Explain myocardial infraction ecg changes and ecg images simply and clearly
Reading File
Finding Sources
Searching Images
myocardial infarction ECG changes STEMI ST elevation
Finding Sources
Searching Images
ECG evolutionary changes myocardial infarction hyperacute T wave Q wave
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content and images. Here is a clear, well-organized explanation:
Myocardial Infarction (MI) — ECG Changes Explained Simply
What's Happening in the Heart
A heart attack (MI) occurs when a coronary artery is suddenly blocked. The heart muscle downstream stops getting oxygen. This disrupts the electrical activity of those cells, and the ECG captures these changes in a predictable sequence over time.
The 3 Main ECG Changes (in order of appearance)
1. 🔺 Hyperacute T Waves — Minutes after occlusion
The earliest sign. T waves become tall, broad-based, and peaked in the leads overlying the affected area. This happens within minutes of the blood supply being cut off.
Think of it as the heart "shouting" electrically before it starts dying.
2. 📈 ST-Segment Elevation — Minutes to hours
As infarction progresses, the ST segment rises above baseline in the leads facing the damaged zone. This is the hallmark of STEMI (ST-Elevation MI) and indicates full-thickness (transmural) ischemia.
ST elevation morphologies:
- Flat/horizontal → Convex (domed) → "Tombstone" (merges with T wave — most severe)
- Concave ST elevation is more typical of pericarditis, not MI
Why it happens: When transmural (full-wall) ischemia occurs, a "current of injury" flows from the damaged epicardial tissue outward. Leads overlying the area record ST elevation; leads on the opposite wall record reciprocal ST depression.

3. 🕳️ Pathological Q Waves — Hours to days
As myocardial cells die and become electrically silent, the normal depolarization forces disappear. The ECG records the opposite wall's activity unopposed → a deep, wide Q wave appears.
Pathological Q wave criteria: width ≥ 0.04 sec (1 small square) and depth ≥ 25% of the R wave height.
The Full Evolutionary Timeline
| Time | ECG Finding |
|---|---|
| Minutes | Hyperacute T waves (tall, broad, peaked) |
| Minutes–hours | ST elevation (STEMI pattern) |
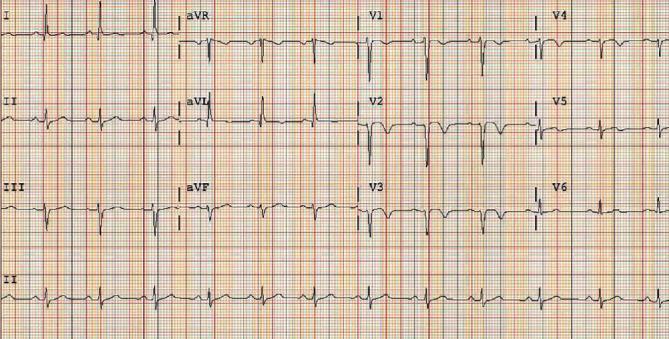
| Hours–days | T-wave inversion develops |
| Hours–days | Pathological Q waves form |
| Days–weeks | ST returns to baseline; deep T inversions |
| Weeks–months | Q waves may persist permanently |
Real ECG Examples
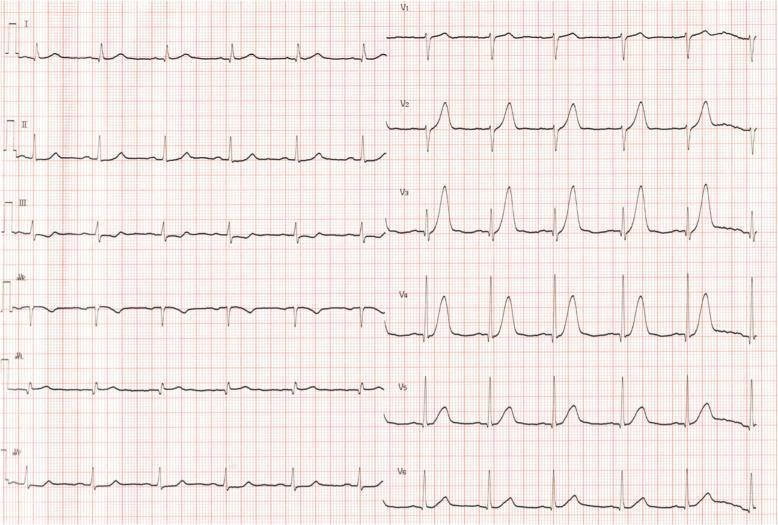
Anterior STEMI (LAD occlusion)

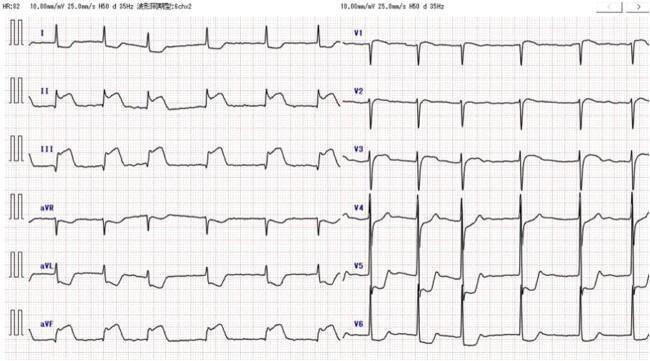
Inferior STEMI (RCA or LCx occlusion)
Subacute/Evolved Anterior MI (days later)
Lead Localization: Which Territory?
| Leads with ST Elevation | Wall Affected | Artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| V1–V6 + I, aVL | Anterolateral | Proximal LAD |
| II, III, aVF | Inferior | RCA (or LCx) |
| I, aVL | High lateral | LCx / Diagonal |
| V1–V3 (depression = posterior equivalent) | Posterior | RCA / LCx |
| V4R–V6R (right-sided leads) | Right ventricle | Proximal RCA |
Reciprocal Changes — The Mirror Image
When one wall is damaged (ST elevation), the electrically opposite wall shows ST depression. This is a helpful confirmation sign:
- Anterior STEMI → reciprocal depression in II, III, aVF
- Inferior STEMI → reciprocal depression in I, aVL, and sometimes V1–V4
STEMI vs NSTEMI at a Glance
| STEMI | NSTEMI | |
|---|---|---|
| ST elevation? | ✅ Yes | ❌ No |
| Troponin rise? | ✅ Yes | ✅ Yes |
| Q waves? | Often develop | Usually absent |
| Occlusion type | Complete | Partial |
| Urgency | Immediate PCI | Urgent/semi-urgent |
Special ECG Patterns Worth Knowing
- Wellens sign: Deep symmetric T inversions in V1–V4 → critical LAD stenosis (not full occlusion yet — a warning sign)
- De Winter pattern: ST depression + tall T waves in precordial leads + ST elevation in aVR → proximal LAD occlusion (STEMI equivalent)
- ST elevation in aVR: Suggests left main coronary artery disease or severe multivessel disease
Sources: Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.