foundation Primer on Kidney Diseases, 8th ed., Chapter 6
- Campbell-Walsh-Wein Urology, Part XI
This is a shared conversation. Sign in to Orris to start your own chat.