Metastasis and routes of metastasis
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the core content needed. Let me compile the comprehensive answer.
Metastasis and Routes of Metastasis
Definition
Metastasis is the spread of a primary tumor to physically discontinuous sites - a process that unequivocally marks a tumor as malignant. Approximately 30% of solid tumors present with clinically evident metastases at diagnosis, and an additional 20% have occult (microscopic) metastases at that time.
Not all malignant tumors metastasize with equal frequency. Gliomas of the CNS and basal cell carcinomas of the skin invade locally but rarely metastasize, demonstrating that invasiveness and metastatic potential are separable properties.
Routes of Metastatic Spread
Cancers disseminate through three main pathways:
1. Seeding of Body Cavities and Surfaces
Occurs when tumor cells spread into a natural "open field" lacking physical barriers.
- Most common site: Peritoneal cavity
- Other cavities: Pleura, pericardium, meninges, joints
- Classic example: Ovarian carcinoma - cells spread widely over peritoneal surfaces, often coating the omentum without deeply invading the underlying tissue
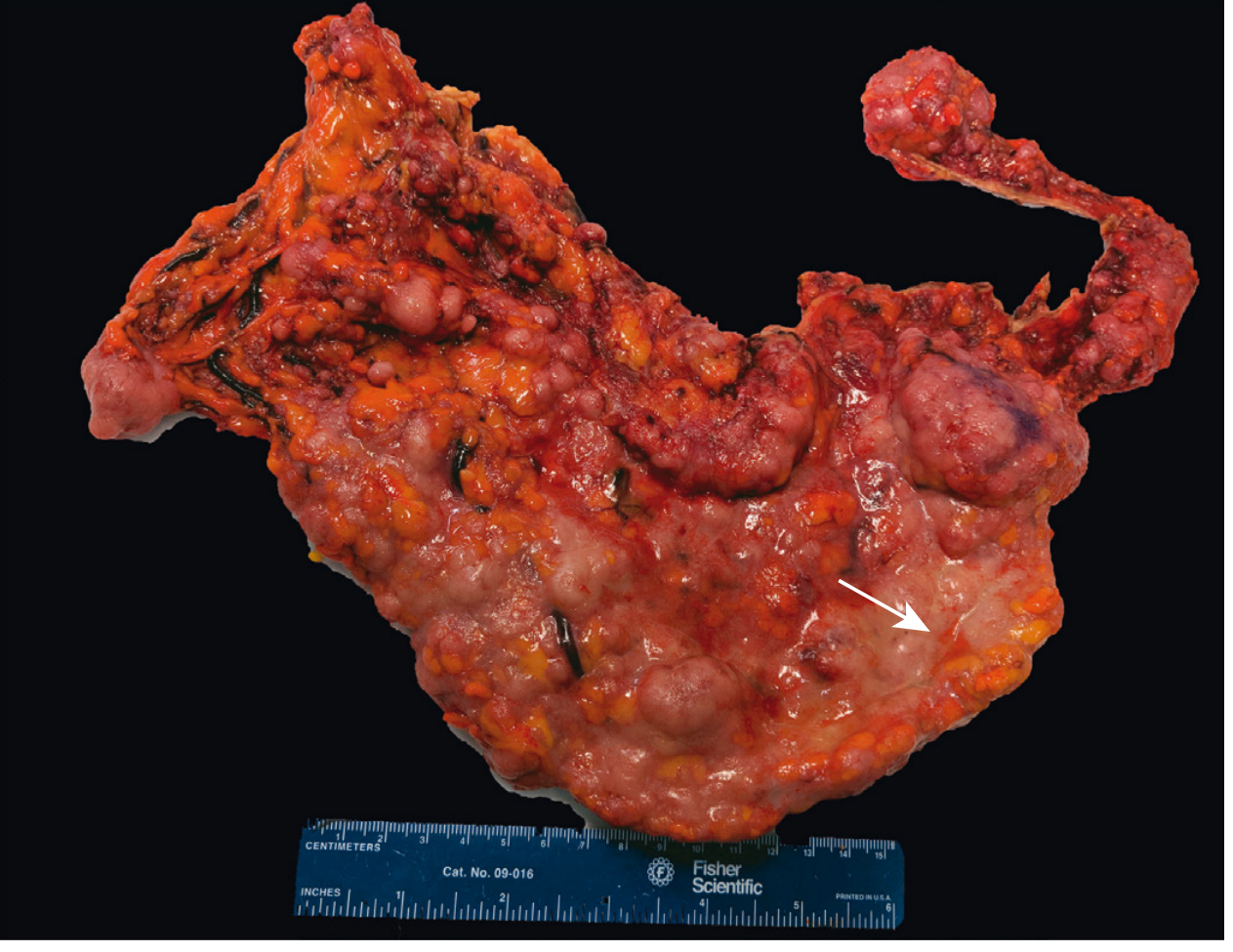
Involvement of omentum by metastatic ovarian carcinoma - Robbins Pathologic Basis of Disease
- Pseudomyxoma peritonei: When mucus-secreting appendiceal or ovarian carcinomas fill the peritoneal cavity with a gelatinous neoplastic mass
- CNS example: Medulloblastoma or ependymoma can penetrate cerebral ventricles and seed meningeal surfaces via cerebrospinal fluid
2. Lymphatic Spread
The most common initial pathway for dissemination of carcinomas (epithelial malignancies). Sarcomas occasionally also use this route.
Key points:
- Tumors do not have functional lymphatic vessels internally; the vessels at the margins of the invading tumor are sufficient
- Spread follows natural lymphatic drainage patterns
- Example: Breast carcinoma (upper outer quadrant) → axillary nodes → infraclavicular/supraclavicular nodes
- Example: Lung carcinoma → perihilar tracheobronchial → mediastinal nodes
- Skip metastasis: Local nodes can be bypassed, possibly due to variation in drainage patterns or anastomoses
Sentinel lymph node biopsy exploits this orderly spread: the first draining node is biopsied (using radiolabeled tracers or colored dyes) to guide surgical management in breast cancer and melanoma.
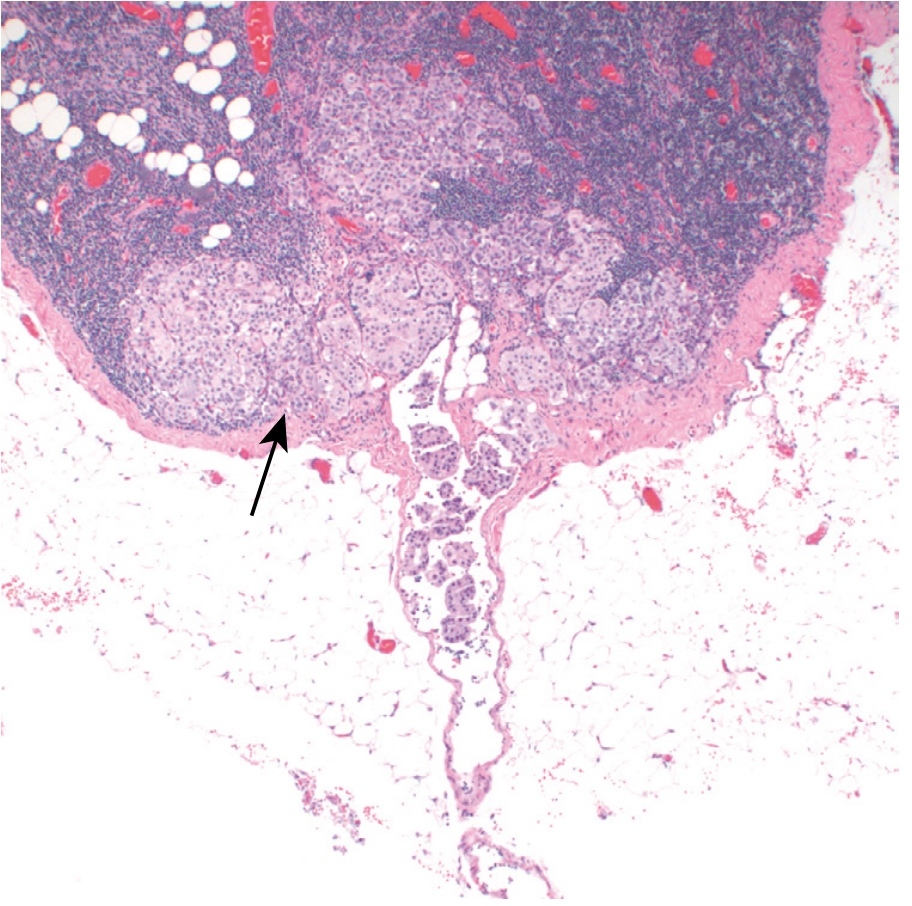
Axillary lymph node with metastatic breast carcinoma - Robbins Pathologic Basis of Disease
3. Hematogenous Spread
Preferred route for sarcomas (mesenchymal tumors); carcinomas also use this route (e.g., renal cell carcinoma, hepatocellular carcinoma).
Key principles:
- Arteries are harder to penetrate due to thicker walls; veins are more vulnerable
- Tumor cells preferentially follow venous drainage:
- Portal vein drainage → liver (GI and pancreatic primaries)
- Caval drainage → lungs
- The liver and lungs are therefore the most common sites of hematogenous metastasis
- Some tumors show organ tropism (e.g., prostate cancer → bone, breast cancer → bone/brain/liver/lungs) due to specific receptor-ligand interactions
The Metastatic Cascade (Step-by-Step)
The cascade is divided into two phases: (1) Invasion of the ECM and (2) Vascular dissemination, homing, and colonization.
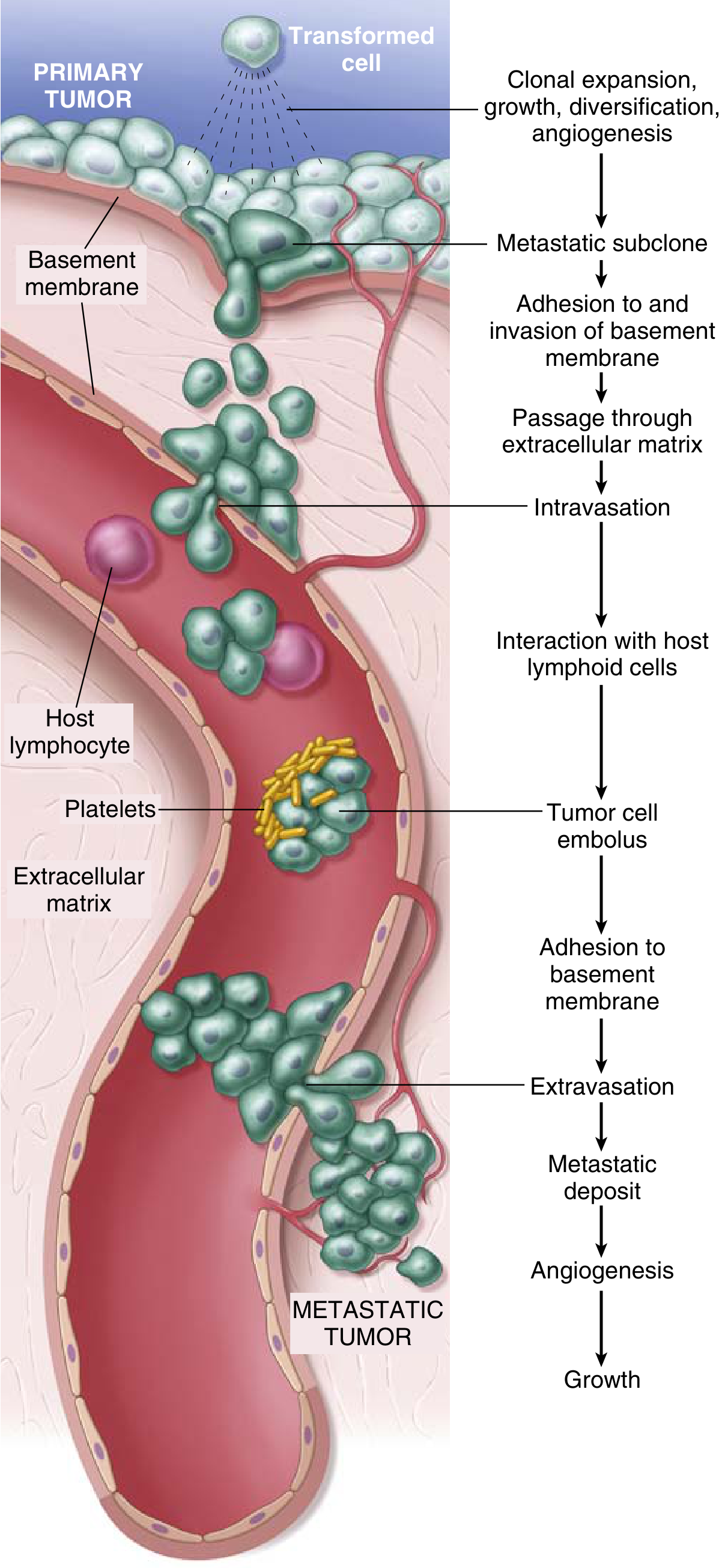
The Metastatic Cascade - Robbins & Kumar Basic Pathology
Phase 1 - Invasion of the Extracellular Matrix (ECM)
The ECM consists of basement membranes and interstitial connective tissue. A carcinoma cell must breach the basement membrane, traverse the interstitial connective tissue, and gain access to the circulation.
Step A: Loosening of intercellular junctions
- Normally, E-cadherins hold epithelial cells tightly together and relay anti-growth signals via β-catenin
- In many epithelial cancers, E-cadherin function is lost through:
- Mutational inactivation of E-cadherin genes
- Transcriptional silencing by SNAIL and TWIST transcription factors
- This process is called Epithelial-Mesenchymal Transition (EMT) - cells downregulate epithelial markers (E-cadherin) and upregulate mesenchymal markers (vimentin, smooth muscle actin), acquiring a promigratory phenotype
Step B: Degradation of ECM
- Tumor cells secrete proteolytic enzymes or induce stromal cells (fibroblasts, macrophages) to do so
- Key proteases involved:
- Matrix metalloproteinases (MMPs) - especially MMP9 (type IV collagenase)
- Cathepsin D
- Urokinase plasminogen activator
- MMPs not only degrade ECM but also release sequestered growth factors (e.g., VEGF)
Step C: Migration and invasion
- Tumor cells bind to the remodeled ECM via altered integrin expression
- Cells migrate along new ECM binding sites, guided by chemotactic factors from inflammatory and stromal cells
- Actin filament assembly drives directional movement
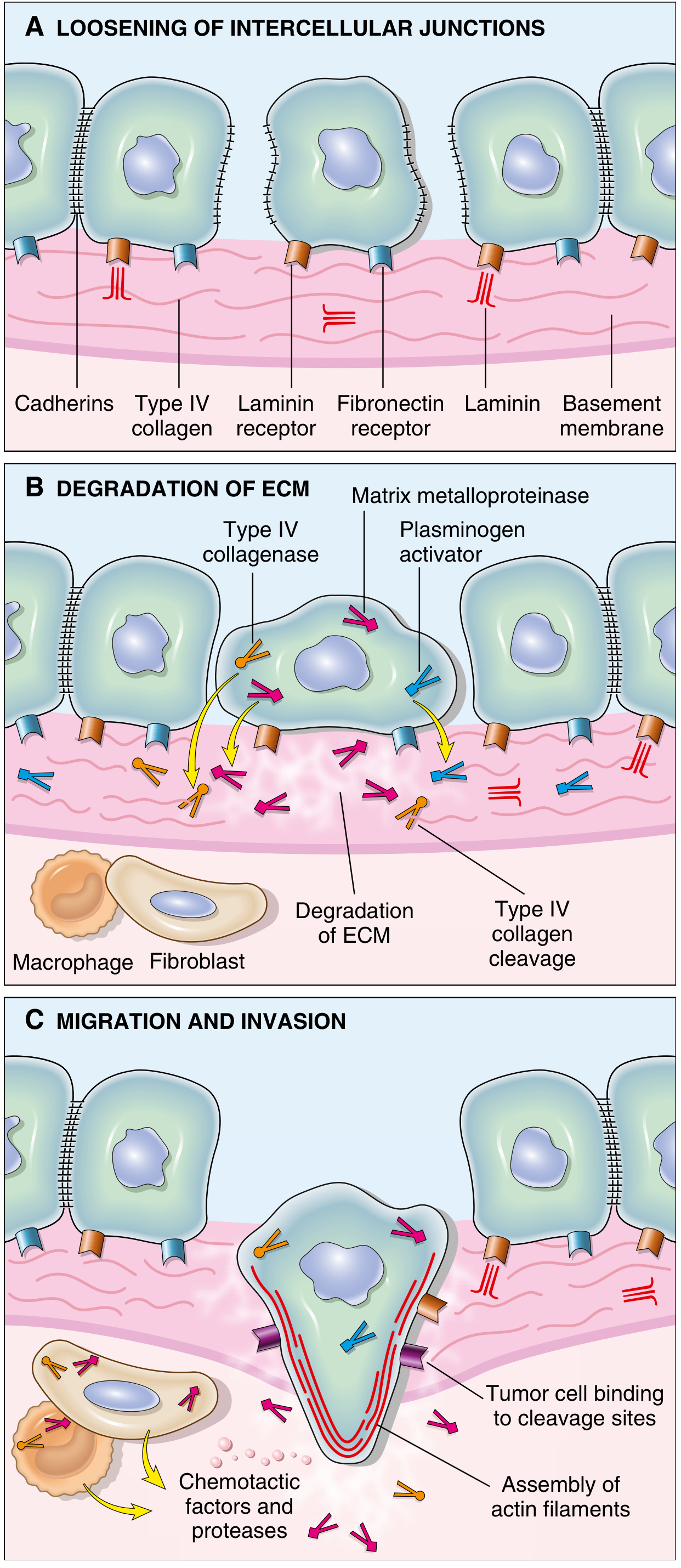
Steps in basement membrane invasion - Robbins & Kumar Basic Pathology
Phase 2 - Vascular Dissemination, Homing, and Colonization
| Step | Description |
|---|---|
| Intravasation | Tumor cells penetrate blood vessel or lymphatic walls |
| Survival in circulation | Cells must evade shear stress, NK cells, and immune surveillance; tumor cells often form emboli with platelets and leukocytes for protection |
| Arrest and extravasation | Circulating tumor cells arrest in capillaries by size or specific adhesion; they re-express adhesion molecules to adhere to endothelium, then extravasate by the same ECM-degradation mechanism |
| Micrometastasis formation | Cells form a small deposit at the distant site |
| Colonization | Micrometastases grow into macroscopic tumors - requires angiogenesis, evasion of local immunity, and adaptation to new microenvironment |
Why is metastasis so inefficient? Despite millions of tumor cells entering the blood daily, very few produce metastases. This is because the process is multistep - each stage requires overcoming immune defenses and adapting to a foreign microenvironment. No single "metastasis gene" has been found; the metastatic phenotype likely requires cumulative genetic and epigenetic changes.
Organ Tropism - "Seed and Soil" Hypothesis
(Proposed by Stephen Paget, 1889)
The site of metastasis is not always determined purely by blood flow patterns. Some tumors show preferential spread to specific organs:
| Primary Tumor | Common Metastatic Sites |
|---|---|
| Breast | Bone, lungs, liver, brain, adrenals |
| Lung | Brain, adrenals, liver, bone |
| Prostate | Bone (osteoblastic) |
| Kidney | Lung, liver, bone, brain |
| Colon | Liver (portal drainage), lungs |
| Thyroid (follicular) | Bone, lungs |
| Choriocarcinoma | Lungs |
| Neuroblastoma | Liver, bone marrow |
This organ specificity is explained by:
- Organ-specific adhesion molecules and chemokine receptors on tumor cells matching ligands on target organ endothelium (e.g., CXCR4 on breast cancer cells, CXCL12/SDF-1 in bone marrow)
- The local microenvironment (soil) supporting or inhibiting tumor growth
Summary Table: Routes of Metastasis
| Route | Tumor Types | Common Pattern | Example |
|---|---|---|---|
| Lymphatic | Carcinomas (mainly) | Follows regional lymph drainage | Breast → axillary nodes |
| Hematogenous | Sarcomas (primarily); also carcinomas | Follows venous drainage | Colorectal → liver via portal vein |
| Body cavity seeding | Carcinomas invading serous surfaces | Peritoneal/pleural spread | Ovarian → peritoneum |
| Transcoelemic (CSF) | CNS tumors | Via cerebrospinal fluid | Medulloblastoma → spinal cord |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528); Robbins & Kumar Basic Pathology (9780323790185)
This is a shared conversation. Sign in to Orris to start your own chat.