Explain me about Mi . it's egc and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed answer.
Myocardial Infarction (MI): Overview, ECG Changes, and Treatment
Definition
MI (heart attack) is the death of cardiac muscle due to prolonged ischemia - when blood supply to part of the myocardium is interrupted long enough to cause irreversible cell necrosis. Roughly 800,000 Americans experience an MI each year (nearly one every 40 seconds), causing ~400,000 deaths annually. The vast majority are caused by atherosclerosis.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis
The typical sequence of events:
- An atheromatous plaque is eroded or disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces - exposing subendothelial collagen and necrotic plaque contents to blood.
- Platelets adhere, aggregate, and activate - releasing thromboxane A₂, ADP, and serotonin, causing further aggregation and vasospasm.
- Activation of coagulation via tissue factor adds to the growing thrombus.
- Within minutes, the thrombus can completely occlude the coronary artery lumen.
When angiography is performed within 4 hours of MI onset, it demonstrates coronary thrombosis in ~90% of cases. This sequence has direct therapeutic implications: early thrombolysis and/or angioplasty can dramatically limit myocardial necrosis. - Robbins, Cotran & Kumar
Non-atherothrombotic causes (~10%): vasospasm (cocaine, ephedrine), embolism (from mural thrombus, endocarditis vegetations, atrial fibrillation), vasculitis, sickle cell disease, amyloid deposition.
Types of MI by Extent

| Type | Mechanism | Result |
|---|---|---|
| Transmural (STEMI) | Complete occlusion of an epicardial vessel | Full-thickness LV wall necrosis in distribution of affected artery |
| Subendocardial (NSTEMI) | Partial/transient occlusion, or thrombus that lyses before full-thickness necrosis | Necrosis confined to inner 1/3-1/2 of wall; regional or circumferential |
| Microinfarcts | Small intramural vessel occlusion (vasculitis, embolism, cocaine) | Scattered small foci of necrosis |
Coronary Artery Territory:
-
LAD (Left Anterior Descending) - anterior LV wall, anterior septum (most common; "widow maker")
-
LCx (Left Circumflex) - lateral and posterior LV wall
-
RCA (Right Coronary Artery) - inferior LV wall, posterior septum, RV
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
ECG Changes in MI
The three major electrical abnormalities underlying ECG changes in acute MI are:
| Defect in Infarcted Cells | Current Flow Direction | ECG Change in Overlying Leads |
|---|---|---|
| Rapid repolarization (accelerated K⁺ channel opening) | Out of infarct | ST segment elevation |
| Decreased resting membrane potential (loss of intracellular K⁺) | Into infarct | TQ depression (manifested as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
Serial ECG Evolution in Anterior MI:
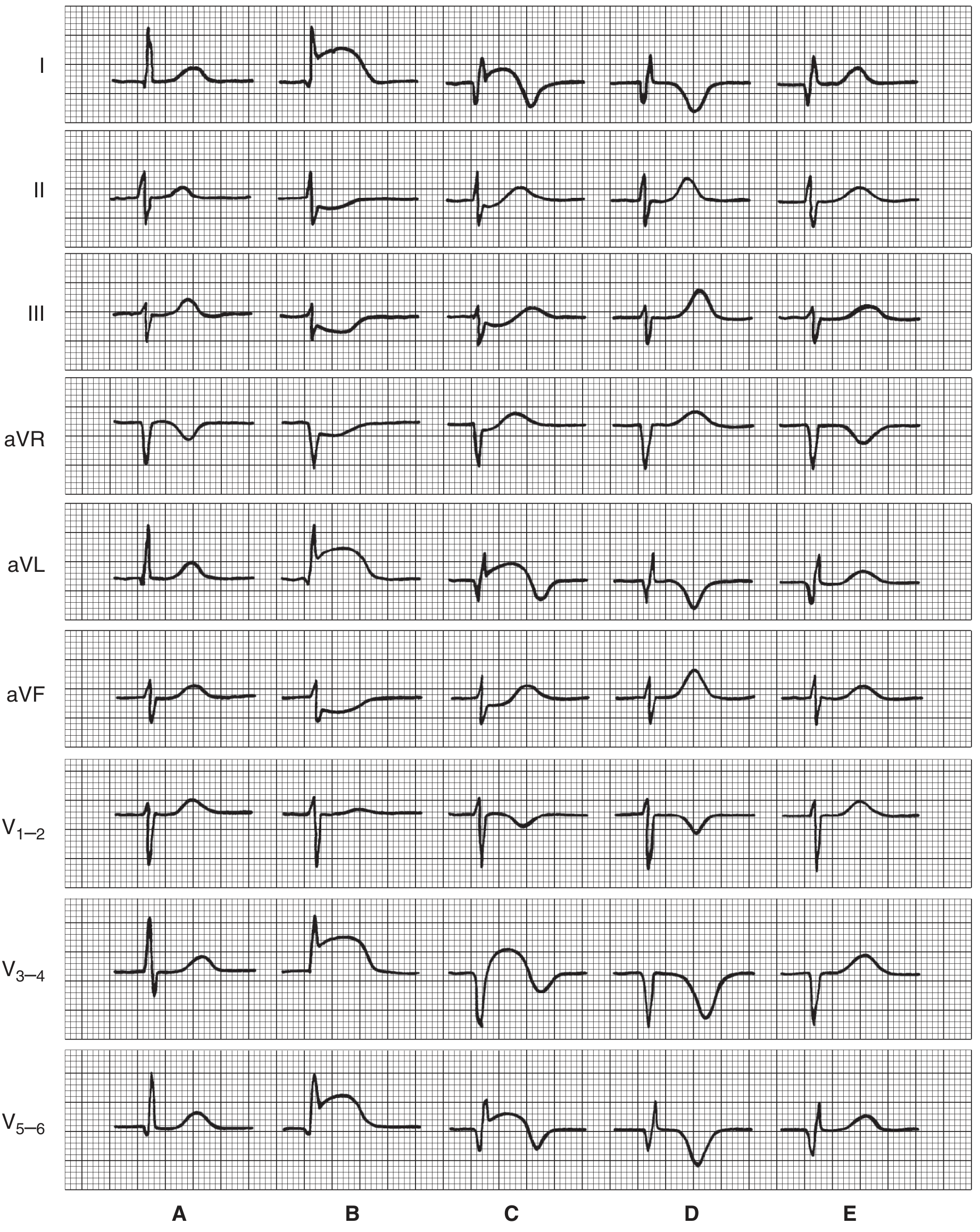
- A - Normal tracing: Baseline
- B - Very early (hours after infarction): ST segment elevation in leads I, aVL, V3-5; reciprocal ST depression in leads II, III, aVF
- C - Later (hours to days): Q waves appear in I, aVL, V5-6; QS complexes in V3-4 (transmural necrosis); ST changes persist but lessen; T waves begin to invert
- D - Days to weeks: Deep T wave inversions; Q waves become more prominent
- E - Weeks to months: Q waves stabilize; T waves may normalize or remain inverted; "electrically silent" scar
Lead Localisation of STEMI:
| Infarct Location | ECG Leads Showing ST Elevation | Artery Involved |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Anterolateral | V1-V6, I, aVL | LAD or LCx |
| Inferior | II, III, aVF | RCA (or LCx) |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | Tall R in V1, reciprocal ST depression V1-V2 | RCA or LCx |
| Right ventricular | ST elevation in V4R | RCA (proximal) |
Other Key ECG Points:
-
Reciprocal changes: Leads on the opposite side of the heart show ST depression.
-
Q waves: Develop after some days/weeks - electrically silent dead muscle/scar. Abnormal Q = >40ms wide or >25% depth of R wave. Non-Q-wave infarcts tend to be less severe but have high risk of reinfarction.
-
Arrhythmias: Common in 3 phases - (1) 0-30 min post-infarction: reentry arrhythmias; (2) relative quiet period; (3) 12h onwards: increased automaticity; (4) 3 days to weeks: reentry again. Risk of ventricular fibrillation is highest.
-
NSTEMI/UA: No ST elevation; may show ST depression, T-wave inversions, or a normal ECG; diagnosis requires elevated troponin (NSTEMI) vs. normal troponin (UA).
-
Ganong's Review of Medical Physiology, 26th Ed.
Biomarkers
| Biomarker | Rises | Peaks | Normalises |
|---|---|---|---|
| Troponin I/T (most sensitive/specific) | 3-6 hrs | 24-48 hrs | 5-14 days |
| CK-MB | 3-6 hrs | 24 hrs | 48-72 hrs |
| Myoglobin | 1-4 hrs (earliest) | 6-12 hrs | 24 hrs |
Treatment
Immediate (Acute) Management - MONA + Reperfusion
General measures:
- Morphine - for pain relief (reduces sympathetic drive, preload; use cautiously)
- Oxygen - for O₂ sat <94% (routine use no longer recommended for all patients)
- Nitrates (sublingual nitroglycerin) - for pain relief and vasodilation; contraindicated in hypotension or RV infarction
- Aspirin (162-325mg, chewed) - immediate antiplatelet effect; reduces mortality
Reperfusion Therapy - The Priority in STEMI
Primary PCI (Percutaneous Coronary Intervention) is the treatment of choice when available:
- Goal: door-to-balloon time <90 minutes
- Superior to thrombolysis when performed in a timely manner at a PCI-capable centre
- Mechanical restoration of flow with balloon angioplasty ± stent
Thrombolytic (Fibrinolytic) Therapy - when PCI is not available within 120 min:
- Agents: streptokinase, alteplase (tPA), tenecteplase, reteplase
- Most effective within the first 3 hours ("golden hour")
- Contraindicated if systolic BP >185 mmHg or diastolic >110 mmHg persistently
- Contraindicated in recent stroke, active bleeding, recent major surgery
Antiplatelet and Antithrombotic Therapy
- Dual antiplatelet therapy (DAPT): Aspirin + a P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel) - continued for 12 months post-ACS
- Anticoagulation: Heparin (UFH or LMWH), bivalirudin, or fondaparinux - used acutely to prevent further thrombosis
Additional Pharmacotherapy
| Drug Class | Examples | Indication |
|---|---|---|
| Beta-blockers | Metoprolol, carvedilol | Reduce heart rate/O₂ demand; reduce arrhythmias; improve survival |
| ACE inhibitors / ARBs | Lisinopril, ramipril | Post-MI with reduced EF; reduce remodelling; start within 24h |
| High-intensity statin | Atorvastatin 80mg, rosuvastatin 40mg | Plaque stabilisation; reduce recurrence; start immediately |
| Aldosterone antagonist | Eplerenone, spironolactone | For EF <40% + HF or diabetes post-MI |
| P2Y12 inhibitors | Ticagrelor, clopidogrel | Dual antiplatelet therapy |
Summary of In-Hospital Treatment (Fuster's Heart, 15th Ed.):
"Hospitalized patients should be treated with ASA, a platelet P2Y12 receptor inhibitor, antithrombotic therapy, a beta-blocker, an ACE inhibitor, and a high-intensity statin."
Long-term / Secondary Prevention
- Continue DAPT for 12 months
- Lifelong aspirin + statin + ACE inhibitor (if EF reduced)
- Beta-blocker (especially if EF <40%)
- Cardiac rehabilitation
- Risk factor control: smoking cessation, BP and diabetes management, diet, exercise
- ICD implantation if EF remains <35% despite >3 months of optimal medical therapy
Complications of MI
| Complication | Timing | Notes |
|---|---|---|
| Arrhythmias (VF, VT) | Hours | Most common cause of early death |
| Cardiogenic shock | Hours-days | Pump failure; needs urgent PCI |
| Papillary muscle rupture | 2-7 days | Acute mitral regurgitation |
| Free wall rupture | 3-7 days | Cardiac tamponade; often fatal |
| Ventricular septal defect | 3-7 days | Acquired VSD; new harsh murmur |
| Left ventricular aneurysm | Weeks-months | Persistent ST elevation; mural thrombus |
| Dressler's syndrome | Weeks-months | Autoimmune pericarditis |
| Heart failure | Acute/chronic | Systolic dysfunction |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Pathogenesis, morphology, types
- Ganong's Review of Medical Physiology, 26th Ed. - ECG mechanisms, serial changes, arrhythmias
- Fuster and Hurst's The Heart, 15th Ed. - ACS management, pharmacotherapy
- Goldman-Cecil Medicine - Classification, treatment framework
This is a shared conversation. Sign in to Orris to start your own chat.