Michel and mondini dysplasia for ms ent pg exam
Reading File
Finding Sources
Finding Sources
Searching the Web
Michel and Mondini dysplasia inner ear ENT PG exam key points
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the material needed. Here is a complete, exam-oriented answer:
Michel Aplasia & Mondini Dysplasia - MS ENT PG Exam Notes
Overview: Classification of Inner Ear Malformations
Inner ear malformations are responsible for ~20% of congenital SNHL. The classic classification (Jackler) divides them into two broad groups:
Malformations limited to membranous labyrinth (bony labyrinth normal, >90% of congenital deafness):
- Scheibe (cochleosaccular dysplasia) - most common
- Siebenmann-Bing (complete membranous dysplasia)
- Alexander (basal turn dysplasia)
Malformations of osseous + membranous labyrinth (radiologically detectable):
- Michel aplasia (complete labyrinthine aplasia)
- Cochlear aplasia
- Cochlear hypoplasia
- Incomplete partition (Mondini)
- Common cavity
Incidence of Cochlear Malformations (Cummings Table 194.1)
| Malformation | Incidence |
|---|---|
| Incomplete partition / Mondini dysplasia | 55% (most common) |
| Common cavity | 26% |
| Cochlear hypoplasia | 15% |
| Cochlear aplasia | 3% |
| Michel aplasia | 1% (most severe, rarest) |
MICHEL APLASIA (Complete Labyrinthine Aplasia)
Key Facts
- First described by: Michel (1863)
- Developmental arrest: before 3rd gestational week (before otic vesicle formation)
- Result: Complete absence of all inner ear structures - cochlea, vestibule, semicircular canals; the otic capsule is entirely absent
- The petrous bone itself is aplastic/severely malformed
- External ear and middle ear may be unaffected
- Inheritance: Autosomal dominant (AD); recessive also possible
Pathology
- No otic vesicle forms; the entire membranous and osseous labyrinth is absent
- Associated with anencephaly and thalidomide exposure
Radiology (HRCT temporal bone)
- Complete absence of the otic capsule on axial and coronal cuts
- External auditory canal and middle ear may appear normal
- Must differentiate from labyrinthine ossification (ossification shows a dense otic capsule of normal dimensions; aplasia shows no capsule)
Hearing
- Profound anacusis (total deafness) - bilateral
- Conventional hearing aids: no benefit
- Cochlear implant: NOT a candidate (no cochlea or nerve to stimulate)
- Vibrotactile devices: beneficial in some patients
MONDINI DYSPLASIA (Incomplete Partition / IP-II)
Key Facts
- First described by: Carlo Mondini (1791) - in a young deaf man who had died of gangrene
- Developmental arrest: 6th-7th week of gestation
- Most common radiologically detectable cochlear malformation (~55%)
- Inheritance: Autosomal dominant; may be unilateral
The Classic Mondini Triad (IP-II)
- Cochlea with only 1.5 turns (normal = 2.5 turns) - basal coil is normal; middle and apical coils fuse into a single cystic apex (scala communis / apical scala communis)
- Dilated/enlarged vestibule (minimal dilation)
- Enlarged vestibular aqueduct (EVA)
Pathology
- Only the basal coil is clearly identifiable
- Absence/deficiency of the osseous spiral lamina and interscalar septum at the apex
- Endolymphatic duct is usually enlarged
- Abnormal communication between endolymphatic/perilymphatic spaces and subarachnoid space (via cribriform area of the lateral IAC) - predisposes to perilymphatic fistula
Radiology (HRCT)
- Cochlea smaller than normal: 5-6 mm (normal 8-10 mm vertically)
- Absence of interscalar septum - the key radiological feature (not just counting turns, as coronal CT can make a normal cochlea appear to have only 1.5 turns due to the oblique angle)
- Dilated vestibular aqueduct (>1.5 mm at midpoint - Valvassori criteria)
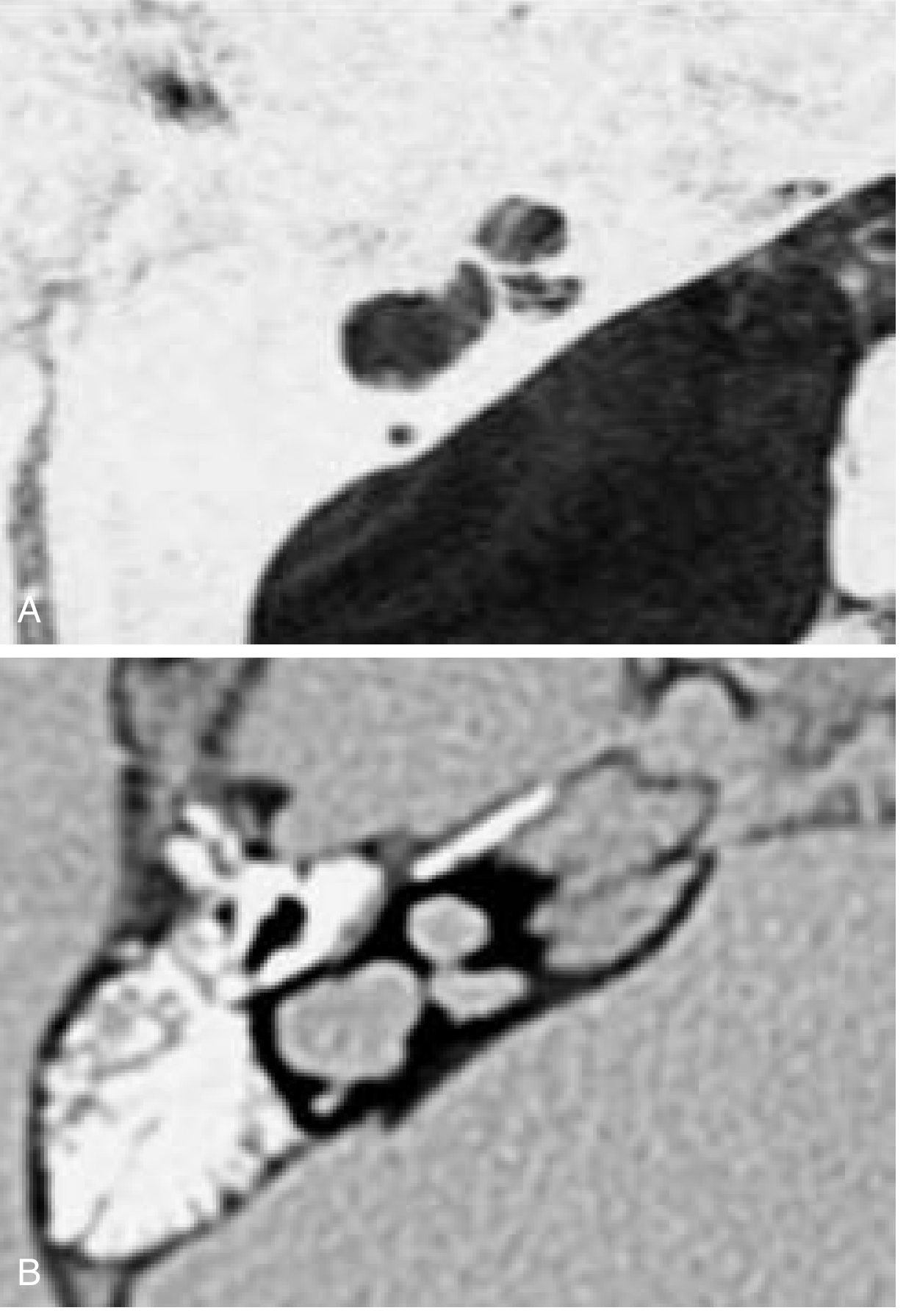
Cummings Otolaryngology, Fig. 194.8 - Incomplete partition (Mondini): axial MRI (A) and CT (B) showing absence of interscalar septum
Hearing
- Variable SNHL - may range from mild to profound
- Some residual hearing is common (neurosensory structures are present in most cases)
- Early hearing rehabilitation is indicated
- Cochlear implant: CANDIDATE - but with important surgical caveats
Associated Syndromes
- Pendred syndrome (most important association - goiter + SNHL + EVA + Mondini)
- Waardenburg syndrome
- Treacher Collins syndrome
- Wildervanck syndrome
- CHARGE association (Mondini-type deformity + absent semicircular canals + coloboma + heart disease + choanal atresia + retarded growth + genital hypoplasia + ear anomalies)
- Congenital CMV infection (accounts for >40% of deafness of unknown etiology)
Incomplete Partition Subtypes (Sennaroglu Classification)
| Type | Description | Key Features |
|---|---|---|
| IP-I | Cystic cochlea-vestibular anomaly | No modiolus, no interscalar septa; cystic cochlea + dilated vestibule; NO EVA |
| IP-II | Classic Mondini | 1.5 turns, absent apical interscalar septum, dilated vestibule + EVA |
| IP-III | X-linked deafness | Interscalar septa present but NO modiolus; associated with X-linked DFNX2 (SLC17A8) |
Comparison: Michel vs. Mondini (High-Yield for MCQs)
| Feature | Michel Aplasia | Mondini Dysplasia |
|---|---|---|
| Described by | Michel (1863) | Carlo Mondini (1791) |
| Developmental arrest | <3rd week (before otic vesicle) | 6th-7th week |
| Cochlea | Completely absent | 1.5 turns (basal coil present) |
| Vestibule/SCCs | Absent | Mildly dilated vestibule |
| Vestibular aqueduct | Absent | Enlarged (EVA) |
| Otic capsule | Absent on CT | Present |
| Incidence | 1% (rarest) | 55% (most common) |
| Hearing | Anacusis | Variable SNHL |
| CI candidacy | No | Yes (with precautions) |
| CSF gusher risk | N/A | Yes (perilymphatic-CSF communication) |
Surgical Pearls (Cochlear Implant in Mondini)
- CSF gusher is the major intraoperative hazard - due to abnormal CSF-perilymph communication through the cribriform plate defect in the IAC
- Higher risk of meningitis with or without CI
- MRI pre-op is mandatory to confirm cochlear nerve presence
- An absent cochlear nerve is an absolute contraindication for CI
- Consider short/compressed electrode arrays; insertion may be difficult
Memory Aids
- Michel = Most severe, Missing everything (no inner ear at all) - arrest before 3rd week
- Mondini = Most common cochlear malformation, 1.5 turns - arrest at 6-7th week
- Mondini triad: 1.5 turns + dilated vestibule + EVA (Pendred syndrome is the most tested association)
- Scheibe = most common of ALL congenital deafness (membranous only, normal bony labyrinth)
Sources: Cummings Otolaryngology Head and Neck Surgery, 7th ed., Ch. 194; KJ Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology, Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.