Vomiting evaluation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive content from multiple authoritative sources. Let me compile the full evaluation.
Vomiting — Clinical Evaluation
Definition & Physiology
Vomiting is the forceful expulsion of gastric contents through the mouth, coordinated by the vomiting center in the medullary reticular formation. It proceeds through three sequential phases:
- Nausea — increased duodenal/jejunal tone, decreased gastric tone → intestinal contents reflux into stomach; associated with hypersalivation and tachycardia
- Retching — rhythmic, synchronous contraction of diaphragm, abdominal muscles, and intercostal muscles against a closed glottis, without expulsion
- Vomiting — contraction of external oblique and rectus abdominis + relaxation of hiatal diaphragm → increased thoracoabdominal pressure; simultaneous relaxation of gastric fundus, cardia, and upper esophageal sphincter; glottis closes to prevent aspiration
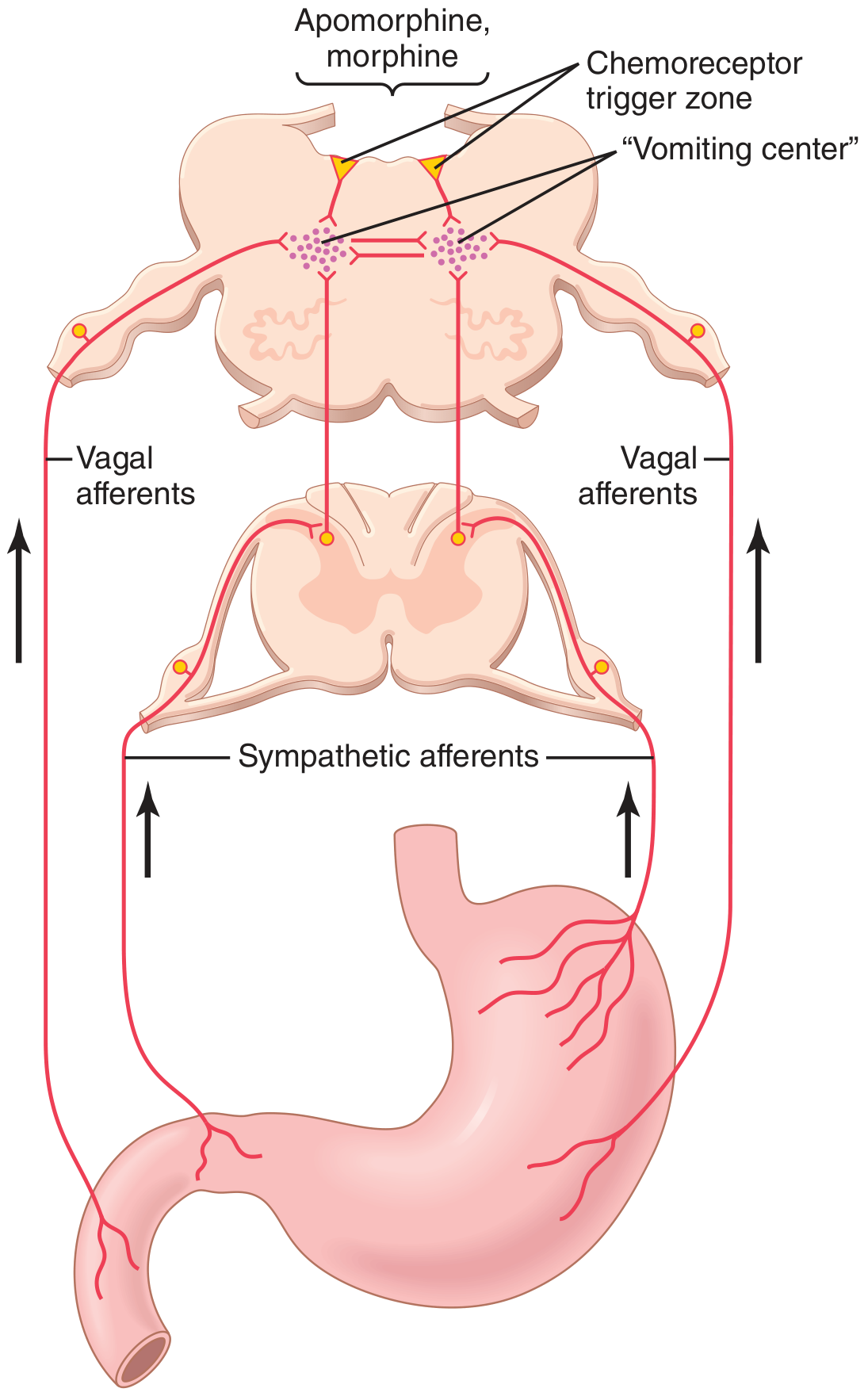
Figure: The vomiting center (medullary/pontine reticular formation) receives input from vagal and sympathetic afferents from the GI tract and from the chemoreceptor trigger zone (CTZ) in the area postrema. — Guyton & Hall Medical Physiology
Afferent Inputs to the Vomiting Center
| Source | Examples |
|---|---|
| GI visceral afferents (vagal/sympathetic) | Gastric distension, irritation, duodenal stimuli |
| Extra-GI visceral afferents | Biliary system, peritoneum, pharynx, genitalia, heart (e.g., MI) |
| CNS/cortical afferents | Vestibular system, thalamus, cerebral cortex |
| Chemoreceptor trigger zone (CTZ) | Area postrema, floor of 4th ventricle — partially outside the blood-brain barrier; responds to drugs (morphine, digoxin, apomorphine, chemotherapy), toxins, metabolic derangements |
The CTZ is rich in dopamine D2 and serotonin (5-HT3) receptors; the lateral vestibular nucleus is rich in cholinergic and histamine receptors — these are targets for antiemetic therapy.
History
Characterize the Vomiting
| Feature | Clinical significance |
|---|---|
| Timing/onset | Acute (<1 week) vs. chronic (>1 month) |
| Relationship to meals | Immediately post-prandial → gastric outlet obstruction or pyloric stenosis; early morning → pregnancy, raised ICP, uremia |
| Frequency and volume | Copious/frequent → obstruction |
| Effortless/projectile | Projectile without nausea → CNS etiology (raised ICP) |
| Relief with vomiting | Relieves pain in PUD and bowel obstruction; no relief in inflammatory conditions (cholecystitis, pancreatitis) |
Characteristics of the Vomitus
| Vomitus Appearance | Suggested Diagnosis |
|---|---|
| Bright red blood | Peptic ulcer, gastritis, esophageal varices, Mallory-Weiss tear, Dieulafoy lesion, aortoenteric fistula |
| Coffee-ground | Any upper GI bleed; Hgb → hematin via gastric acid; also iron tablets, red wine |
| Undigested food | Gastric outlet obstruction, achalasia, esophageal stricture/atresia |
| Bilious (yellow-green) | Obstruction distal to ampulla of Vater |
| Feculent (brown, fecal odor) | Advanced low small bowel or large bowel obstruction |
| True feces | Gastrocolic fistula |
Associated Symptoms
- Diarrhea + fever + myalgias → infectious gastroenteritis
- Headache + visual changes + neck stiffness → CNS etiology (meningitis, raised ICP, intracranial mass)
- Nystagmus + vertigo + tinnitus → vestibular/labyrinthine disease
- Abdominal pain → obstruction, PUD, cholecystitis, pancreatitis, appendicitis
- Chest pain → myocardial infarction (especially inferior MI), esophageal rupture
- Dysphagia → esophageal disease
- Jaundice → hepatobiliary disease
- Episodic with hot-shower relief + cannabis use → cannabinoid hyperemesis syndrome (CHS)
Differential Diagnosis by Category
GI Causes
- Gastroenteritis (most common, usually viral/self-limited)
- Peptic ulcer disease / gastritis
- Gastric outlet obstruction (pyloric stenosis, malignancy)
- Intestinal obstruction (adhesions, hernia, volvulus, intussusception)
- Acute cholecystitis, cholelithiasis
- Acute pancreatitis
- Hepatitis
- Achalasia / esophageal stricture
- Gastroparesis
Neurologic / CNS
- Meningitis
- Intracranial hypertension (tumor, hydrocephalus, hemorrhage)
- Migraine
- Labyrinthitis / vestibular neuritis / motion sickness
- Post-concussion syndrome
Metabolic / Endocrine
- Diabetic ketoacidosis
- Renal failure (uremia)
- Adrenal insufficiency
- Hyperparathyroidism / hypercalcemia
- Hypo/hyperthyroidism
Drugs & Toxins
- Opioids (morphine, codeine)
- Digoxin toxicity
- Chemotherapy
- NSAIDs
- Alcohol
Obstetric
- Pregnancy (hyperemesis gravidarum)
Cardiac
- Inferior/posterior myocardial infarction
Other
- Cyclical vomiting syndrome (CVS) — episodic, migraine-associated
- Cannabinoid hyperemesis syndrome (CHS)
- Psychogenic / bulimia nervosa
- Post-operative nausea and vomiting (PONV)
Age-Based Consideration (Pediatric)
| Age | Priority Diagnoses |
|---|---|
| Newborn | Esophageal/intestinal atresia, malrotation ± volvulus, Hirschsprung's, metabolic disorders, sepsis |
| Infant (<12 mo) | Pyloric stenosis, intussusception, GERD, UTI, meningitis |
| Child (>12 mo) | Gastroenteritis, intussusception, migraine, appendicitis, intracranial mass |
Bilious or bloody vomitus, hematochezia, or significant abdominal pain should trigger concern for diagnoses beyond simple viral gastroenteritis. — Tintinalli's Emergency Medicine
Physical Examination
| System | Finding | Suggested Diagnosis |
|---|---|---|
| General | Poor skin turgor, dry mucous membranes | Dehydration |
| Vital signs | Fever | Gastroenteritis, cholecystitis, appendicitis, peritonitis |
| Vital signs | Tachycardia + orthostatic changes | Dehydration/volume depletion |
| Eyes | Nystagmus | Labyrinthitis, vertebrobasilar insufficiency, cerebellar infarct/bleed, drug intoxication |
| Eyes | Papilledema | Raised ICP (CNS tumor, bleed) |
| Neck | Goiter | Thyroid disease |
| Lungs | Rales | Pneumonia |
| Abdomen | Distension, high-pitched bowel sounds | Obstruction |
| Abdomen | RUQ tenderness + Murphy's sign | Cholecystitis |
| Abdomen | Rigidity/guarding | Peritonitis, perforation |
| Oral | Loss of dental enamel | Bulimia nervosa |
Complications of Vomiting
- Metabolic alkalosis with hypochloremia and hypokalemia (from loss of H⁺ and Cl⁻)
- Dehydration and electrolyte disturbances
- Mallory-Weiss tear — mucosal laceration at gastroesophageal junction from violent retching
- Boerhaave syndrome — full-thickness esophageal rupture → mediastinitis/peritonitis (life-threatening)
- Aspiration pneumonitis — in patients with impaired consciousness
- Malnutrition / weight loss
- Wernicke encephalopathy — in prolonged vomiting (thiamine depletion)
- Bezoar formation in severe gastroparesis
Diagnostic Workup
Guided by history and physical; no single test is universally indicated.
| Test | Indication |
|---|---|
| BMP/electrolytes, BUN, Cr | Assess dehydration, metabolic alkalosis, renal failure |
| CBC | Infection, anemia |
| LFTs, lipase | Biliary/pancreatic disease |
| Urine hCG | Any woman of reproductive age |
| Urinalysis | UTI, renal disease |
| Blood glucose | DKA |
| Upright CXR / AXR | Free air (perforation), obstruction (air-fluid levels), pneumonia |
| CT abdomen/pelvis | Obstruction, appendicitis, pancreatitis, mass |
| Head CT / MRI | Suspected CNS etiology |
| Upper endoscopy | Chronic vomiting, hematemesis, suspected mucosal disease |
| Gastric emptying scan | Suspected gastroparesis |
Management
Immediate Priorities
- Assess and protect the airway (especially in altered consciousness)
- Assess hemodynamic status and volume depletion → IV crystalloid if severe
- Hold oral medications; find parenteral substitutes as needed
- Consider nasogastric tube if obstruction or high-output vomiting
Antiemetics
| Drug | Class | Mechanism | Dose | Notes |
|---|---|---|---|---|
| Ondansetron | 5-HT3 antagonist | CTZ + vagal GI terminals | 4–8 mg IV/PO | First-line; generally well-tolerated |
| Metoclopramide | D2/5-HT2 antagonist | CTZ + gastric motility | 10–20 mg IM/IV q6h | Risk of tardive dyskinesia (black box) |
| Prochlorperazine | D1/D2 antagonist | CTZ | 5–10 mg IM/PO; 25 mg PR | Extrapyramidal effects |
| Droperidol / Haloperidol | D2 antagonist | CTZ | 1.25 / 5 mg IV | QT prolongation monitoring |
| Promethazine | H1/muscarinic antagonist | Vestibular nucleus | 12.5–25 mg IM/IV | Sedating; IV route → tissue necrosis risk |
| Dimenhydrinate | H1 antagonist | Vestibular nucleus | 25–50 mg PO/IV | Motion sickness |
| Dexamethasone | Corticosteroid | CNS/undefined | 4–8 mg IV | PONV, chemotherapy-induced |
| Aprepitant | NK1 antagonist | Substance P/CTZ | 40–125 mg PO | PONV, chemotherapy |
| Scopolamine | Muscarinic antagonist | Vestibular nucleus | 1.5 mg patch | Motion sickness |
ED stepwise approach (Rosen's Emergency Medicine):
- Ondansetron 4 mg IV → repeat after 15–30 min if needed
- Add metoclopramide 10 mg IV if inadequate
- Consider droperidol 1.25 mg IV or haloperidol 5 mg IV (if mechanical obstruction excluded)
- Prochlorperazine 10 mg IV or promethazine 12.5 mg IM/IV if above fail
Special Situations
- Cannabinoid hyperemesis syndrome: cessation of cannabis (definitive); acute — capsaicin cream topically, haloperidol, or lorazepam; hot showers provide temporary relief
- Post-operative vomiting: aprepitant, ondansetron, dexamethasone, droperidol (combination additive); rule out anastomotic leak, ileus
- Pregnancy (hyperemesis gravidarum): pyridoxine (B6) ± doxylamine first-line; ondansetron second-line; IV fluids, thiamine supplementation
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Guyton & Hall Textbook of Medical Physiology; Yamada's Textbook of Gastroenterology; S. Das Manual on Clinical Surgery; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.