One bone + One joint + One X-ray + One clinical case Example: Today: Femur anatomy Hip joint Femoral neck fracture X-ray Case discussion Make me so that I can make my ortho very strong, make me perfect detailed notes
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the material needed to build comprehensive notes. Let me compile the complete Day 1 Ortho notes:
🦴 ORTHO DAY 1 - FEMUR + HIP JOINT + FEMORAL NECK FRACTURE X-RAY + CLINICAL CASE
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, Rockwood & Green's Fractures in Adults 10th Ed 2025, Grainger & Allison's Diagnostic Radiology, THIEME Atlas of Anatomy, Rosen's Emergency Medicine
PART 1 - THE FEMUR (Bone)
General Facts (High-Yield)
- The femur is the longest, strongest, and heaviest bone in the human body
- It is subjected to forces during powerful muscle contraction and weight transmission
- Structurally, the femoral neck acts as an oblique strut between the pelvis (horizontal beam) and the femoral shaft (vertical beam) - this geometry allows wide range of motion but creates significant shearing forces at the neck
Regional Anatomy
| Region | Bone Type | Clinical Significance |
|---|---|---|
| Femoral head, neck, intertrochanteric | Predominantly cancellous | Less resistant to torsional forces; fractures from low-energy falls |
| Subtrochanteric region, femoral shaft | Cortical | Requires higher force to fracture |
| Distal metaphysis | Cortex thins, bone widens | Resistance to stress decreases |
Parts of the Femur
- Femoral head - 2/3 sphere; covered with articular cartilage except at the fovea capitis (where ligamentum teres attaches)
- Femoral neck - projects superolaterally from shaft; normal neck-shaft angle = 125-135° (coxa vara < 120°, coxa valga > 140°)
- Anteversion angle - femoral neck is anteverted ~10-15° relative to the femoral condyles
- Greater trochanter - attachment of gluteus medius and minimus (key abductors)
- Lesser trochanter - attachment of iliopsoas (main hip flexor)
- Intertrochanteric line (anterior) / Intertrochanteric crest (posterior) - mark the capsular attachment
- Femoral shaft - cylindrical; linea aspera on posterior surface provides attachment for adductors, hamstrings, and vastus muscles
- Distal femur - medial and lateral condyles; adductor tubercle on medial condyle (landmark)
Angulation Angles to Know
| Angle | Normal Value | Deformity if abnormal |
|---|---|---|
| Neck-shaft (collodiaphyseal) angle | 125-135° | Coxa vara (<120°) / Coxa valga (>140°) |
| Anteversion (torsion) | 10-15° | Increased = in-toeing gait |
| Pauwels' angle (fracture line) | - | Type I <30°, II 30-50°, III >50° |
Muscle Compartments of the Thigh
| Compartment | Muscles | Main Action | Nerve |
|---|---|---|---|
| Anterior | Quadriceps, sartorius | Knee extension, hip flexion | Femoral nerve (L2-L4) |
| Medial | Adductors, gracilis | Hip adduction | Obturator nerve (L2-L4) |
| Posterior | Hamstrings | Hip extension, knee flexion | Sciatic nerve (L4-S3) |
Blood Supply of the Femur
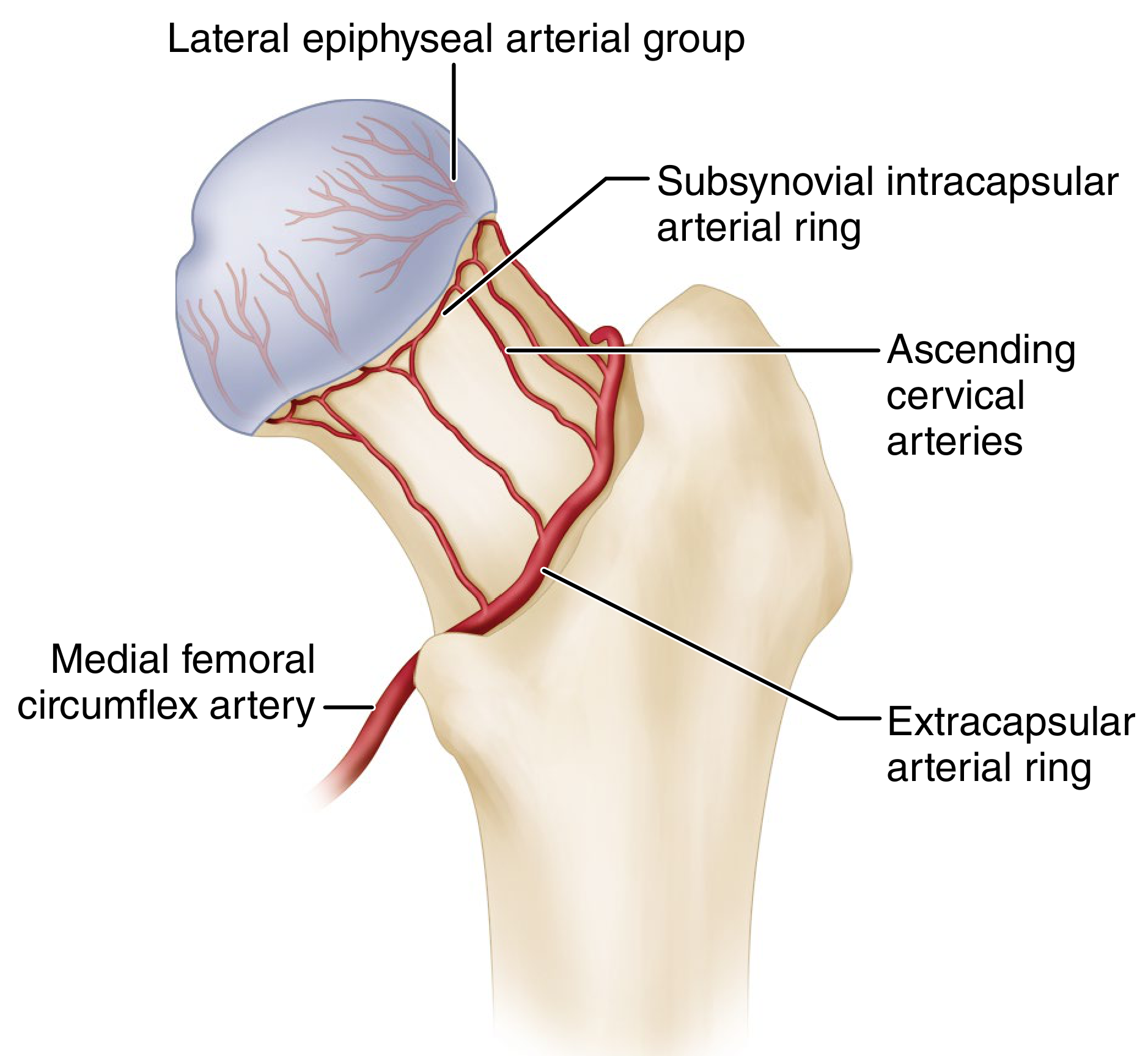
This diagram is THE key to understanding AVN - learn every vessel here.
Main supply to the femoral head:
- Medial femoral circumflex artery (MFCA) - most important; branch of profunda femoris (deep femoral artery). Runs posteriorly and ascends around the femoral neck → forms the extracapsular arterial ring → gives ascending cervical arteries → form subsynovial intracapsular ring → give lateral epiphyseal arterial group (retinacular vessels) which supply the bulk of the femoral head
- Lateral femoral circumflex artery (LFCA) - contributes less; supplies mostly the anterior head
- Artery of ligamentum teres (from obturator artery) - supplies only a small area near the fovea; clinically relevant mainly in children
Why displaced intracapsular fractures = AVN risk:
The ascending cervical / retinacular vessels hug the femoral neck within the capsule. An intracapsular fracture (subcapital especially) or hematoma raises intracapsular pressure → ruptures these vessels → avascular necrosis (15-35% risk with displaced fractures).
PART 2 - THE HIP JOINT (Joint)
Joint Type
- Synovial ball-and-socket joint (enarthrosis)
- Most stable joint in the body due to: deep acetabulum + labrum + strong capsule + powerful muscles
Articular Surfaces
- Femoral head (ball) - fits into the acetabulum
- Acetabulum (socket) - formed by ilium (above), ischium (behind-below), pubis (front-below); covered by lunate surface (horseshoe-shaped articular cartilage); central acetabular fossa is non-articular (contains fat pad and ligamentum teres)
- Acetabular labrum - fibrocartilaginous rim that deepens the acetabulum by ~20%; seals the joint space
Capsule and Ligaments
| Ligament | Origin - Insertion | Function |
|---|---|---|
| Iliofemoral (Y-ligament of Bigelow) | Anterior inferior iliac spine (AIIS) → intertrochanteric line | Strongest ligament in the body; prevents hyperextension; tightens on extension and ER |
| Pubofemoral | Pubic ramus → lower intertrochanteric area | Prevents excessive abduction and extension |
| Ischiofemoral | Ischium → greater trochanter | Winds around neck posteriorly; prevents hyperextension |
| Ligamentum teres | Fovea capitis → acetabular notch | Carries artery of ligamentum teres; minimal mechanical role in adults |
| Transverse acetabular ligament | Bridges acetabular notch | Converts notch into foramen; helps seal joint |
Capsular attachment: Anteriorly at the intertrochanteric line (whole neck is intracapsular anteriorly); Posteriorly it only covers the medial 2/3 of the neck (outer third of posterior neck is EXTRAcapsular - that's where the MFCA is most vulnerable).
Movements and Muscles
| Movement | Range | Prime Mover | Nerve |
|---|---|---|---|
| Flexion | 0-120° (120-135° with knee bent) | Iliopsoas | Femoral + L1-L3 |
| Extension | 0-20° | Gluteus maximus | Inferior gluteal (L5-S2) |
| Abduction | 0-45° | Gluteus medius and minimus | Superior gluteal (L4-S1) |
| Adduction | 0-30° | Adductors | Obturator (L2-L4) |
| Internal rotation | 0-45° | Gluteus medius/minimus (ant fibres), TFL | Superior gluteal |
| External rotation | 0-45° | Deep 6 rotators (piriformis, obturators, gemelli, quadratus femoris) | Multiple |
Trendelenburg Sign (High-Yield)
- Tests gluteus medius (superior gluteal nerve L4-S1)
- Positive sign: when standing on the affected leg, the contralateral pelvis drops (instead of rising)
- Caused by: Superior gluteal nerve palsy, hip pathology, coxa vara, weak abductors
- Walking version = Trendelenburg gait (lurching toward affected side to reduce abductor moment arm)
Neurovascular Relations at the Hip
The femoral triangle contains (lateral to medial: NAVEL):
- Nerve (femoral nerve) - lateral
- Artery (femoral artery) - middle; midpoint between ASIS and pubic symphysis
- Vein (femoral vein) - medial
- Empty space (femoral canal - potential hernia site)
- Lymphatics
PART 3 - X-RAY: FEMORAL NECK FRACTURE
How to Read a Hip X-Ray - Systematic Approach
Radiographic lines to check on every AP pelvis X-ray:
- Shenton's line - smooth arc from inferior femoral neck to inferior pubic ramus. BROKEN in hip dislocation, fractures, developmental dysplasia
- Neck-shaft angle - should be 125-135°
- Trabecular pattern - medial compressive trabeculae / lateral tensile trabeculae of the femoral neck
- Acetabular reference lines - iliopectineal line (anterior column), ilioischial line (posterior column), Köhler's teardrop, acetabular roof
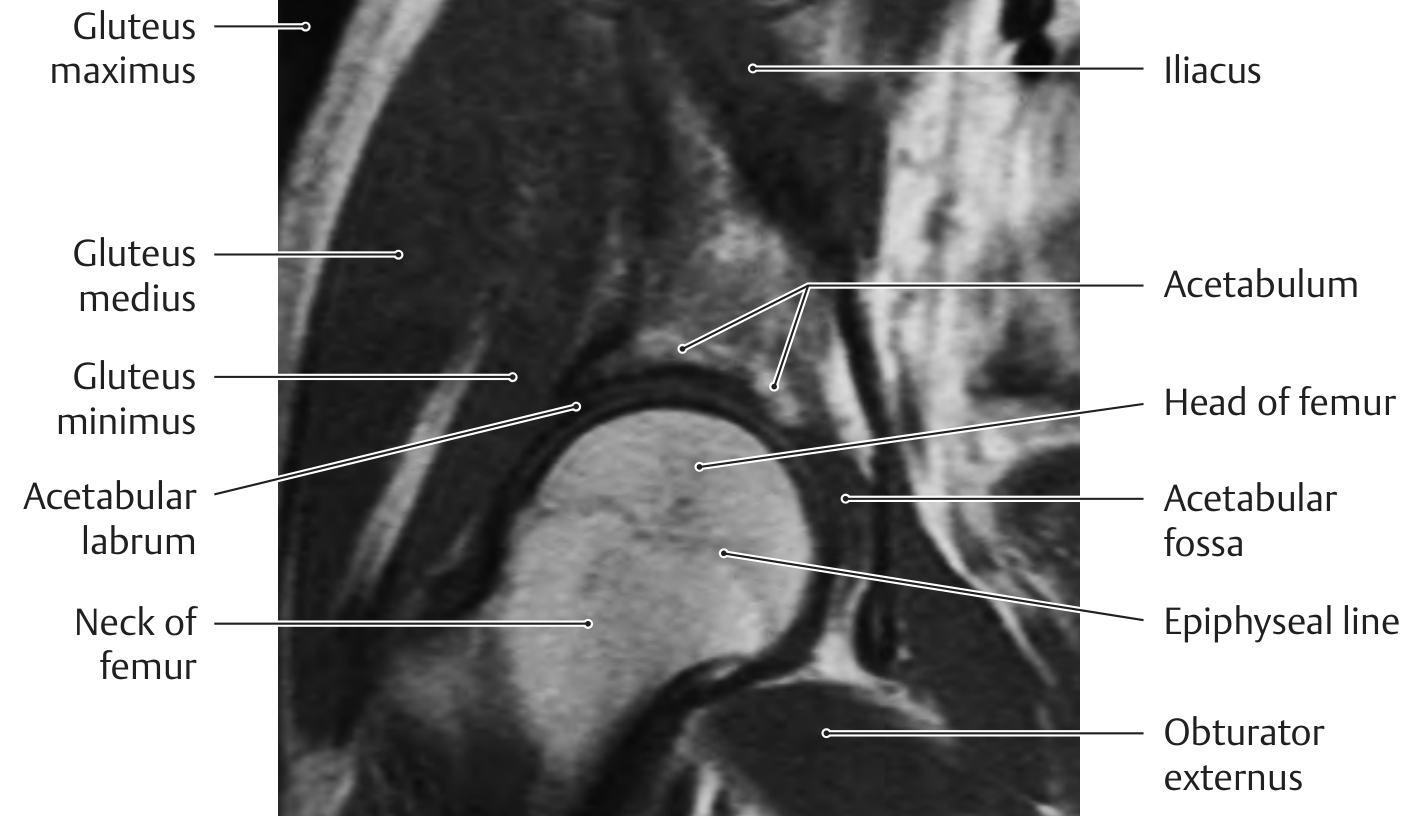
X-Ray Anatomy of the Proximal Femur
Classification of Femoral Neck Fractures
Three systems - know all three:
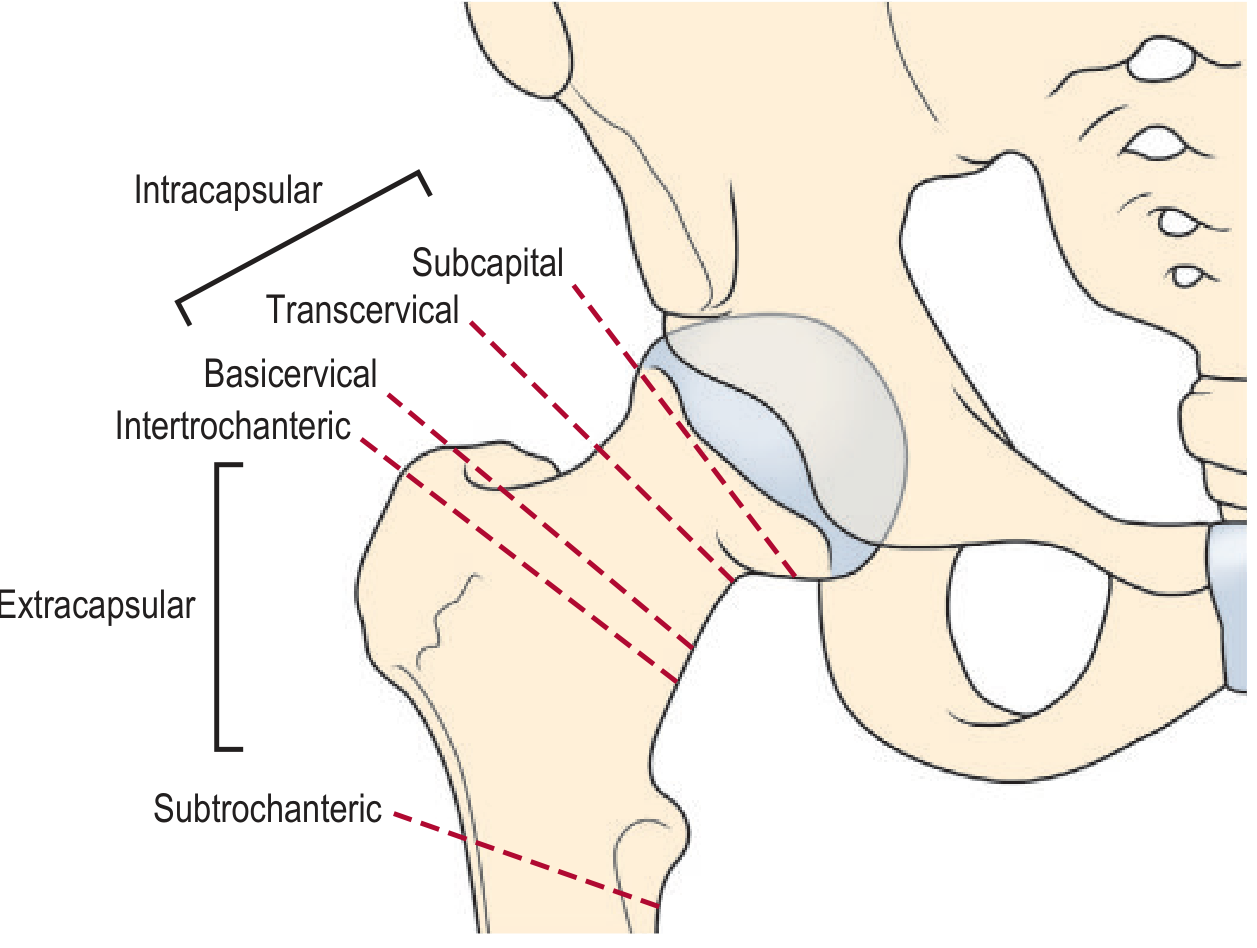
A. By Anatomical Location (most fundamental)
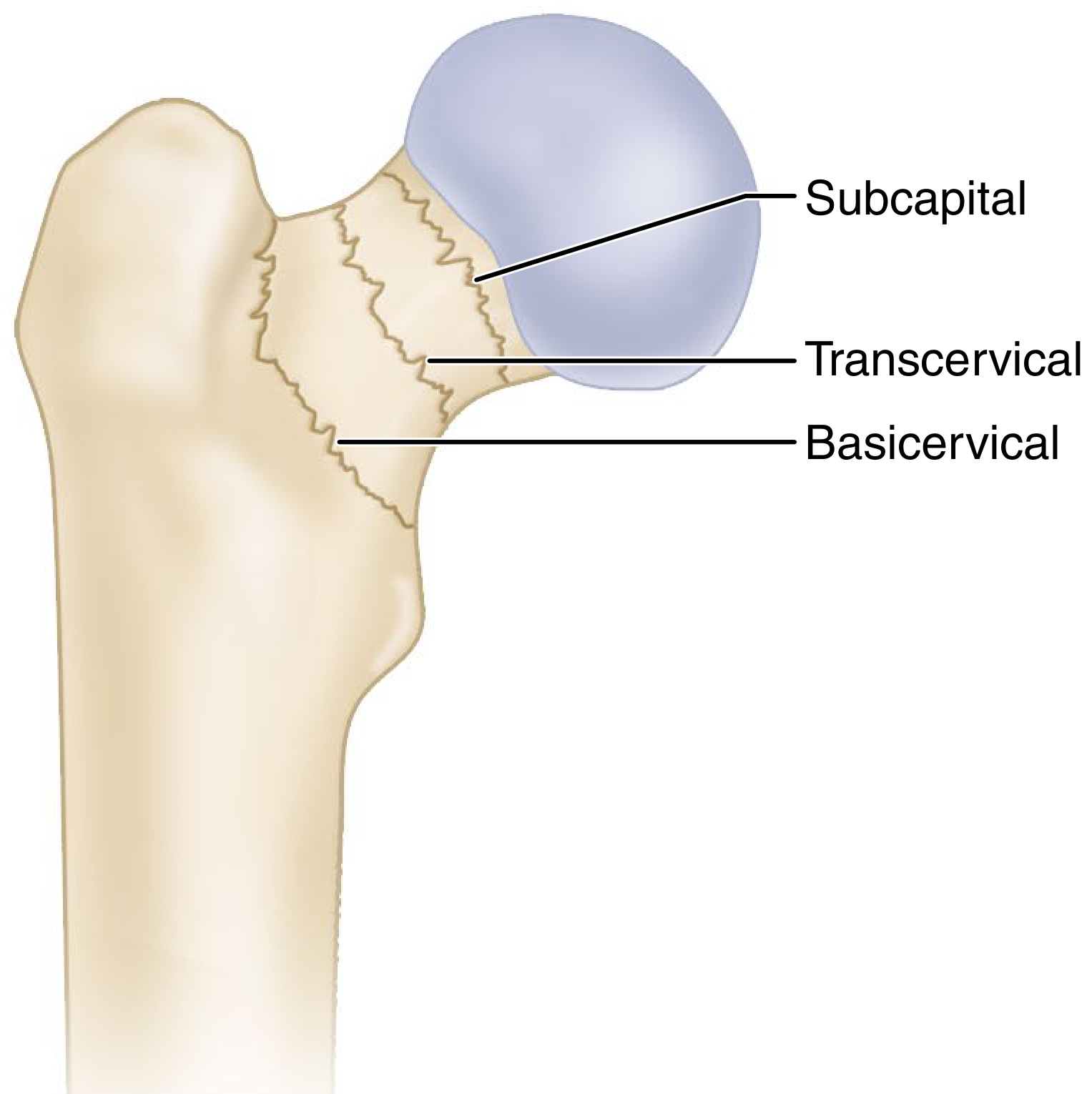
| Location | Intracapsular? | AVN Risk | Common Treatment |
|---|---|---|---|
| Subcapital | Yes | Highest | Hemiarthroplasty / THA (if displaced) |
| Transcervical | Yes | High | Internal fixation (if young/undisplaced) |
| Basicervical | Borderline/No | Lower | Usually fixation with DHS |
| Intertrochanteric | No (extracapsular) | Very low | DHS or IM nail |
| Subtrochanteric | No (extracapsular) | Very low | IM nail (first choice) |
B. Garden Classification (most widely used clinically)
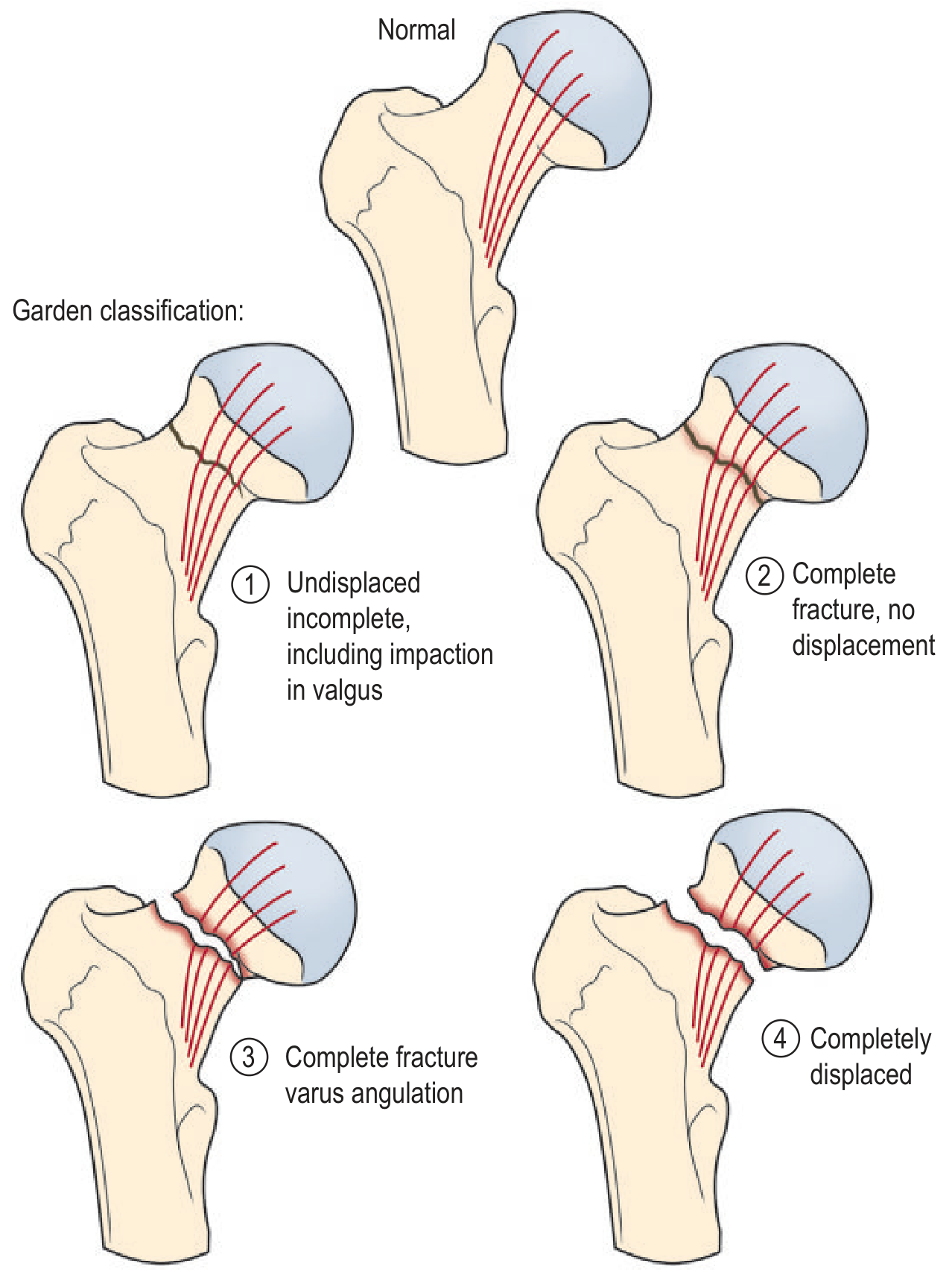
| Stage | Description | Trabecular pattern | Displacement |
|---|---|---|---|
| Garden I | Incomplete (impacted in valgus) | Medial trabeculae angled upward | No displacement - valgus impaction |
| Garden II | Complete fracture, no displacement | Trabeculae still aligned | No displacement |
| Garden III | Complete fracture, partial displacement | Head and neck trabeculae MIS-aligned | Partial - head tilted into varus |
| Garden IV | Complete fracture, full displacement | Trabeculae of head RE-aligned with acetabulum | Full displacement - no contact |
Exam trick for Garden III vs IV:
- Garden III: neck and head still have contact; trabecular lines between head and acetabulum are NOT aligned (head has tilted)
- Garden IV: neck and head have NO contact; BUT trabecular lines between head and acetabulum RE-align (head has rotated back with acetabulum, completely free from neck)
Practical simplification used by most surgeons:
- Garden I + II = Undisplaced → treat with internal fixation
- Garden III + IV = Displaced → treat with arthroplasty (hemi or THA) in elderly
C. Pauwels Classification (based on biomechanics)
| Type | Angle of fracture line to horizontal | Forces | Stability |
|---|---|---|---|
| Type I | 0-30° | Compressive - good for healing | Most stable |
| Type II | 30-50° | Mixed compressive and shear | Intermediate |
| Type III | >50° | Predominantly shear | Unstable - highest risk of nonunion |
Steeper fracture line = more shear = higher risk of fixation failure and nonunion.
What to Look for on the X-Ray (Checklist)
- Is the fracture intracapsular or extracapsular?
- Is there displacement? (Is Shenton's line broken?)
- What is the neck-shaft angle? (Varus = displaced)
- Are trabecular lines aligned in the femoral head vs acetabulum? (Garden grading)
- What is the Pauwels angle?
- Is there associated fracture (acetabulum, shaft, pelvis)?
- Any signs of pre-existing pathology (Paget disease, metastasis, osteoporosis)?
If plain X-ray is normal but clinical suspicion is high:
- ~15% of femoral neck fractures are radiographically occult on plain film
- MRI is the gold standard for occult fractures (detects marrow edema)
- CT useful if MRI unavailable or for assessing comminution
PART 4 - CLINICAL CASE
Case Presentation
A 75-year-old woman with a history of osteoporosis is brought to the Emergency Department by her family after she was found on the floor at home. She reports she heard a "crack" and then fell - note: the fracture may have caused the fall, not the other way around. She cannot bear weight.
Examination:
- Right lower limb is shortened and externally rotated (pathognomonic position)
- Groin pain that worsens with active movement
- Pain on axial loading (heel strike test / telescoping)
- No distal neurovascular deficit
Vitals: BP 130/80, HR 88, afebrile
Step-by-Step Approach
1. What is your immediate differential?
- Femoral neck fracture (most likely)
- Intertrochanteric fracture (also causes shortening + ER)
- Subtrochanteric fracture
- Acetabular fracture
- Pubic ramus fracture (less shortening/ER)
- Hip dislocation (posterior = flexed + IR; anterior = extended + ER - but usually requires high energy in elderly)
2. Investigations
| Investigation | Why |
|---|---|
| AP pelvis + cross-table lateral hip | First-line; classify fracture |
| Full-length femur X-ray | Never miss a distal fracture |
| Bloods: FBC, CMP, coagulation, group & hold | Pre-op workup |
| ECG | Pre-op cardiac assessment |
| MRI hip | If X-ray negative but high suspicion (occult fracture) |
| CT | If MRI unavailable; better for comminution |
3. X-ray shows Garden III subcapital fracture
Now you classify: Intracapsular + displaced = high AVN risk = need arthroplasty
4. Management Decision Tree
Femoral Neck Fracture
│
├─── YOUNG patient (<60 yrs) + any garden grade
│ → URGENT internal fixation (within 6-12 hrs)
│ → Goal: save the femoral head
│ → Cannulated screws or sliding hip screw
│
└─── ELDERLY patient (>60-65 yrs)
│
├─── Undisplaced (Garden I/II)
│ → Internal fixation (cannulated screws)
│ → (some centres use hemiarthroplasty for very elderly)
│
└─── Displaced (Garden III/IV)
│
├─── NOT independently mobile / dementia / limited prognosis
│ → HEMIARTHROPLASTY (cemented preferred in elderly)
│
└─── INDEPENDENTLY MOBILE (walking outdoors before injury)
→ TOTAL HIP ARTHROPLASTY (THA)
→ Better functional outcomes in active elderly
5. Surgical approach considerations
| Procedure | Access | Implant | Notes |
|---|---|---|---|
| Internal fixation | Lateral approach | 3 cannulated cancellous screws (inverted triangle) | Young patients; must achieve anatomic reduction first |
| Dynamic Hip Screw (DHS) | Lateral approach | Barrel + lag screw + side plate | Better for basicervical; not for true subcapital |
| Hemiarthroplasty | Posterolateral or Hardinge (lateral) | Unipolar or bipolar head (Austin-Moore / Thompson / Modern cemented) | Elderly, displaced; cemented = less subsidence |
| Total Hip Arthroplasty | Posterolateral or anterior | Full hip prosthesis | Active elderly; better QoL outcomes |
6. Complications to Know
| Complication | Timing | Mechanism | Prevention/Treatment |
|---|---|---|---|
| Avascular necrosis (AVN) | Months to years | Disruption of retinacular vessels; higher risk Garden III/IV | Prompt fixation in young; arthroplasty in elderly displaced |
| Non-union | 3-6 months | Inadequate fixation, shear forces (high Pauwels), AVN | Good reduction + fixation; salvage with arthroplasty |
| Implant failure / cut-out | Weeks to months | Varus malreduction, osteoporosis, tip-apex distance >25mm | Correct reduction; tip-apex distance |
| Deep vein thrombosis / PE | Days to weeks | Immobility, hypercoagulable state | LMWH chemoprophylaxis + mechanical (TED stockings) |
| Pneumonia / pressure sores | Days | Immobility | Early surgery (<48 hrs) reduces mortality |
| Mortality | 1 year mortality ~20-30% | Multi-morbidity, complications, inactivity | Early surgery (<48 hrs), geriatric co-management |
7. Mortality context (exam favourite):
- 1-year mortality after hip fracture in the elderly is 20-30%
- Surgery within 48 hours significantly reduces mortality
- Hip fracture is managed as a medical emergency, not an elective procedure
Exam Mnemonics
Garden classification memory trick:
"1 = Incomplete valgus; 2 = Complete no displacement; 3 = Complete varus; 4 = Completely gone (displaced)"
Pauwels - the steeper the line, the worse the shear:
"Vertical = Vicious" (Type III with steep vertical fracture is worst)
Leg position in fracture vs dislocation:
- Fracture = Shortened + Externally Rotated (capsule torn, limb collapses into ER)
- Posterior dislocation = Flexed + Internally Rotated + Adducted (FIAD)
- Anterior dislocation = Extended + Externally Rotated + Abducted
Blood supply mnemonic (MFCA is king):
"Medial Femoral Circumflex = Major Flow to Cartilage" - it's the primary supply. Destroy it = AVN.
QUICK-RECALL SUMMARY TABLE
| Topic | Key Fact |
|---|---|
| Longest, strongest bone | Femur |
| Neck-shaft angle | 125-135° (normal) |
| Most important artery to femoral head | Medial femoral circumflex artery (MFCA) |
| Garden I/II | Undisplaced → internal fixation |
| Garden III/IV | Displaced → arthroplasty in elderly |
| Pauwels III | >50° fracture line = most shear = worst prognosis |
| Classic clinical sign of neck fracture | Shortened + externally rotated limb |
| If X-ray normal but suspect fracture | MRI is gold standard |
| Timing for surgery | <48 hours (reduces mortality) |
| 1-year mortality hip fracture | 20-30% in elderly |
| AVN risk (displaced intracapsular) | 15-35% |
| Trendelenburg sign tests | Gluteus medius (superior gluteal nerve) |
| Shenton's line broken | Hip dislocation or fracture |
WHAT'S NEXT (Day 2 suggestion)
Following the natural ortho progression, Day 2 would be:
- Bone: Tibia/Fibula anatomy
- Joint: Knee joint (most complex joint - menisci, cruciate ligaments, collateral ligaments)
- X-ray: Tibial plateau fracture (Schatzker classification)
- Clinical case: 35-year-old motorcyclist, valgus knee injury - tibial plateau fracture
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Rockwood and Green's Fractures in Adults 10th Ed 2025 | Grainger & Allison's Diagnostic Radiology | THIEME Atlas of Anatomy - General Anatomy & Musculoskeletal System | Rosen's Emergency Medicine
These notes are structured the same way every day will follow: anatomy first, then joint mechanics, then X-ray interpretation with classification systems, then clinical case with management algorithm. By Day 30 you will have covered every major bone-joint-fracture complex in orthopaedics. Say "Day 2" whenever you are ready to continue, or ask for any clarification on today's material.
This is a shared conversation. Sign in to Orris to start your own chat.