Opv ipv fipv vaccine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple textbooks. Here is the complete, detailed answer:
OPV, IPV, and fIPV - Polio Vaccines
Overview
Two main types of polio vaccine exist, each targeting all three poliovirus serotypes (types 1, 2, and 3):
| Feature | OPV (Oral Polio Vaccine) | IPV (Inactivated Polio Vaccine) | fIPV (Fractional IPV) |
|---|---|---|---|
| Developer | Albert Sabin (1963) | Jonas Salk (1955) | Derived from IPV |
| Type | Live attenuated | Killed/inactivated | Killed/inactivated |
| Route | Oral | Subcutaneous/IM | Intradermal |
| Dose | Standard dose | 0.5 ml | 0.1 ml (1/5th of full IPV) |
| Antibody produced | IgA (mucosal) + IgG | IgG (systemic) | IgG (systemic) |
| Herd immunity | Yes (fecal-oral spread) | No | No |
| VAPP risk | Yes | None | None |
OPV - Oral Polio Vaccine (Sabin Vaccine)
- Composed of live, attenuated virus strains developed by Albert Sabin, first licensed in 1963
- Given orally - replicates in oropharynx and intestinal epithelial cells without causing pathogenicity
- Produces IgA antibodies at mucosal surfaces (gastrointestinal tract), which blocks viral entry and transmission - this is why OPV is superior for gut immunity
- Also produces IgG systemic immunity
- 4-dose schedule: 2 months, 4 months, 6-18 months, and 4-6 years
- Produces antibodies to all 3 serotypes in >95% of recipients
- Dose is lower than IPV because OPV replicates in the gut and the resulting antibody titer is much higher
- Spreads to unvaccinated contacts - provides indirect "herd" protection
- Cheaper and easier to administer - no syringe, no trained staff needed
- Major advantage in developing countries for mass immunization
OPV Types:
- tOPV (trivalent OPV) - contained types 1, 2, and 3 - used until April 2016
- bOPV (bivalent OPV) - contains only types 1 and 3 - used since April 2016 (after "The Switch")
- mOPV (monovalent OPV) - contains only 1 serotype - used in targeted campaigns
Disadvantage - VAPP and VDPV:
- Vaccine-Associated Paralytic Poliomyelitis (VAPP): OPV attenuated virus can rarely revert to neurovirulence. Estimated at ~4 cases/1,000,000 birth cohort/year. Most frequently associated with Sabin type 3 (60% of VAPP cases), then type 2, then type 1. ~1 case per 2.4 million doses distributed
- Vaccine-Derived Poliovirus (VDPV): OPV strains undergo genetic changes during replication; in communities with low vaccination coverage, this can result in circulating VDPVs that cause paralytic disease indistinguishable from wild poliovirus
- cVDPV - circulating VDPV (person-to-person transmission)
- iVDPV - immunodeficiency-associated VDPV (in immunocompromised persons)
- aVDPV - ambiguous VDPV (sewage isolates or unknown source)
IPV - Inactivated Polio Vaccine (Salk Vaccine)
- Killed/inactivated poliovirus developed by Jonas Salk, introduced in 1955
- Given by subcutaneous injection (or IM)
- Full dose = 0.5 ml
- Stimulates IgG antibodies that eliminate the virus during viremia (blood-borne phase)
- Does NOT produce significant mucosal IgA - so does not prevent gut colonization or fecal-oral transmission (no herd immunity via this route)
- Primary vaccination with 4 doses produces antibody in >98% of recipients
- Safe - no significant side effects, no risk of VAPP
- Currently the exclusive vaccine used in the USA since 1999 and in most developed countries
- Does not replicate - does not spread to contacts
- More expensive than OPV; requires cold chain and trained staff for injection
Enhanced-potency IPV (eIPV):
- The current product used since the mid-1980s has higher antigen content than the original Salk vaccine - more immunogenic
fIPV - Fractional IPV
- Fractional IPV (fIPV) is IPV given at 1/5th the standard dose (0.1 ml instead of 0.5 ml), administered by intradermal injection
- The intradermal route is highly immunogenic due to the high density of Langerhans cells (antigen-presenting cells) in the dermis - this compensates for the reduced antigen dose
- Studies show that 2 intradermal fIPV doses are non-inferior to 1 full-dose IPV in generating seroprotective antibody titers
- Key advantage: cost savings (stretches IPV supply 5x), which is critical for resource-limited countries needing to introduce IPV rapidly
India's fIPV Policy:
As part of the Polio Endgame Strategy, India introduced IPV on 30 November 2015. Given the large birth cohort and supply constraints, India chose fIPV:
- Given as 0.1 ml intradermal injection
- Schedule: at 6 weeks and 14 weeks of age (under UIP)
- Rationale: mitigate the risk of type 2 poliovirus after the tOPV to bOPV switch in April 2016 (since bOPV does not protect against type 2)
The Polio Endgame Strategy and OPV-IPV Sequencing
The Polio Eradication and Endgame Strategic Plan 2013-2018 outlined key steps:
- Introduce at least 1 dose of IPV into routine immunization by end of 2015 (before the tOPV-to-bOPV switch)
- "The Switch" (April 18 - May 1, 2016): Global synchronized cessation of tOPV, replacing with bOPV - removing type 2 component from all OPV
- Eventual withdrawal of all OPV (planned for 2019-2020) to eliminate VDPV risk entirely
Why this sequencing?
- Wild poliovirus type 2 has not been detected since 1999 (declared eradicated September 2015)
- Wild poliovirus type 3 has not been detected since November 2012
- Continuing to use tOPV meant the risk of VAPP and cVDPV from type 2 OPV now outweighed its benefit
- IPV must be introduced BEFORE removing OPV type 2 to protect the birth cohort against any accidental/lab leak of type 2 virus
- WHO recommends: countries using OPV-only should add at least 1 dose of IPV (3 OPV + 1 IPV)
- Adding a dose of trivalent IPV after immunization with bOPV also reduces the risk of type 2 vaccine-derived polio
Key Comparison Summary
| Aspect | OPV | IPV | fIPV |
|---|---|---|---|
| Immunity type | Mucosal IgA + systemic IgG | Systemic IgG only | Systemic IgG only |
| Herd effect | Yes | No | No |
| VAPP risk | Yes (~1/2.4M doses) | None | None |
| VDPV risk | Yes | None | None |
| Cost | Low | High | Moderate (5x cheaper than full IPV) |
| Administration | Oral drops | SC/IM injection | Intradermal injection |
| Cold chain | Required | Required | Required |
| Use in developing countries | Primary vaccine (bOPV now) | Supplemental (1+ dose required) | India and other LMICs |
| Use in USA/developed world | Discontinued (since 1999-2000) | Exclusive use | Not routinely used |
Sources: Park's Textbook of Preventive and Social Medicine; Sherris & Ryan's Medical Microbiology, 8th Ed; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine
Pulse polio
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Excellent - I now have comprehensive details. Here is the full, structured answer:
Pulse Polio Immunization Programme (PPI)
Definition
"Pulse" describes the sudden, simultaneous, mass administration of OPV on a single day to all children 0-5 years of age, regardless of their previous immunization status. It is a Supplementary Immunization Activity (SIA) - the doses given are extra doses that supplement (and do NOT replace) routine immunization doses.
Launch and History
| Year | Event |
|---|---|
| 1995 | Programme launched in India |
| 9 Dec 1995 | First National Immunization Day (NID) |
| 20 Jan 1996 | Second NID round (6 weeks after first) |
| Initial target | Children under 3 years |
| Later revised (WHO recommendation) | Extended to children under 5 years |
| 1999-2000 | House-to-house vaccination of missed children introduced |
| 25 Feb 2012 | India removed from list of polio-endemic countries |
| 27 March 2014 | India certified polio-free |
The last case of polio in India was reported from Howrah, West Bengal.
Key Features
- Two rounds per year, ~4-6 weeks apart
- Conducted during low transmission season (November to February)
- Peak transmission in India: June to September
- NIDs (National Immunization Days) cover ~172 million children
- SNIDs (Sub-National Immunization Days) cover 40-80 million children (used in high-risk states like UP and Bihar)
- No minimum interval between PPI doses and scheduled OPV doses
- Children aged 0-1 year receive both scheduled and PPI doses
Strategies Used in PPI
7 Strategies for Polio Eradication (India):
(a) Conduct Pulse Polio Immunization days every year until poliomyelitis is eradicated
(b) Sustain high levels of routine immunization coverage
(c) Monitor OPV coverage at district level and below
(d) Improve AFP (Acute Flaccid Paralysis) surveillance capable of detecting all cases of AFP due to polio and non-polio aetiology
(e) Ensure rapid case investigation, including collection of stool samples for virus isolation
(f) Follow-up of all AFP cases at 60 days to check for residual paralysis
(g) Conduct outbreak control for confirmed/suspected poliomyelitis cases within 48 hours of notification
Vaccination Delivery Strategies (Reaching Every Child)
- Fixed booths - at designated immunization sites
- House-to-house visits - for children missed at booths (introduced 1999-2000)
- Transit vaccination - at railway stations, inside long-distance trains, major bus stops, markets, religious congregations, major road crossings
- Border booths - special booths at Wagah border, Attari train station (Punjab), Munabo train station (Barmer, Rajasthan) - to cover children coming from neighboring countries
- Mobile teams deployed in high-risk areas of UP and Bihar
- Migratory population tracking - migrants from UP and Bihar identified in Punjab, Haryana, Gujarat, and West Bengal, covered during SNIDs
Mopping Up
- Last stage in polio eradication
- Door-to-door immunization in high-risk districts where wild poliovirus is known/suspected to be circulating
- Targets specific geographic pockets rather than the whole country
Improvements Made During PPI
Vaccine Vial Monitor (VVM) - Introduced 1998
- A colour label on vaccine bottles with a white square inside a deep blue circle
- If the vaccine is exposed to higher temperature, the white square gradually turns blue
- When the square matches the surrounding blue circle in colour - vaccine is considered ineffective
- Made mandatory in all vaccine procurements since 1998
- Ensures health workers can easily verify vaccine potency at the point of use
Monovalent OPV (mOPV)
- From 2005-2006, mOPV1 and mOPV3 were developed and licensed for targeted use during SIAs based on surveillance data
- Specific recommendation in 2006: all neonates in high-risk areas of UP given a "birth dose" of mOPV1
AFP Surveillance (Backbone of PPI)
Supported since 1997 via a network of Surveillance Medical Officers (SMOs):
- SMOs are specially trained and responsible for defined geographic areas
- National surveillance team based in Delhi
- Weekly reporting system established
- Any case of AFP in children under 15 years must be reported mandatorily
- Active surveillance extended to ALL causes of AFP (not just polio) since 1992
- Cases reported: 1,005 in 1996 → 11,675 by later years (due to better detection)
- Stool specimen collection completeness: 59% (1998) → 82% (by Sept 2020)
- Environmental surveillance continues at 4+ sites (to detect VDPVs)
- Line listing of all AFP cases maintained (started 1989) - to check duplication, identify high-risk pockets, document high-risk age groups
Special Efforts in High-Risk Areas (UP and Bihar)
- Government identified 107 high-risk blocks for polio - multi-pronged strategy implemented (sanitation + hygiene + clean water + OPV)
- Every newborn in UP and Bihar identified and vaccinated during campaigns and tracked for 8 subsequent rounds
- Deployment of additional personnel for intensified SIAs
- Social mobilization using local influencers, community and religious leaders
Post-Eradication Measures (Maintaining Polio-Free Status)
- All states/UTs developed Rapid Response Teams (RRT) for outbreak response
- Emergency Preparedness and Response Plan (EPRP) developed by all states
- Rolling emergency stock of OPV maintained for WPV/cVDPV detection
- Extremely high vigilance for importation or circulation of poliovirus and VDPV
- Introduction of IPV (fIPV) from 30 November 2015 as part of Polio Endgame Strategy
- tOPV to bOPV switch carried out in April 2016
Source: Park's Textbook of Preventive and Social Medicine
Cold chain
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here it is:
Cold Chain
Definition
The cold chain is a system of storage and transport of vaccines at low temperature from the manufacturer to the actual vaccination site. It is necessary because vaccine potency (the ability to adequately protect the vaccinated patient) can diminish - and once lost, can never be regained - if vaccines are exposed to inappropriate temperatures.
The success of any national immunization programme depends on the supply chain meeting the "6 Rights":
The right vaccine - in the right quantity - at the right place - at the right time - in the right condition (no temperature breaks) - at the right cost
Temperature Requirements
Vaccines are sensitive biological products. Different vaccines are sensitive to different temperature extremes:
Vaccines Sensitive to FREEZING (must never go below 0°C):
- Cholera
- DTwP, DTaP, Pentavalent (DTwP-Hep B-Hib)
- Hepatitis B
- Hib (liquid)
- HPV
- IPV
- Meningococcal A & C
- Pneumococcal (PCV)
- Rotavirus (liquid)
- Td, TT
- Typhoid (Vi polysaccharide)
Vaccines Sensitive to HEAT - Grouped by Sensitivity:
| Group | Heat Sensitivity | Vaccines |
|---|---|---|
| A | Most sensitive | OPV |
| B | - | Influenza |
| C | - | IPV, JE (freeze-dried), Measles/MR/MMR (freeze-dried) |
| D | - | Cholera, DTwP/Pentavalent, Hib (liquid), Measles (FD), Rotavirus, Rubella (FD), Yellow fever (FD) |
| E | - | BCG, HPV, JE, Tetanus/TD/Td |
| F | Least sensitive | Hepatitis B, Hib (freeze-dried), Meningococcal A, Pneumococcal |
Note: Heat stability data for freeze-dried vaccines applies only to unopened vials. Most freeze-dried vaccines rapidly lose potency after reconstitution. Opened multi-dose vials without preservative must be kept at +2°C to +8°C and used within 4 hours of opening.
Cold Chain Equipment
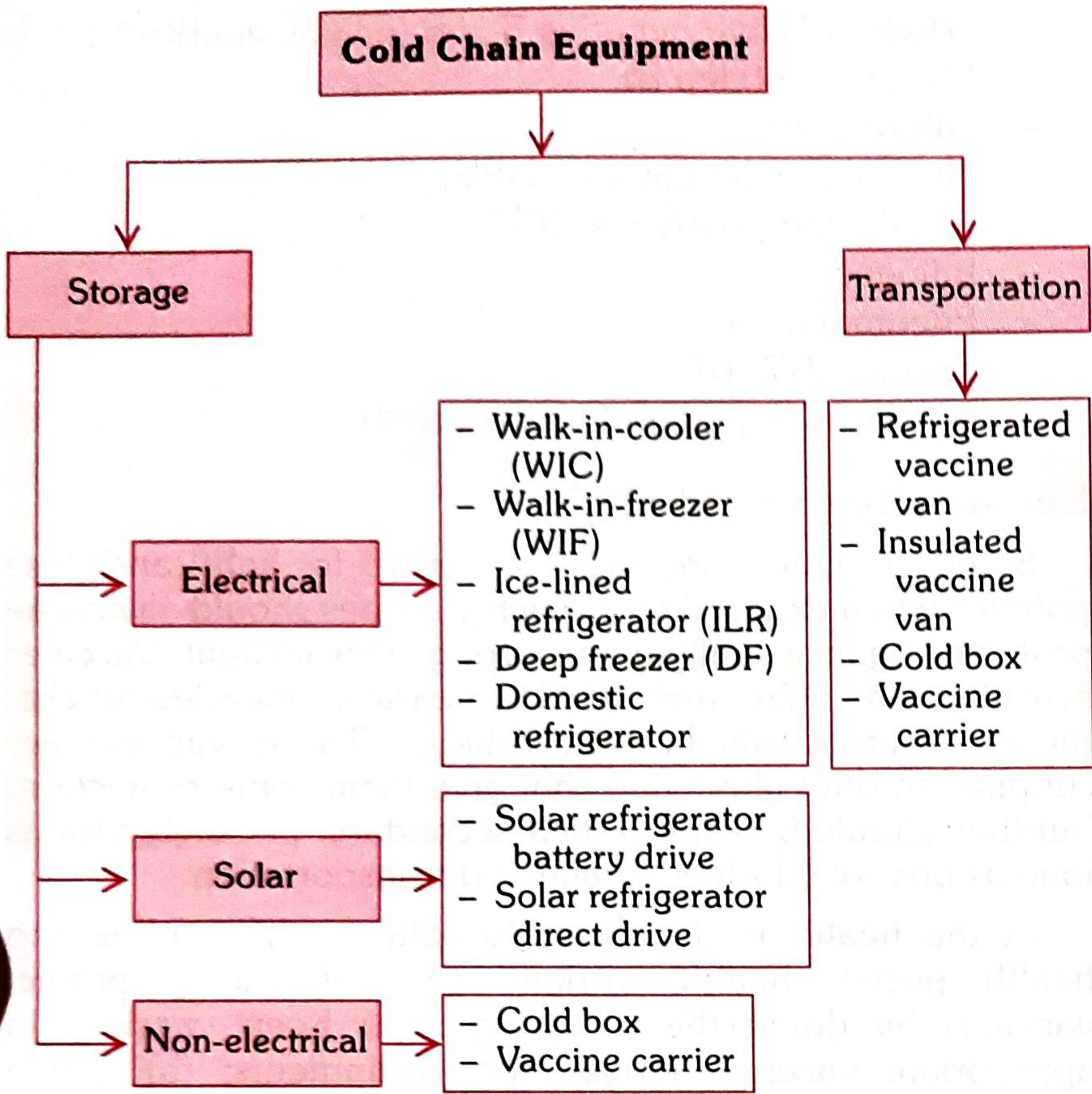
A. STORAGE Equipment
Electrical Storage:
1. Walk-in-Freezer (WIF)
- Pre-fabricated modular PUF (polyurethane foam) insulated panel cold room
- Two identical refrigeration units + standby generator (auto start on power cut)
- Temperature: -15°C to -25°C
- Location: National, state, and regional vaccine stores
- Use: Bulk storage of OPV; preparation of frozen ice packs
2. Walk-in-Cooler (WIC)
- Pre-fabricated modular PUF insulated panel cold room
- Temperature: +2°C to +8°C
- Capacity: 16.5, 32, and 40 cubic meter sizes (India)
- Location: Government Medical Store Depots, state and regional vaccine stores; some district stores
- Use: Large quantity storage of all UIP vaccines (BCG, Hep B, DPT, Pentavalent, IPV, Measles, TT)
- Comes with continuous temperature recorder and alarm system
3. Deep Freezer (DF)
- Top opening lid (prevents loss of cold air)
- Temperature: -15°C to -25°C
- Use:
- Storing OPV for up to 3 months (district level and above)
- Freezing ice packs (sub-district level only)
- Important: DF used for vaccine storage should NOT be used simultaneously for ice pack preparation (risks raising cabinet temperature)
- Limited hold-over time (depends on number of frozen ice packs and frequency of opening)
4. Ice-Lined Refrigerator (ILR) - Most important link in cold chain
- Top-opening (holds cold air better than front-opening)
- Temperature: +2°C to +8°C
- Needs minimum 8 hours continuous electricity in a 24-hour period
- Has lining of water containers (ice packs/tubes) fitted around all walls
- When electricity fails - the ice lining maintains safe temperature for vaccines
- Much better hold-over time than DF or domestic refrigerators
- Larger ILR at district HQ; smaller ILR at PHC
- Vaccine placement inside ILR basket:
- Bottom of basket: OPV, BCG, Measles, JE (heat-sensitive, not freeze-sensitive)
- Upper part of basket: DPT, TT, Hep B, IPV, Pentavalent and diluents (freeze-sensitive)
- Never keep vaccines directly on the floor of the ILR (risk of freezing)
5. Domestic Refrigerator (Front-load)
- Temperature: +2°C to +8°C
- Limited hold-over time and capacity
- Used at private clinics/nursing homes (only if continuous power supply is assured)
- Placement: Measles, BCG, Rotavirus, OPV on top shelf; DPT, Pentavalent, TT, IPV, Hep B, JE on middle shelf; diluents next to their respective vaccines; ice packs on bottom shelf
Solar Storage:
- Solar refrigerator battery drive - uses 12/24V DC compressor charged by solar energy; vaccine compartment +2°C to +8°C; freezer compartment up to -7°C
- Solar refrigerator direct drive - freezes phase change material during sunlight, uses the "ice bank" to keep refrigerator cold during night/cloudy days
B. TRANSPORTATION Equipment
| Equipment | Use |
|---|---|
| Refrigerated vaccine van | Transports large vaccine quantities maintaining temperature |
| Insulated vaccine van | For transit transport with ice packs |
| Cold box | Medium-term transport and storage; field use |
| Vaccine carrier | Outreach sessions; short-duration field use |
Risk of cold chain failure is greatest at sub-centre and village level - therefore vaccines are NOT stored at sub-centre level and must be supplied on the day of use.
Hold-Over Time
Defined as: "Time taken by the equipment to raise the inside cabinet temperature from its temperature at the time of power cut to the maximum of its recommended range."
Hold-over time depends on:
- (a) Ambient temperature - higher ambient = shorter hold-over time
- (b) Frequency of lid opening and basket use
- (c) Quantity of vaccines inside with adequate spacing
- (d) Condition of ice-pack lining (frozen/partially frozen/melted)
Vaccine Vial Monitor (VVM)
A VVM is a chemical indicator label attached to the vaccine container by the manufacturer. It records cumulative heat exposure through a gradual colour change.
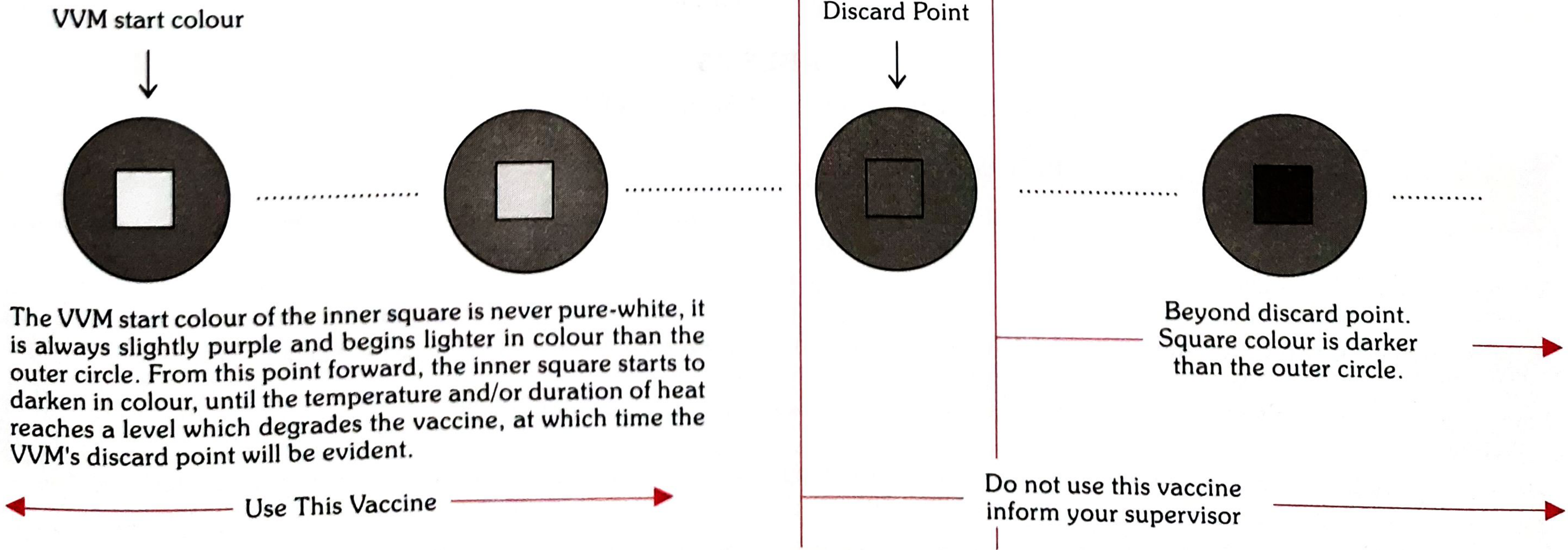
- Inner square lighter than outer circle = Use the vaccine (safe)
- Inner square same colour or darker than outer circle = DISCARD; do not use; inform supervisor
- The VVM start colour is never pure white - it is always slightly purple and begins lighter than the outer circle
- 4 types: VVM2, VVM7, VVM14, VVM30 - the number = days taken for the inner square to reach discard point at a constant 37°C
- VVMs do NOT measure exposure to freezing temperature
- VVM status decides which batch to use first - a batch with more heat exposure should be used before one with a longer expiry date
Shake Test (for Freeze-Damaged Vaccines)
Used to check whether freeze-sensitive vaccines have been damaged by temperatures below 0°C. Frozen vaccines form flakes that settle at the bottom.
Procedure:
- Take the suspect "TEST" vial
- Take a vial of the same antigen, manufacturer, and batch → freeze it solid at -20°C overnight in DF → let it thaw (do NOT heat) → this is the "Frozen Control" vial
- Hold both vials together; vigorously shake for 10-15 seconds
- Place both on a flat surface side-by-side; observe for 30 minutes; compare sedimentation rate
Interpretation:
- Test vial sedimentation slower than control → Passes shake test → vaccine not damaged → USE it
- Test vial sedimentation same or faster than control → Fails shake test → vaccine damaged → DO NOT USE → notify supervisor
Open Vial Policy (2015)
Allows reuse of partially used multi-dose vials in subsequent sessions up to 4 weeks (28 days) to reduce vaccine wastage.
Applies to: DPT, TT, Hepatitis B, OPV, Liquid Pentavalent, PCV, and injectable IPV
Conditions for reuse:
- Cold chain maintained at +2°C to +8°C
- VVM has not reached discard point
- Vaccine vial has not been exposed to direct sunlight
- No contamination suspected
Does NOT apply to: BCG, Measles/MR, JE - these must be destroyed after 48 hours or before the next session (whichever is earlier).
Open vials should never be submerged in water (e.g., water accumulated in vaccine carrier) - risk of contamination of the vial septum.
Diluent Storage - Important Rules
- Use ONLY the diluent supplied by the manufacturer (specific pH, volume, and chemical properties)
- Store diluents at +2°C to +8°C in ILR
- If space constraints require storing diluents outside cold chain - cool them for at least 24 hours before use to ensure vaccine and diluent are at the same temperature at reconstitution
- Failure to do so causes thermal shock - death of live organisms in the vaccine
Source: Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.