Carpel tunnel syndrome
Reading File
Finding Sources
Searching PubMed
"carpal tunnel syndrome"[MeSH Terms] AND treatment
Searching the Web
carpal tunnel syndrome diagnosis treatment guidelines 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a complete overview:
Carpal Tunnel Syndrome (CTS)
Anatomy
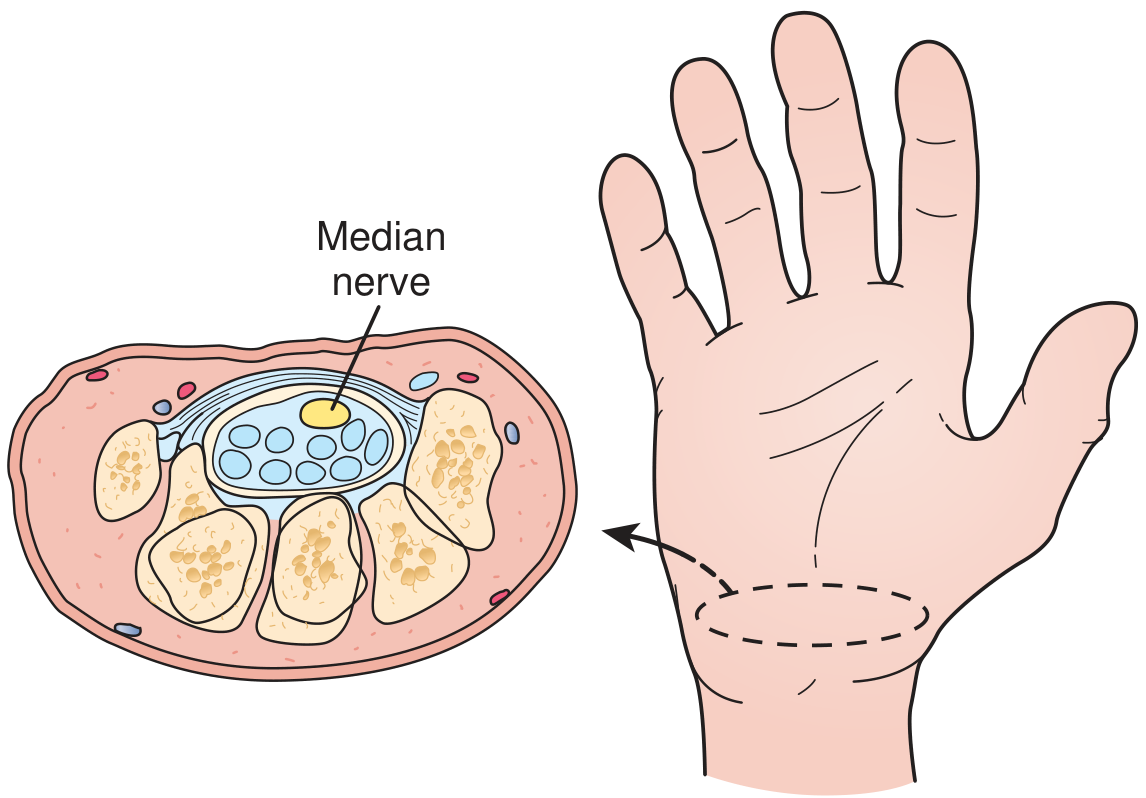
The carpal tunnel is bounded on three sides by the carpal bones and on the palmar side (the "roof") by the transverse carpal ligament (flexor retinaculum). Nine flexor tendons plus the median nerve pass through it. The median nerve is the most palmar (superficial) structure. Any increase in tunnel pressure above 20-30 mmHg impedes epineurial blood flow and impairs nerve function.
- Campbell's Operative Orthopaedics 15e, p. 4502
Definition & Epidemiology
CTS is the most common peripheral nerve entrapment neuropathy, caused by compression of the median nerve at the wrist.
- Affects up to 10% of the U.S. population
- Twice as common in women than men
- Peak incidence: ages 30-60
- Carpal tunnel syndrome, described by Paget in 1854
- Idiopathic in most cases; direct association with specific work activities is often difficult to prove
- Campbell's Operative Orthopaedics 15e | Goldman-Cecil Medicine
Risk Factors / Causes
Patient factors: Female sex, obesity, physical inactivity, smoking, certain occupations
Conditions that decrease tunnel size: Osteoarthritis, fractures, bony deformities
Conditions that increase tunnel contents:
- Tenosynovitis of flexor tendons (most common cause)
- Pregnancy (usually resolves post-delivery)
- Rheumatoid arthritis
- Hypothyroidism
- Diabetes mellitus
- Acromegaly
- Amyloid infiltration
- Sarcoidosis
- Synovial or ganglion cysts
Screening blood tests should be checked in all CTS patients to rule out systemic causes: thyroid function, glucose, rheumatoid factor, ESR.
- Bradley & Daroff's Neurology in Clinical Practice, p. 549
Clinical Features
Symptoms:
- Paresthesia (numbness, tingling, burning) in the thumb, index, middle finger, and radial half of the ring finger - the median nerve sensory distribution
- Symptoms often worse at night - waking the patient from sleep
- Relief by shaking or elevating the hand ("flick sign")
- Pain may radiate up the forearm toward the shoulder (diffuse brachialgia)
- Decreased grip strength
- Subjective numbness may extend into a broader distribution including the medial hand
Signs (in established/severe cases):
- Thenar muscle atrophy (abductor pollicis brevis, opponens pollicis) - reported in ~50% of surgical patients
- Weakness of thumb abduction and opposition
- Objective sensory loss over the distal thumb, index, and middle fingers - but not the thenar eminence (the palmar cutaneous branch exits proximal to the flexor retinaculum, sparing it - a useful diagnostic point)
Diagnosis
CTS is primarily a clinical diagnosis.
Provocative Tests
| Test | Description | Sensitivity | Specificity |
|---|---|---|---|
| Phalen test | Sustained wrist flexion ~90° for 1 min - reproduces symptoms | ~74% | ~75% |
| Tinel sign | Tapping over carpal tunnel at wrist - tingling in median distribution | Lower sensitivity | Most specific |
| Durkan (carpal compression) test | Direct thumb pressure on carpal tunnel for 30 sec | 87% | 90% - best overall |
| CTS-6 score | Clinical scoring tool using history + exam | 95% (score ≥12) | 91% |
Electrodiagnostic Studies (NCS/EMG)
- Distal motor latency >4.5 ms and sensory latency >3.5 ms are abnormal
- NCS: ~90% sensitive, ~60% specific
- EMG: insertional activity, fibrillations, reduced recruitment in abductor pollicis brevis
- Required before surgery; can be negative even in symptomatic patients
- Also helpful for evaluating proximal compression (elbow, cervical spine) and peripheral neuropathy
Ultrasound / MRI
- Useful in atypical or difficult cases; not routinely required
Differential Diagnosis
- Cervical radiculopathy (C6, C7)
- Thoracic outlet syndrome
- Pronator teres syndrome (proximal median nerve entrapment)
- Diabetic peripheral neuropathy
- Inflammatory/autoimmune conditions
Treatment
Step 1 - Conservative (Mild to Moderate CTS)
- Activity modification - avoid provocative activities; ergonomic changes (wrist pads for keyboard users)
- Neutral wrist splinting - particularly at night; effective for most patients
- Nerve gliding exercises - routinely prescribed, can provide relief
- NSAIDs/oral analgesics - may provide some relief (though evidence shows little superiority over placebo)
- Corticosteroid injection - effective; provides meaningful relief in mild-moderate CTS, may delay surgery by 1 year. Methylprednisolone injection is most commonly used.
- 5% dextrose injection - emerging evidence for temporary relief
Most patients respond well to conservative measures, but symptom recurrence within 1 year is common.
Step 2 - Surgical (Moderate to Severe / Failed Conservative Rx)
Indications:
- Significant motor or sensory deficit
- Thenar muscle atrophy
- Failure of 4-6 months of conservative therapy
- Recurrent symptoms
Techniques:
- Open carpal tunnel release - incision over palm, divides the transverse carpal ligament
- Endoscopic carpal tunnel release - generally preferred; shorter recovery, less pillar pain, equivalent long-term outcomes to open technique
- Ultrasound-guided percutaneous release - newer minimally invasive approach
Surgical outcomes are excellent, with high rates of symptom resolution.
Special Populations
Pregnancy: CTS is common during pregnancy (fluid retention increases tunnel pressure). Usually resolves after delivery; splinting and conservative measures preferred. Surgery rarely needed.
Children: CTS is unusual; predisposing factors include congenital bone abnormalities, hypothyroidism, and lysosomal storage diseases.
Recent Evidence (2024-2025)
A 2025 systematic review and network meta-analysis (PMID 40315975) compared conservative treatments for CTS, and a 2025 network meta-analysis (PMID 39894044) examined ultrasound-guided nerve hydrodissection as a management option - reflecting growing interest in image-guided interventions as alternatives to both traditional steroid injection and surgery.
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 4502-4503
- Goldman-Cecil Medicine, p. 4088
- Bradley & Daroff's Neurology in Clinical Practice, p. 549
- Textbook of Family Medicine 9e, p. 821
This is a shared conversation. Sign in to Orris to start your own chat.