CKD
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"chronic kidney disease"[MeSH Terms] AND classification
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have excellent, comprehensive data from authoritative textbooks. Let me compose the full overview.
Chronic Kidney Disease (CKD) - Overview
Definition
CKD is defined as kidney damage or decreased kidney function persisting for 3 months or more, regardless of cause. The two core criteria are:
- GFR < 60 mL/min/1.73 m² - present for ≥3 months, with or without other markers of kidney damage
- Markers of kidney damage (even with normal GFR) - including proteinuria/albuminuria, abnormal urine sediment, electrolyte abnormalities from tubular disorders, abnormal renal histology, or structural abnormalities on imaging
For G1 and G2 stages (GFR ≥60), additional evidence of kidney damage must be present for a diagnosis of CKD to be made.
- Comprehensive Clinical Nephrology, 7th Ed., p. 2133
- Washington Manual of Medical Therapeutics, p. 498
KDIGO 2012 Staging System
The current classification uses three dimensions: cause, GFR category (G), and albuminuria category (A).
GFR Categories (G Stages)
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Normal or high | ≥90 |
| G2 | Mildly decreased | 60–89 |
| G3a | Mildly to moderately decreased | 45–59 |
| G3b | Moderately to severely decreased | 30–44 |
| G4 | Severely decreased | 15–29 |
| G5 | Kidney failure | <15 |
G5 also includes patients on dialysis (G5D).
Albuminuria Categories (A Stages)
| Category | Description | Urine ACR |
|---|---|---|
| A1 | Normal to mildly increased | <30 mg/g |
| A2 | Moderately increased | 30–300 mg/g |
| A3 | Severely increased | >300 mg/g |
KDIGO Heat Map - Risk of CKD Progression
The numbers (1-4+) in the table below indicate visits per year recommended and reflect relative risk of progression (green = low risk, yellow = moderate, orange = high, red = very high):
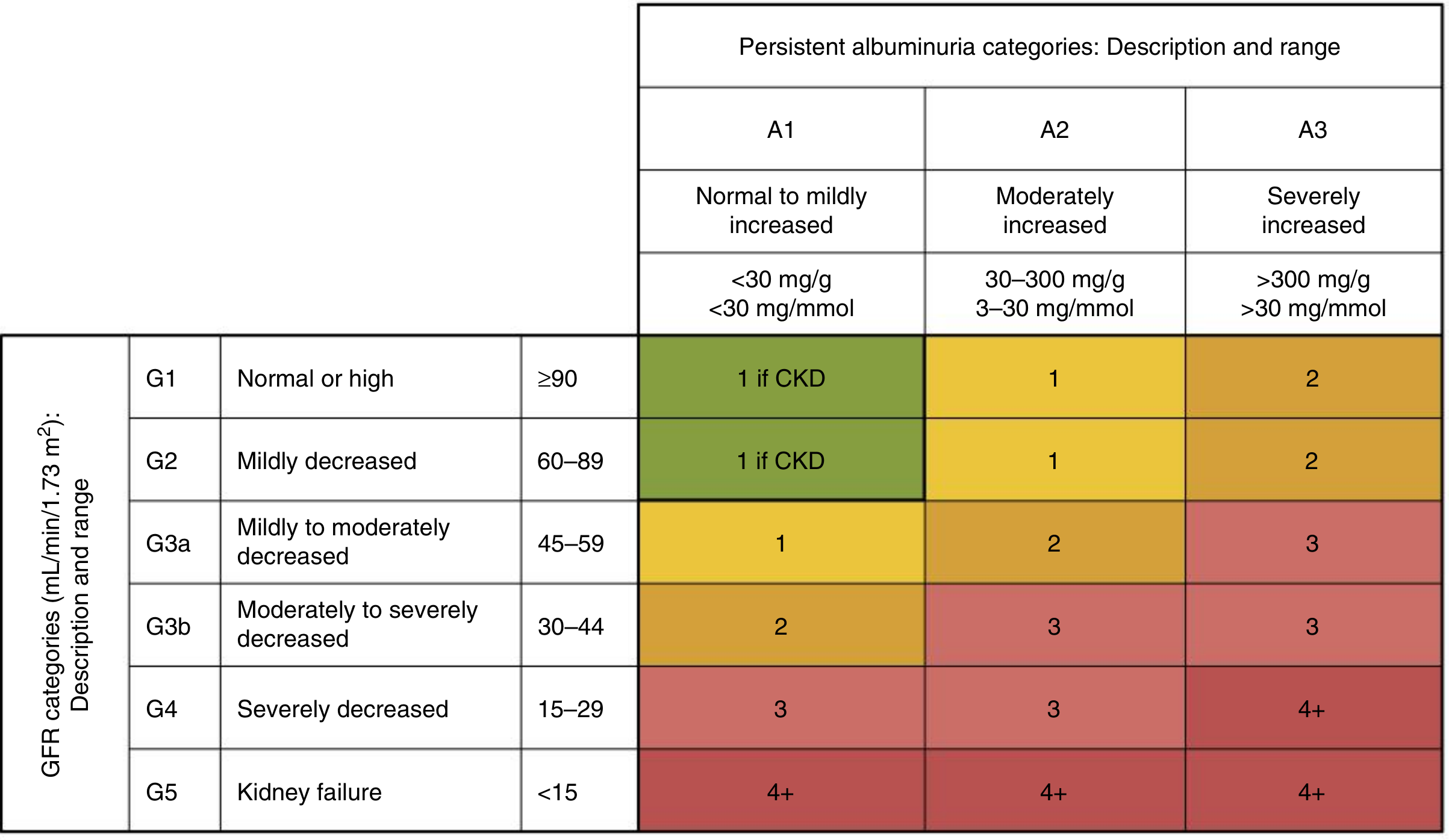
The heat map highlights a key principle: albuminuria independently amplifies risk at any GFR stage. A patient at G3a/A3 carries substantially higher risk than one at G3a/A1.
- Comprehensive Clinical Nephrology, 7th Ed., p. 2138
Estimating GFR
The preferred equations are:
- CKD-EPI (Creatinine) - best available in North America; uses serum creatinine, age, and sex
- CKD-EPI (Creatinine + Cystatin C) - most accurate when both markers are available
- MDRD - widely used historically; performs well but tends to underestimate GFR at higher levels
- Cockcroft-Gault - still used for drug dosing adjustments
Serum creatinine alone is an inadequate marker - even "normal" creatinine can correspond to significantly reduced GFR depending on age, sex, and muscle mass.
- Textbook of Family Medicine, 9e, p. 1192
Epidemiology
-
CKD affects approximately 10-15% of the global adult population
-
In the US, roughly 20 million people have CKD
-
Half of all Americans are expected to develop CKD at some point during their lifetime
-
It is a leading cause of mortality worldwide and carries immense healthcare costs, particularly at kidney failure stage
-
Comprehensive Clinical Nephrology, 7th Ed., p. 2130
Causes
The most common causes of CKD in adults globally are:
Primary causes (accounting for ~2/3 of cases)
- Diabetic nephropathy (diabetic kidney disease) - single leading cause, ~40% of incident cases in high-income countries
- Hypertensive nephrosclerosis / renovascular disease - second most common
- Glomerulonephritis (IgA nephropathy, focal segmental glomerulosclerosis [FSGS], lupus nephritis, membranous nephropathy, MPGN)
Other important causes
- Polycystic kidney disease (PKD) and other inherited disorders
- Obstructive uropathy (chronic obstruction from stones, BPH, etc.)
- Recurrent pyelonephritis / chronic interstitial nephritis
- HIV-associated nephropathy
- Analgesic/NSAID nephropathy
- Contrast or drug-induced nephrotoxicity progressing to CKD
In children
Causes differ markedly from adults - congenital anomalies of the kidney and urinary tract (CAKUT), renal dysplasia, reflux nephropathy, and glomerular diseases predominate.
- NKF Primer on Kidney Diseases, 8e
- Campbell-Walsh-Wein Urology, 5th ed.
Risk Factors for Progression
- Non-modifiable: older age, male sex, race/ethnicity, genetic variants (e.g., APOL1 in individuals of African ancestry), low birth weight/reduced nephron number
- Modifiable: poorly controlled diabetes, hypertension, proteinuria, obesity, smoking, high protein intake, nephrotoxin exposure, recurrent AKI episodes, chronic NSAID use
Key Points
| Feature | Detail |
|---|---|
| Duration criterion | ≥3 months |
| Main GFR stages | G1–G5 (subdivided G3a/G3b) |
| Main albuminuria stages | A1–A3 |
| Best GFR estimating equation | CKD-EPI Cr or CKD-EPI Cr+CysC |
| Leading cause in adults | Diabetic kidney disease |
| Refer to nephrology | GFR <30 (Stage G3b+) |
| Prepare for RRT | Stage G4 onward |
Would you like to go deeper into any specific aspect - pathophysiology, complications (anemia, CKD-MBD, acidosis), or management?
This is a shared conversation. Sign in to Orris to start your own chat.