Treatment for HOCM.
Reading File
Finding Sources
Searching PubMed
hypertrophic obstructive cardiomyopathy treatment
Searching the Web
HOCM treatment guidelines 2024 2025
Finding Sources
Reading Web Page
https://www.acc.org/latest-in-cardiology/ten-points-to-remem…
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from Harrison's 22E (2025) and the 2024 AHA/ACC guideline context. Here is the full answer:
Treatment of HOCM (Hypertrophic Obstructive Cardiomyopathy)
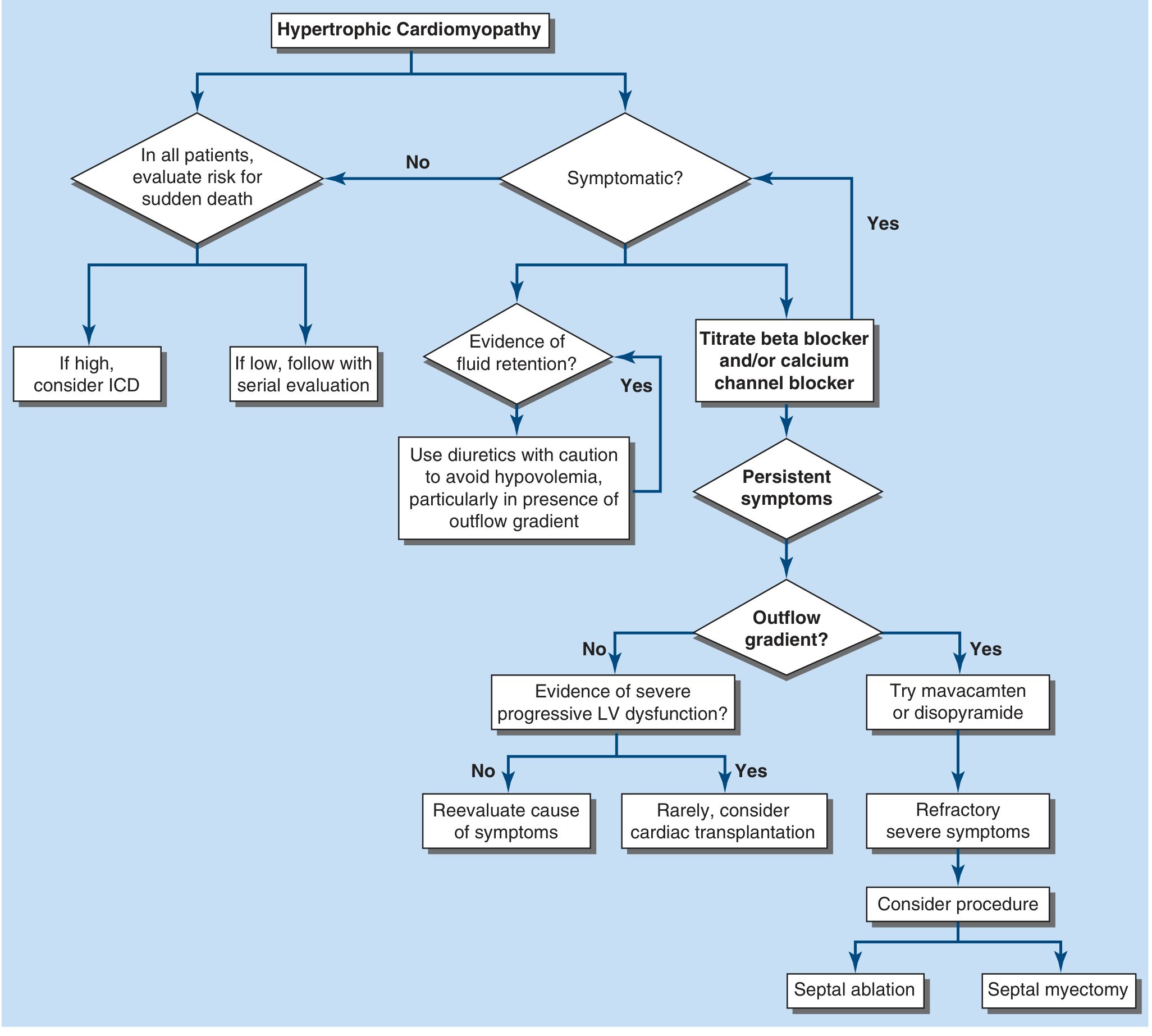
Treatment algorithm for HCM based on symptoms and outflow gradient - Harrison's Principles of Internal Medicine 22E
General Principles
All patients with HOCM should be evaluated for:
- Risk of sudden cardiac death (SCD) - regardless of symptoms
- Symptomatic status - guides step-up therapy
- Atrial fibrillation - common complication requiring specific management
1. Medical Management
First-Line: Negative Chronotropes/Inotropes
| Drug Class | Agents | Mechanism |
|---|---|---|
| Non-vasodilating beta-blockers | Metoprolol, atenolol, propranolol | Slow HR, reduce contractility, enhance diastolic filling |
| Calcium channel blockers (L-type) | Verapamil | Slow HR, reduce obstruction |
- These reduce LVOT obstruction by decreasing HR (lengthening diastolic filling time) and reducing contractility.
- Avoid vasodilators (nitrates, ACE inhibitors, dihydropyridine CCBs) - they worsen obstruction by reducing preload/afterload.
Second-Line: Persistent Symptoms with Outflow Gradient
Disopyramide - a class IA antiarrhythmic with potent negative inotropic properties. Add to a beta-blocker or verapamil when symptoms persist despite first-line therapy.
Novel Agent: Cardiac Myosin Inhibitor
Mavacamten (FDA-approved, 2022) - a first-in-class small-molecule cardiac myosin inhibitor that directly targets the pathophysiologic mechanism of HCM (hypercontractility). Indicated for symptomatic obstructive HCM, including patients with persistent symptoms despite beta-blocker and/or disopyramide therapy. A 2025 meta-analysis confirmed its high efficacy at reducing LVOT gradients and improving symptoms (PMID: 39988344).
- Aficamten is another cardiac myosin inhibitor under active investigation showing similar efficacy.
2024 AHA/ACC guideline update (reaffirmed May 2025): Mavacamten is now formally positioned in the treatment algorithm for symptomatic obstructive HCM. The guideline was reaffirmed as current.
Diuretics
For patients with fluid retention/venous congestion (with or without obstruction), cautious use of diuretics is appropriate - but avoid hypovolemia, which worsens LVOT obstruction.
2. Septal Reduction Therapy (SRT)
Reserved for ~5% of patients with severe, medically refractory symptoms. Both procedures are roughly equivalent in gradient reduction.
A. Surgical Septal Myectomy (Morrow Procedure)
- Gold standard, developed 60+ years ago
- Excises part of the septal myocardium causing dynamic obstruction
- Perioperative mortality is very low at experienced centers
- Excellent long-term survival free of recurrent obstruction
- Mitral regurgitation (due to SAM) usually resolves without separate MV repair
- Preferred for younger patients, those with complex anatomy, or concomitant cardiac lesions
B. Alcohol Septal Ablation (ASA)
- Controlled infarction of the proximal septum via selective injection of ethanol into a septal perforator artery
- Requires suitable coronary anatomy (a large septal perforator)
- Comparable peri-procedural outcomes and gradient reduction to myectomy
- Reserved for patients who wish to avoid surgery or have significant comorbidities
- Common complication of both SRT: Complete heart block requiring permanent pacemaker
Note: Ventricular pacing alone as primary therapy for obstruction is ineffective and not recommended.
3. Prevention of Sudden Cardiac Death
SCD risk is ~0.5%/year baseline. ICD implantation is indicated for:
- Class I (definite): Prior cardiac arrest or sustained VT
- Class IIa (reasonable): 1+ major risk factors (see below)
Major SCD risk factors:
- Prior cardiac arrest or sustained VT
- Unexplained syncope (especially exertional)
- Family history of SCD
- LV wall thickness >30 mm
- LV apical aneurysm
- LV systolic dysfunction (EF <50%)
The ESC HCM Risk-SCD calculator (continuous variables: LVOT gradient, LA diameter, max wall thickness, age, syncope, family history, NSVT) gives a 5-year risk estimate:
- ≥6%: ICD generally advised
- 4-6%: ICD may be considered
- <4%: ICD not advised
4. Atrial Fibrillation Management
- Rate control: beta-blockers, verapamil, or diltiazem
- Rhythm control: disopyramide + rate-control agent, or amiodarone
- Anticoagulation: Recommended for stroke prevention (HCM patients are at elevated thromboembolic risk regardless of CHA₂DS₂-VASc score)
5. Lifestyle Considerations
Historically, vigorous exercise and competitive sports were prohibited. However, recent data have not identified a clear link between exertion and ventricular arrhythmias in HCM, and the 2024 AHA/ACC guideline supports shared decision-making about activity levels rather than blanket restriction.
What to Avoid in HOCM
| Drug/Intervention | Reason |
|---|---|
| Nitrates, hydralazine | Reduce preload → worsen obstruction |
| Dihydropyridine CCBs (nifedipine, amlodipine) | Vasodilation → worsen obstruction |
| Digoxin | Positive inotropy → worsen obstruction |
| High-dose diuretics | Hypovolemia → worsen obstruction |
| Vasopressors (dopamine/dobutamine) | Inotropic, worsen obstruction |
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 2051; 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for Management of HCM (reaffirmed May 2025); Aman A et al., Open Heart 2025 (PMID 39988344) - systematic review of mavacamten/aficamten.
This is a shared conversation. Sign in to Orris to start your own chat.