Metronidazole c/I in chronic alcoholics
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Here is a complete answer based on authoritative textbook sources:
Metronidazole - Contraindication in Chronic Alcoholics
The Core Reason: Disulfiram-like Reaction
Metronidazole inhibits aldehyde dehydrogenase (ALDH), the mitochondrial enzyme responsible for oxidizing acetaldehyde (the toxic intermediate of ethanol metabolism) to acetate.
Normal ethanol metabolism:
Ethanol → Acetaldehyde → Acetate (via ALDH)
When metronidazole blocks ALDH, acetaldehyde accumulates - exactly as happens with disulfiram (Antabuse). This produces a highly unpleasant and potentially dangerous reaction.
Features of the Disulfiram-like Reaction
When a patient on metronidazole ingests alcohol:
| Symptom | Mechanism |
|---|---|
| Facial flushing | Vasodilation from acetaldehyde |
| Nausea & vomiting | Toxic acetaldehyde effect |
| Headache | Vasodilation |
| Dizziness | Hypotension |
| Tachycardia | Compensatory |
| Hypotension | Can be severe / fatal in extreme cases |
Described by Goldman-Cecil Medicine as "potentially severe disulfiram-like reactions" in patients ingesting alcohol while taking metronidazole.
Why It Matters in Chronic Alcoholics
- Chronic alcoholics are likely to continue consuming alcohol, even during a course of antibiotics.
- They may not reliably comply with alcohol abstinence advice.
- Even topical/vaginal formulations warrant caution.
- Per Rosen's Emergency Medicine: patients should avoid alcohol for at least 24 hours after completing metronidazole (72 hours for tinidazole).
Additional CNS Concerns in Chronic Alcoholics
Metronidazole also carries independent CNS adverse effects - peripheral neuropathy, encephalopathy, and seizures (Washington Manual of Medical Therapeutics). Chronic alcoholics already have compromised neurological status (Wernicke's, alcoholic neuropathy), making these risks additive.
Mechanism (Molecular Detail)
Metronidazole (like cefotetan and trimethoprim) inhibits mitochondrial ALDH. The mechanism is described as "not established" for metronidazole specifically - it may differ from disulfiram's direct ALDH blockade - but the clinical outcome (acetaldehyde accumulation) is the same.
Katzung's Basic and Clinical Pharmacology, 16th Ed - "Several other drugs (eg, metronidazole, cefotetan, trimethoprim) inhibit ALDH and have been claimed to cause a disulfiram-like reaction if combined with ethanol."
Key Points for Exams
- Metronidazole c/I with alcohol = disulfiram-like reaction (acetaldehyde accumulation)
- Mechanism = ALDH inhibition
- Features = flushing, N/V, headache, hypotension, tachycardia
- Avoid alcohol for 24 hours post-metronidazole
- Other drugs with same property: cefotetan, tinidazole, trimethoprim, chlorpropamide, moxalactam
Malaria prototype drug
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Chloroquine - Prototype Antimalarial Drug
Classification
Chloroquine is the prototype antimalarial drug - a synthetic 4-aminoquinoline, used as the standard against which all other antimalarials are compared.
Katzung's Basic and Clinical Pharmacology, 16th Ed - "Chloroquine has been a drug of choice for both treatment and chemoprophylaxis of malaria since the 1940s."
Mechanism of Action
The mechanism centers on inhibition of heme polymerization in the parasite's food vacuole:
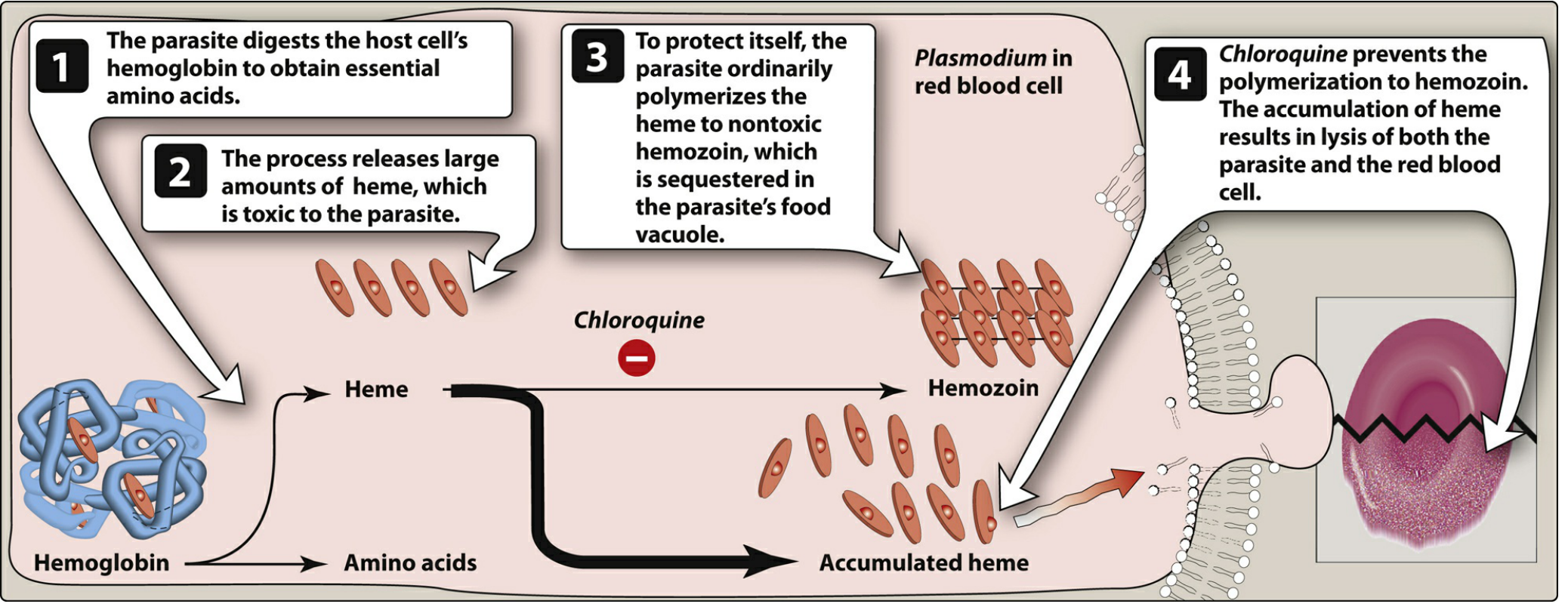
Step by step:
- The malarial parasite digests host RBC hemoglobin to get essential amino acids
- This releases large amounts of free heme - which is toxic to the parasite
- Normally, the parasite polymerizes heme into non-toxic hemozoin (malaria pigment), sequestered in the food vacuole
- Chloroquine (a diprotic weak base) concentrates in the acidic food vacuole by ion trapping, and binds to heme - blocking its polymerization to hemozoin
- Free heme accumulates → oxidative damage to parasite membranes → lysis of both the parasite and the RBC
Type of Activity (Schizonticide)
| Activity | Details |
|---|---|
| Blood schizonticide | Primary action - kills erythrocytic stages |
| NOT hypnozoiticide | Does NOT kill dormant liver stages (hypnozoites) of P. vivax / P. ovale |
| NOT gametocytocidal | Not reliably active against gametocytes |
For radical cure of P. vivax / P. ovale, primaquine or tafenoquine must be added to eliminate hepatic stages.
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Rapid, almost complete after oral dosing; peak in ~3 hours |
| Distribution | Very large Vd (100-1000 L/kg); concentrates in erythrocytes, liver, spleen, kidney, lung, melanin-containing tissues |
| Half-life | Initial: 3-5 days; terminal: 1-2 months (very long) |
| Excretion | Predominantly urine |
| CNS penetration | Yes; also crosses the placenta |
Clinical Uses
- Treatment of uncomplicated malaria due to chloroquine-sensitive strains (P. vivax, P. ovale, P. malariae, sensitive P. falciparum)
- Clears fever in 24-48 hours; clears parasitemia in 48-72 hours
- Chemoprophylaxis in areas without chloroquine-resistant falciparum
- Amebic liver abscess (alternative when metronidazole fails - reaches high liver concentrations)
- Rheumatoid arthritis / SLE (hydroxychloroquine more commonly used)
Resistance
- Chloroquine resistance is now very common in P. falciparum, uncommon but rising in P. vivax
- Mechanism: mutations in PfCRT (P. falciparum chloroquine resistance transporter) - allows the parasite to pump chloroquine out of the food vacuole
- Resistance reversers: verapamil, desipramine, chlorpheniramine (no established clinical role)
- In most endemic regions, artemisinin-based combination therapy (ACT) has replaced chloroquine for falciparum malaria
Adverse Effects
| Severity | Effect |
|---|---|
| Common (low doses) | Pruritus (especially in Africans), mild GI upset |
| Higher doses | Nausea/vomiting, headache, blurred vision, urticaria |
| Rare | Hemolysis (G6PD deficiency), hearing loss, psychosis, seizures, QT prolongation |
| Long-term high dose | Retinopathy (irreversible), myopathy, peripheral neuropathy, ototoxicity |
| IV/IM route | Severe hypotension, cardiac/respiratory arrest - AVOID |
Contraindications
- Psoriasis (may precipitate acute attack)
- Porphyria (may precipitate acute attack)
- Retinal / visual field abnormalities
- Pre-existing myopathy
Safe in pregnancy and young children.
Exam Highlights
- Prototype drug for malaria = Chloroquine
- Class = 4-aminoquinoline
- MOA = Inhibits heme → hemozoin polymerization (heme accumulates → parasite lysis)
- Type = Blood schizonticide (not hypnozoiticide, not gametocytocidal)
- Key ADR = Retinopathy (long-term), pruritus (Africans), QT prolongation
- Resistance gene = PfCRT mutation
- Add primaquine for P. vivax/P. ovale radical cure
This is a shared conversation. Sign in to Orris to start your own chat.